Locating entrance - managing blockage
29/12/2023
Mohamad Zaafrany
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Narrow canal is a great challenge to Endodontist, When combined with calcified entrance the difficulty doubled.
Preoperative assessment to the periapical radiograph would help in avoiding many errors that could happen if case is underestimated.
CBCT has a great role in assessment and planning for management of canal calcification and blockage and it’s considered of great importance
In this article we’ll describe how we overcome the challenge using the correct technique and the right tools.
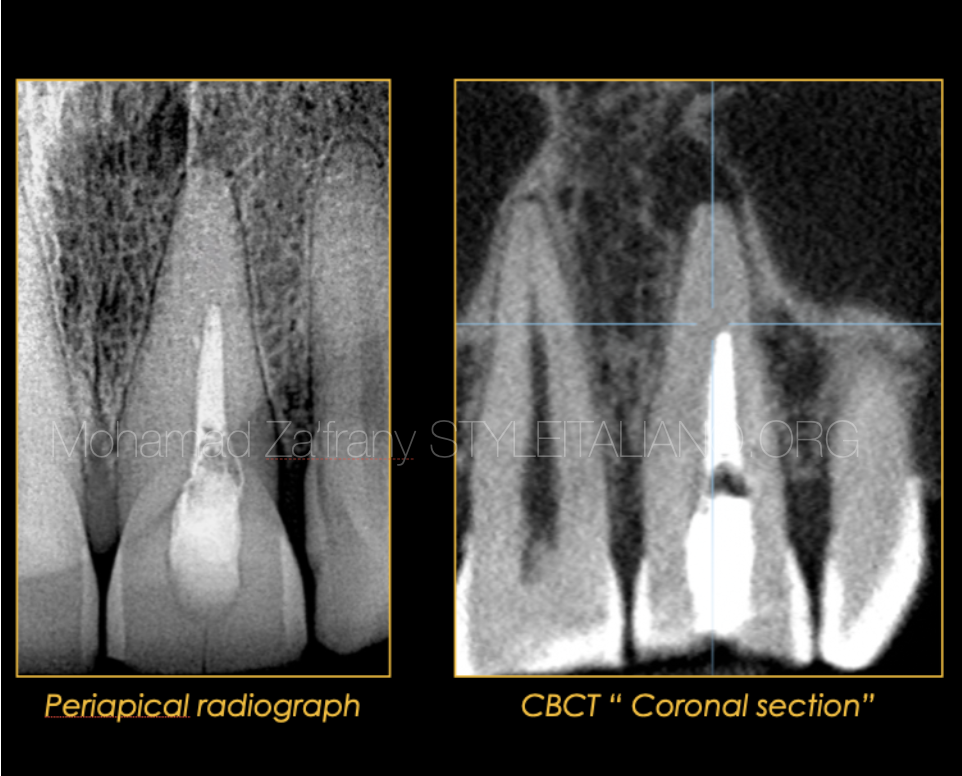
