Partial pulpal necrosis. It occurs occasionally.
29/05/2025
Calogero Bugea
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Managing dental elements with complex endodontic pathologies presents a daily challenge in clinical practice. The case of a lower molar with three canals, characterized by the appearance of a fistula in the furcation area and the subsequent diagnosis of partial pulp necrosis, highlights the need for an accurate diagnostic approach and targeted therapeutic choices. The use of biocompatible materials such as MTA proves crucial in sealing complex anatomical areas, contributing to the long-term success of the treatment, as demonstrated by the resolution of the clinical picture years later.

Fig. 1
In 2018, a 50-year-old woman came to my observation due to the appearance of a fistula in the furcation area of tooth 46. The tooth was restored with a large composite filling.

Fig. 2
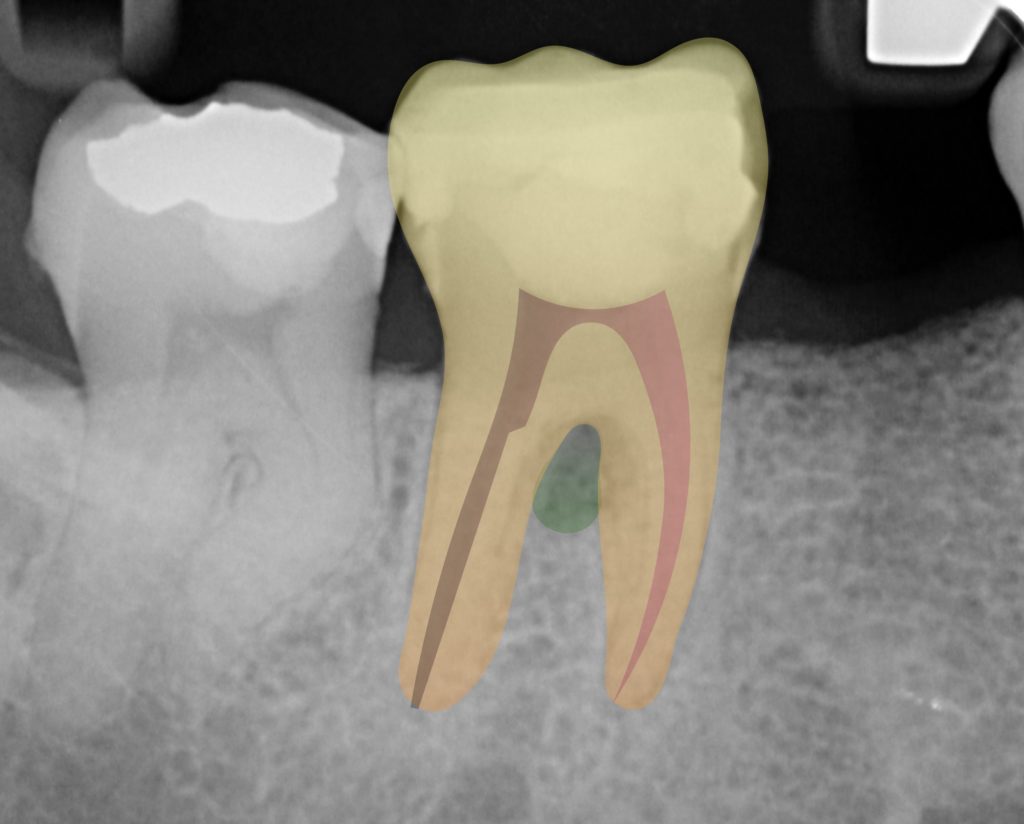
The intraoral radiograph confirmed the presence of infiltrated filling material and showed a radiolucency at the furcation level. However, no radiolucencies were observed at the apex.
