When Anatomy Fights Back: retreatment of a C-shaped mandibular second molar
12/01/2026
Shereen AlAttar
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Re-treatment of C-shaped mandibular molars demands 3D cleaning and sealing beyond files; a stepwise strategy improves predictability.
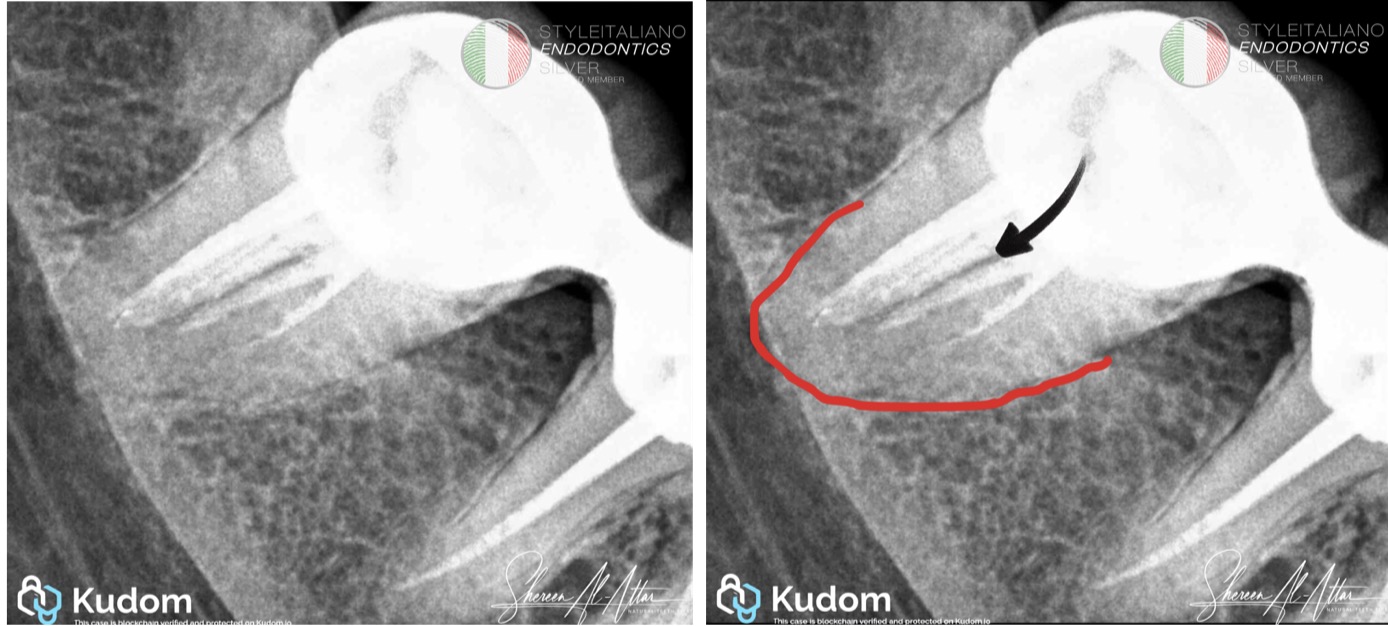
Fig. 1
Diagnostic Clue & Treatment Planning
From the initial periapical radiograph of tooth #47, the presence of a single root outline associated with a furcation-like radiolucent line raised strong suspicion of a C-shaped canal system. Such radiographic features have been consistently reported as key indicators of C-shaped morphology in mandibular second molars [1,3]. This diagnostic insight guided the decision to adopt a retreatment protocol emphasizing enhanced coronal access, ultrasonic assistance, and activated irrigation to compensate for the limitations of mechanical instrumentation.
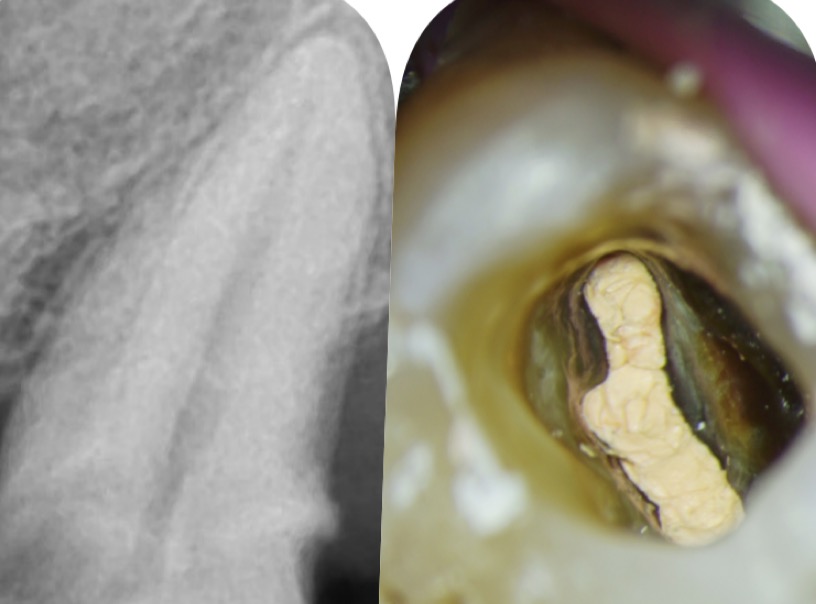
Step 1: Coronal Disassembly
Coronal disassembly was performed through crown removal, elimination of the existing restoration, and retrieval of the coronal gutta-percha. The pulp chamber was then carefully cleaned using ultrasonic tip, ET 20 (Satelec, Acteon group, Merignac, France). This step is essential in retreatment cases, particularly in teeth with complex anatomy, as it restores straight-line access, improves visualization, and removes coronal leakage pathways that may compromise disinfection [4].