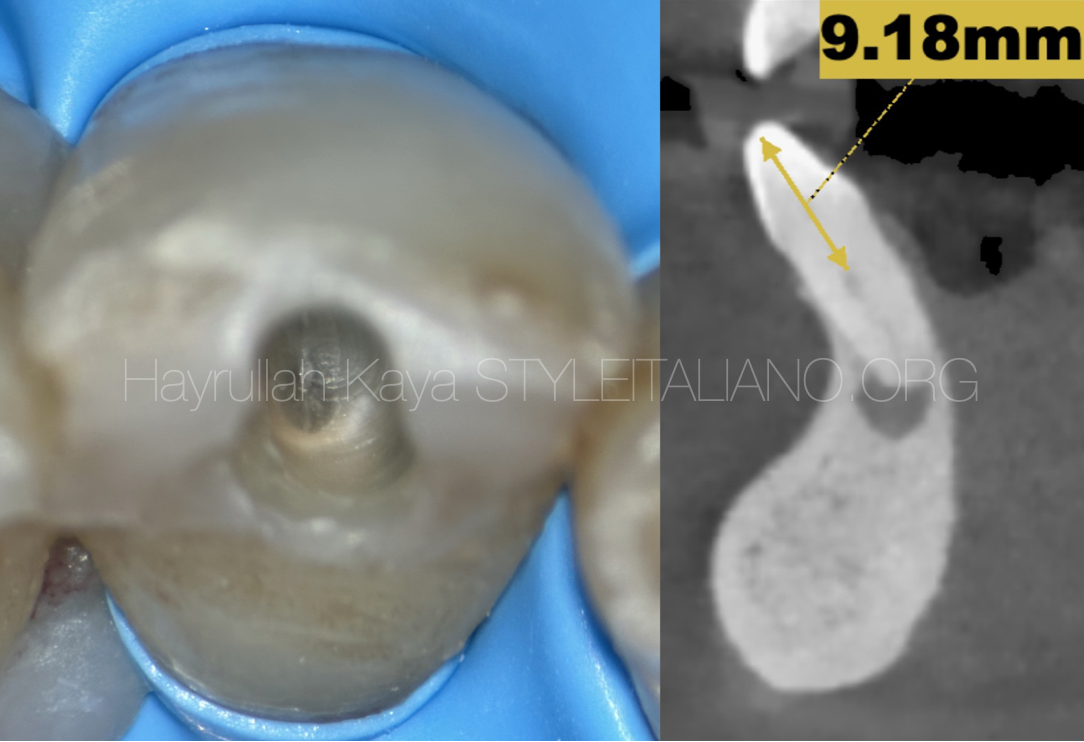
Fig. 1
Preoperative radiographic analysis
This is a referred case as a reason of inability to negotiate the canal of tooth no. 12 to full length.
From the coronal section of CBCT, it was evident the presence of periapical lesion with no canal could be seen apically.
As a rule, the presence of periapical lesion is an indication of patent canal apically.
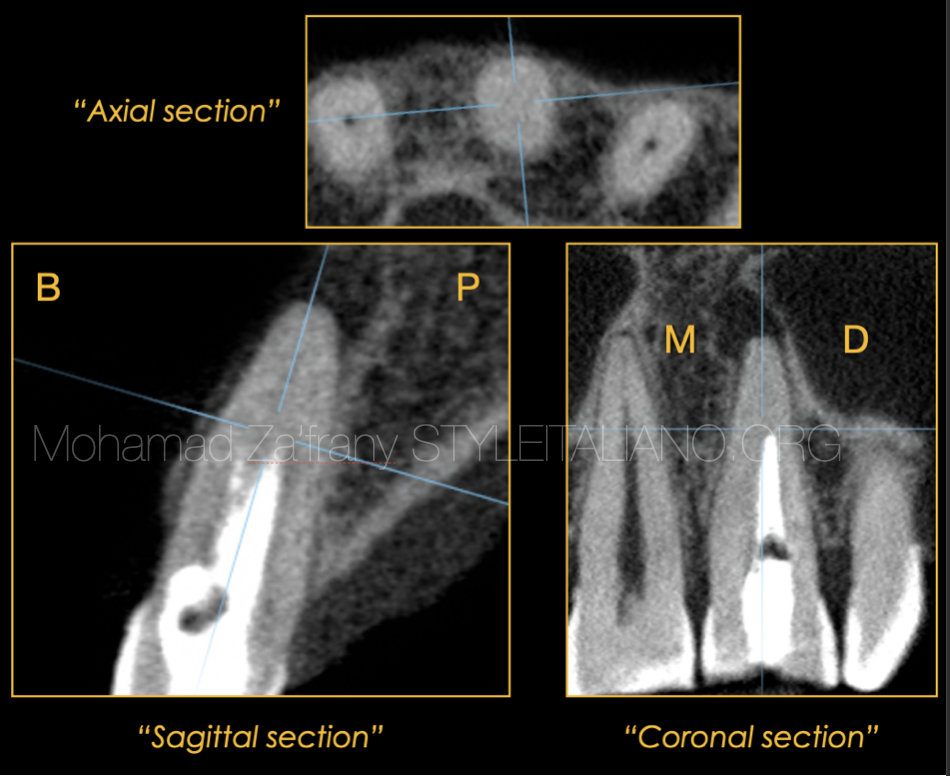
Fig. 2
CBCT analysis
By examination of more CBCT cuts it seems like the prior attempt to locate the canal entrance or the canal path failed as a reason of misalignment of used tools either ultrasonics or files.