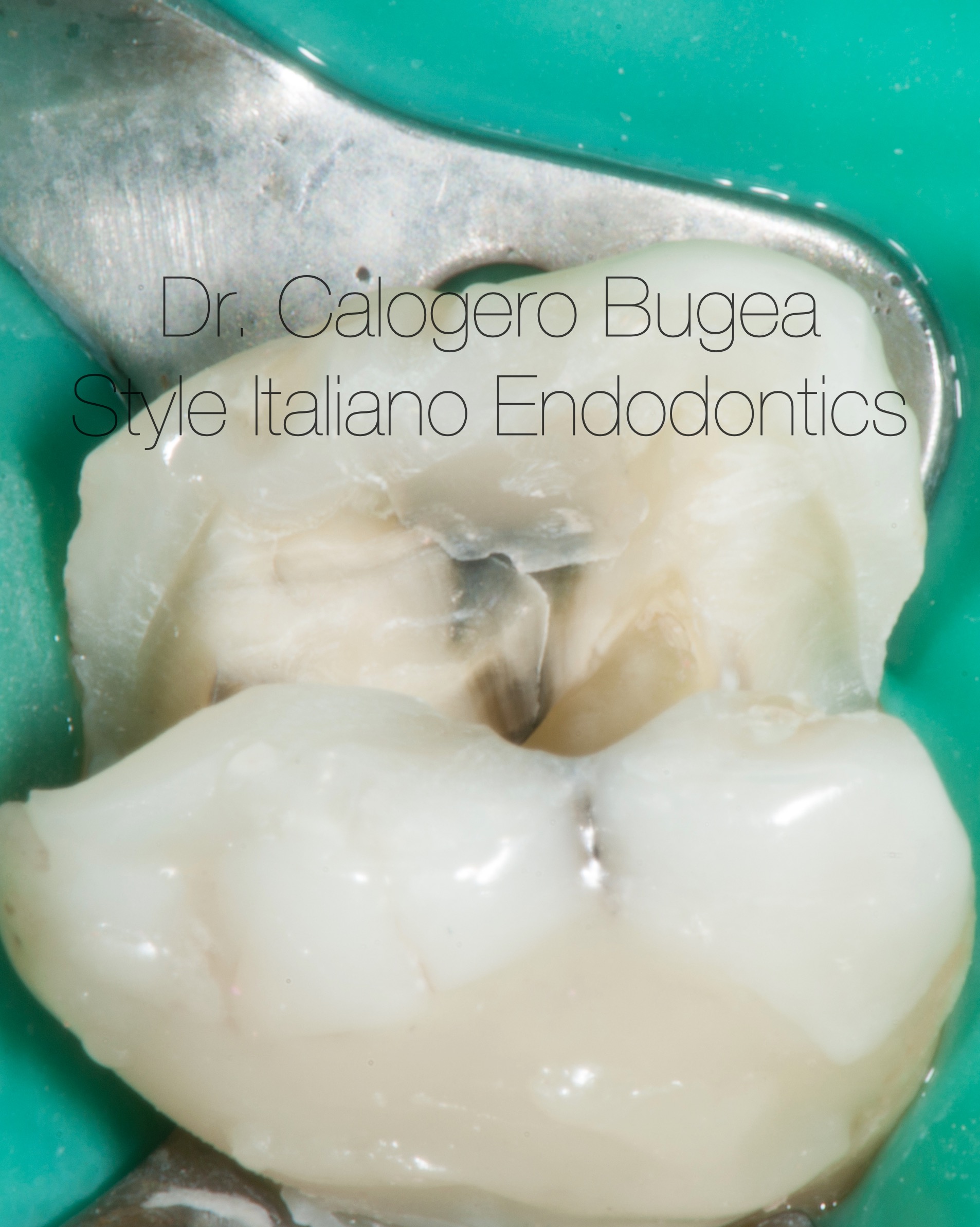
Fig. 3
My immediate thought was that this was a non-vital tooth where, due to the thickness of the cortical bone, the apical lesion wasn't visible, unlike the area near the furcation. Therefore, I opted for a plexus anesthesia instead of the usual nerve block.
I generally prefer to do anestesia in case of retreatments or necrotic teeth to reduce the discomfort due to the clamp of the rubber dam or due to the warm gutta percha inside of the canals.
Fig. 4
During cavity preparation, the patient continued to experience pain, just as if I were treating a vital rather than a necrotic tooth.