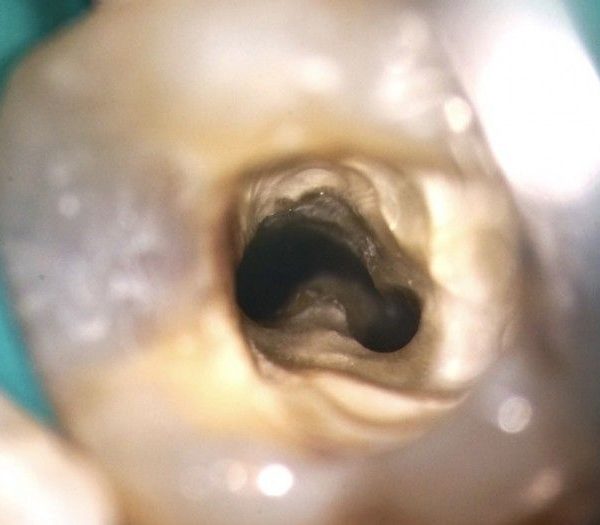
Step 2: Canal Inspection
Following chamber refinement, inspection of the pulp floor confirmed a C-shaped canal configuration, characterized by a continuous groove-like anatomy rather than discrete round orifices. C-shaped systems are known to exhibit significant anatomical variation along the root length, reinforcing the importance of continuous reassessment during treatment rather than reliance on coronal morphology alone [1,2].
Step 3: Cleaning & Shaping
Complete removal of the previous obturation material was achieved using a combination of austenite rotary retreatment files, piezoelectric ultrasonic tip (ET20 Acteon), and the XP Finisher. While rotary instruments effectively removed gutta-percha from the main canal path, adjunctive ultrasonic activation and adaptive finishing files were essential for disrupting filling remnants located in fins and irregular extensions that are typically untouched by conventional instruments [2,5].
Step 4: Irrigation & Activation
Irrigation was delivered using Irriflex plastic needles and enhanced through both sonic and ultrasonic activation. In C-shaped canal systems, where a large proportion of the canal surface remains uninstrumented, irrigation dynamics play a decisive role in debridement and disinfection. Activated irrigation has been shown to significantly improve irrigant penetration, debris removal, and smear layer disruption within complex canal anatomies [4,5]
Step 5: Obturation
Obturation was completed using a tricalcium silicate–based sealer in a sealer-dependent Cold Hydraulic Condensation technique, using total fill sealer (FKG). This approach was selected to address the irregular geometry of the C-shaped canal system. Bioceramic sealers exhibit favorable flow characteristics, slight expansion upon setting, and bioactive properties, allowing improved adaptation to canal irregularities and potentially enhancing long-term sealing and periapical healing [6].
Conclusions
Several classification systems, including those proposed by Melton et al. and Fan et al., have been introduced to describe the characteristic ribbon-shaped anatomy of C-shaped canals, which may present as either a continuous or an interrupted configuration. From a clinical standpoint, however, the primary relevance of these classifications lies in guiding treatment adaptation rather than categorization. Careful assessment of periapical radiographs and, when indicated, CBCT imaging; allows the clinician to appreciate the full extent of the canal system and to manage it comprehensively, irrespective of the specific C-shaped subtype. Consequently, respecting the original anatomy, implementing a meticulous cleaning and activation protocol, and selecting an obturation technique tailored to this complex morphology are fundamental to achieving predictable clinical success.
This case demonstrates that successful management depends primarily on early identification of the anatomical variation, meticulous coronal control, and the combined use of adjunctive techniques aimed at enhancing three-dimensional cleaning and disinfection of the complex fin–isthmus system. Activated irrigation, ultrasonic assistance, and adaptive instruments played a decisive role in the effective removal of previous obturation materials. Furthermore, the use of a tricalcium silicate–based sealer facilitated improved adaptation and sealing of the irregular canal space. When these principles are applied systematically, predictable retreatment outcomes can be achieved even in the presence of highly complex C-shaped canal anatomy. [1,2,6].
Bibliography
1)Fan B, Cheung GSP, Fan M, Gutmann JL, Bian Z.C-shaped canal system in mandibular second molars: Part I—Anatomical features. Journal of Endodontics. 2004;30(12):899–903.
2)Fan B, Min Y, Lu G, Yang J, Cheung GSP, Gutmann JL. Negotiation of C-shaped canal systems in mandibular second molars. Journal of Endodontics. 2009;35(7):1003–1008.
3)Manning SA. Root canal anatomy of mandibular second molars. Part II. C-shaped canals. International Endodontic Journal. 1990;23(1):40–45.
4)Haapasalo M, Shen Y, Wang Z, Gao Y. Irrigation in endodontics. British Dental Journal. 2014;216(6):299–303.
5)van der Sluis LWM, Versluis M, Wu MK, Wesselink PR. Passive ultrasonic irrigation of the root canal: A review of the literature. International Endodontic Journal. 2007;40(6):415–426.
6)Camilleri J. Hydraulic properties of bioceramic root canal sealers. Journal of Endodontics. 2015;41(7):1077–1082.