So the site of the canal looks to be more mesial and more buccal to the previous reduction site.
In the axial cut is confirmed the obliteration of the canal at the level of blockage.
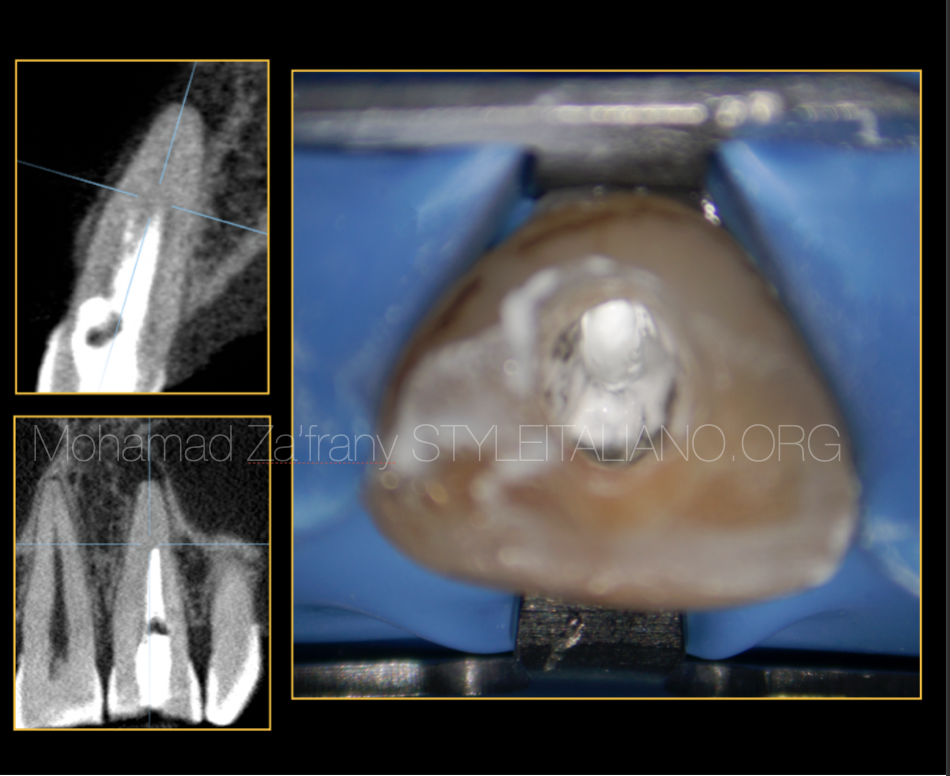
Fig. 3
clinical intervention
After removal of old temporary filling, calcium hydroxide dressing was detected.
It was great to have a radiopaque material inside the canal to trace the previous site of reduction and troughing.