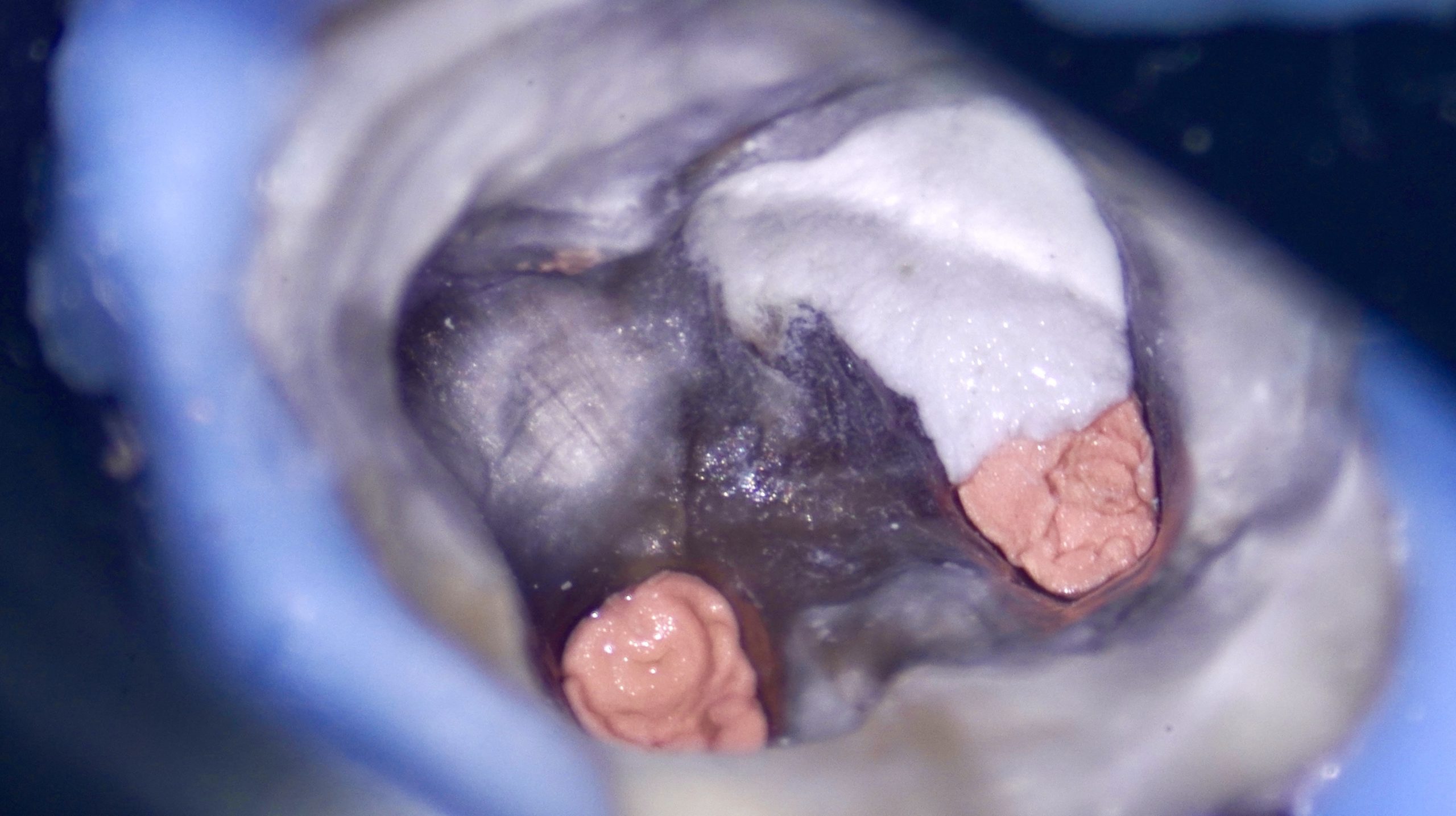
Consequently, I was compelled to perform a nerve block to better manage the pain and work comfortably. Upon opening the pulp chamber, I noticed that the distal canal was bloodless, whereas there was