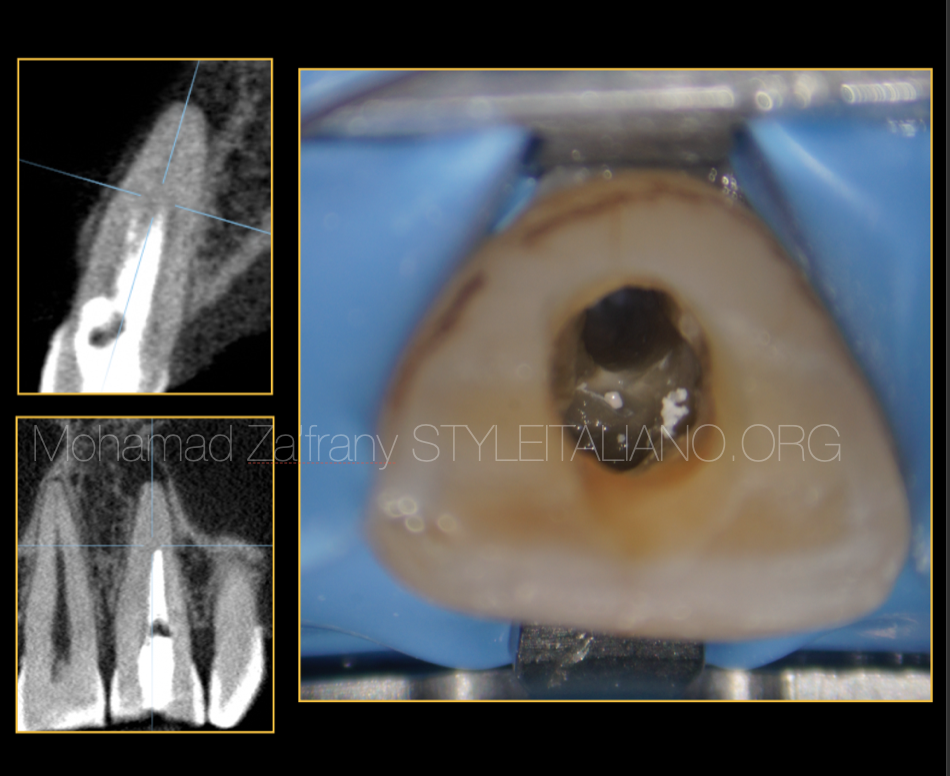
Fig. 4
Removal of canal dressing.
Old calcium hydroxide removed with active irrigation with ultrasonics.
At this stage the use of magnification is very important for precise more conservative reduction
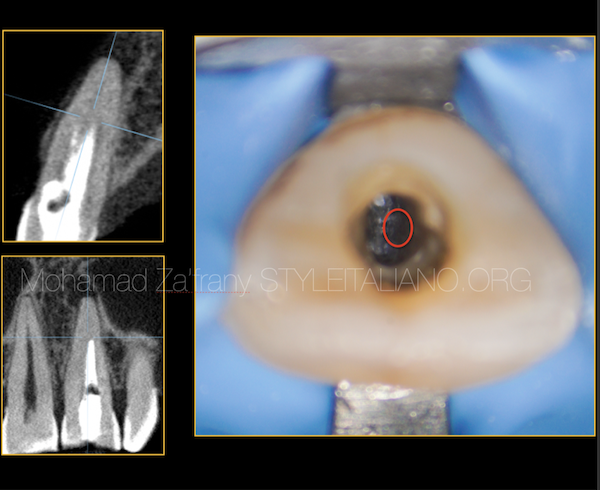
Fig. 5
identifying the site of the canal
The red circle represent the site where the canal should exist which is more buccal and more mesial to the previous reduction site.

Fig. 6
locating the catch
The site of the canal located with the use of magnification and ultrasonics and here comes the role of C file to negotiate the canal.
As the canal is tight and narrow the use of C file is recommended to avoid buckling and bending effect of K files.
C files from Fanta are made of high quality stainless steel which is heat treated to make it more stiff for easier negotiation to the narrow canal
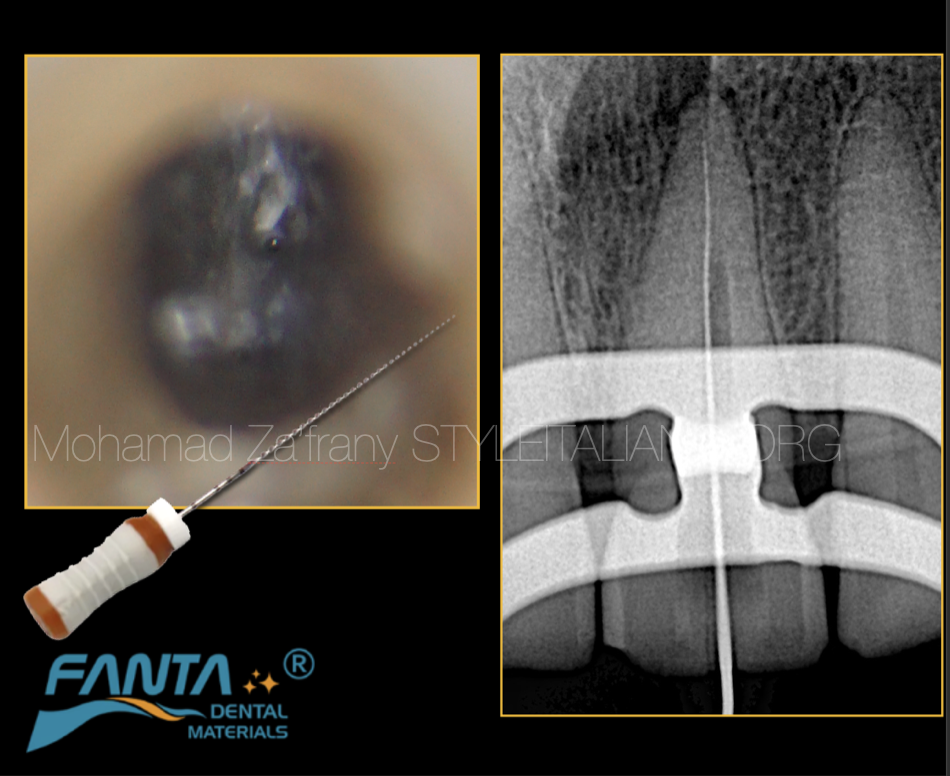
Fig. 7
Negotiation to full lenegh
Canal negotiated to full length using C files with the help of EDTA solution
Files used were 10,12 from Fanta C files.
Working length determined using apex locator but we need to take care and double confirm that this is the canal path not a superimposed perforation thats why shifting the X-ray cone mesial and distal would be preferred as a confirmatory step
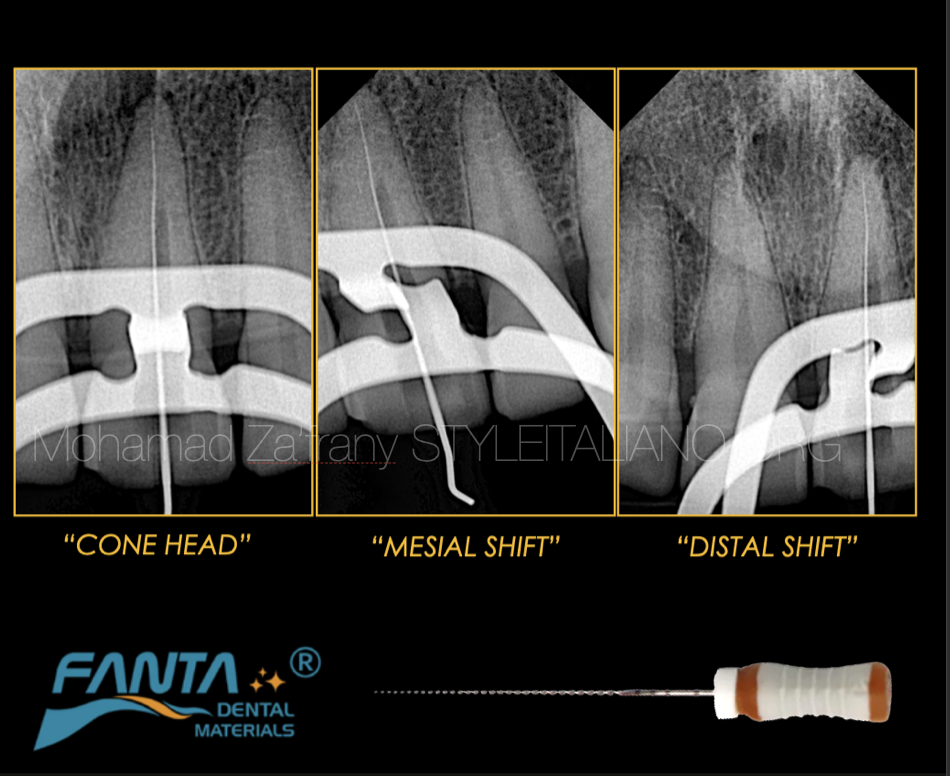
Fig. 8
Double check and confirming the canal path
Mesial and dista shift radiographs were taken confirming its the canal and its not a perforation.
The relation of the file with the root didn’t change, the file is always in the middle of the canal with different cone shift and angulation.
If there is any difference in the relation that would be an indication of superimposed perforation
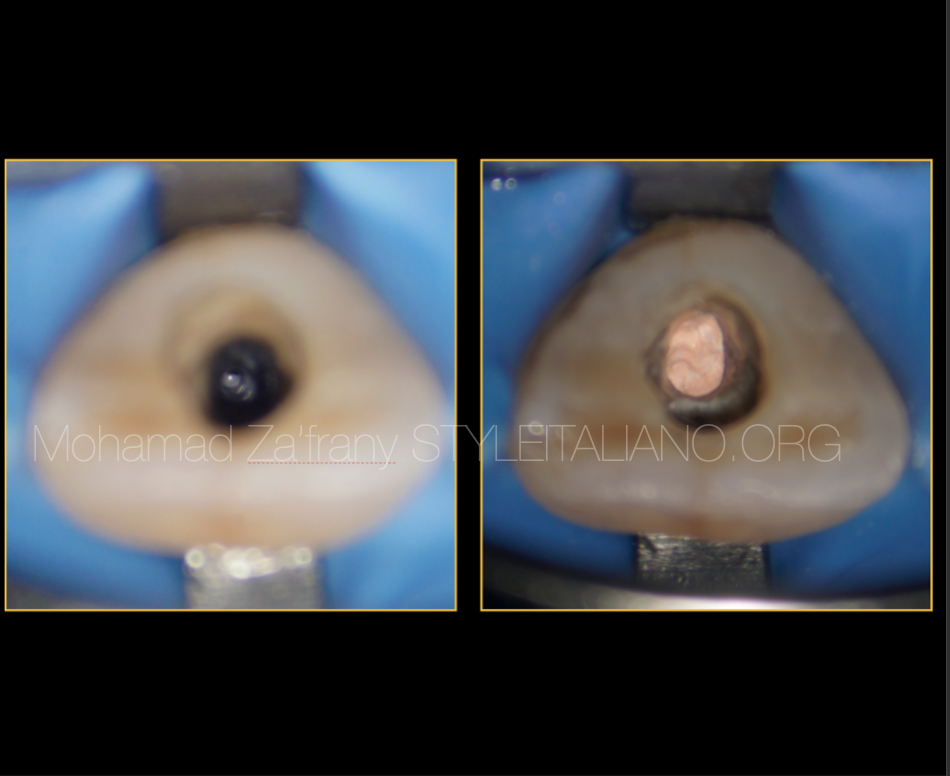
Fig. 9
Canal shaped and obturated
Clinical image showing conservative shaping and obturation to the canal.
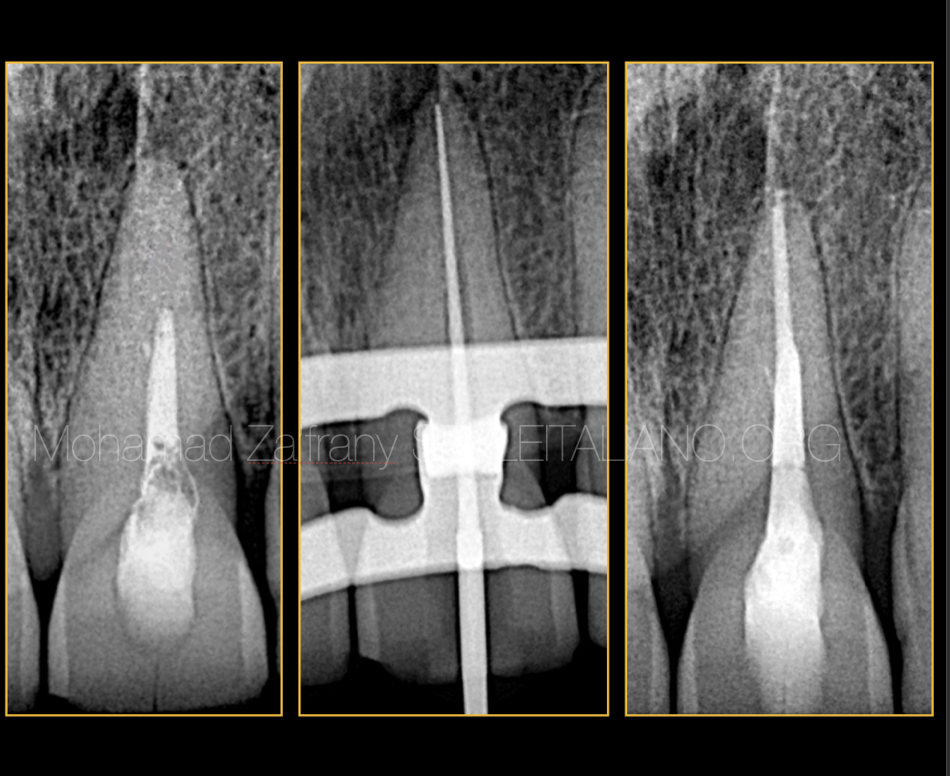
Fig. 10
Radiographic workflow
Final radiographs of MC fit and obturation showing sussessful management of the case with conservative approach.
Conclusions
Preoperative radiograph is very important before starting endodontic treatment
Case difficulty assessment will lead to successful treatment through good planning and selection of the approach technique and the right tools.
The use of magnification and ultrasonic is considered a safe technique to locate calcified canal entrances.
Implementation of CBCT, Magnification and ultrasonics is recommended in complex cases
C files from Fanta Dental materials is recommend for negotiation of narrow and tight canals.
Bibliography
Krasner P, Rankow HJ. Anatomy of the pulp chamber floor. JOE 2004; 30(1):5.
Cohen S, Hargreaves K. Pathways of the Pulp 9th ed. Mosby, St. Louis, MO, 2006.
Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS. Effect of magnification on locating the MB2 canal in maxillary molars. JOE 2002. doi: 10.1097/00004770-200204000-00016.
Nasiri K, Wrbas KT. Management of calcified root canal during root canal therapy J Dent Sci. 2023 Oct; 18(4): 1931–1932.
Falcon P.A., Falcon C.Y., Abbasi F., Hirschberg C.S. Chamberless endodontic access for treatment of calcified anterior central incisors. J Endod. 2021;47:322–326.
Rodríguez G, Patel S, Durán-Sindreu F, Roig M, Abella F. Influence of Cone-beam Computed Tomography on Endodontic Retreatment Strategies among General Dental Practitioners and Endodontists. J Endod. 2017 Sep;43(9):1433-1437. doi: 10.1016/j.joen.2017.04.004. Epub 2017 Jul 8. PMID: 28689702.