bleeding from the mesial canals. This led me to believe that the tooth was only partially necrotic
Fig. 5
Distal view, the absence of bleeding in the distal canal can be noted
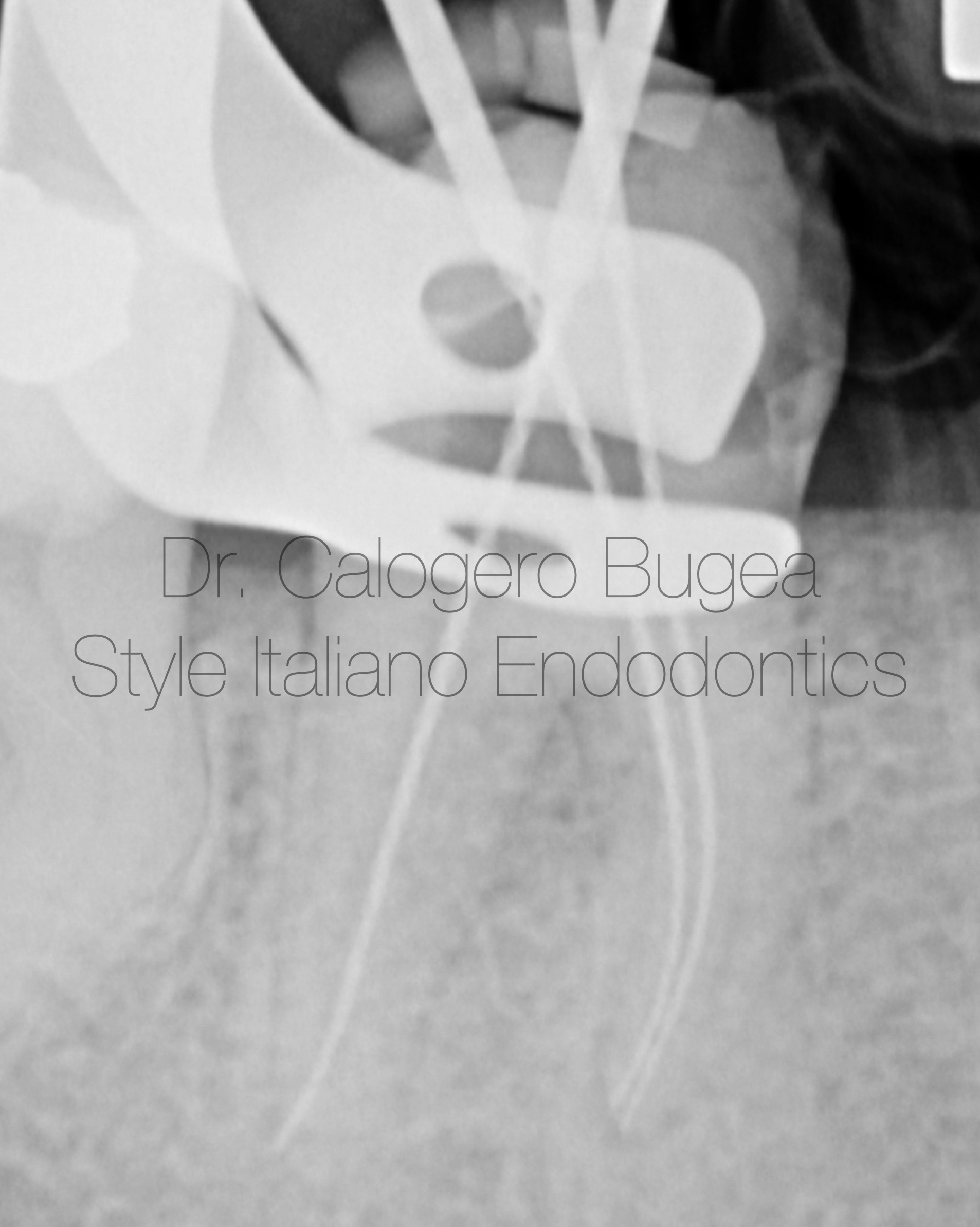
Fig. 6
Working length Xray.
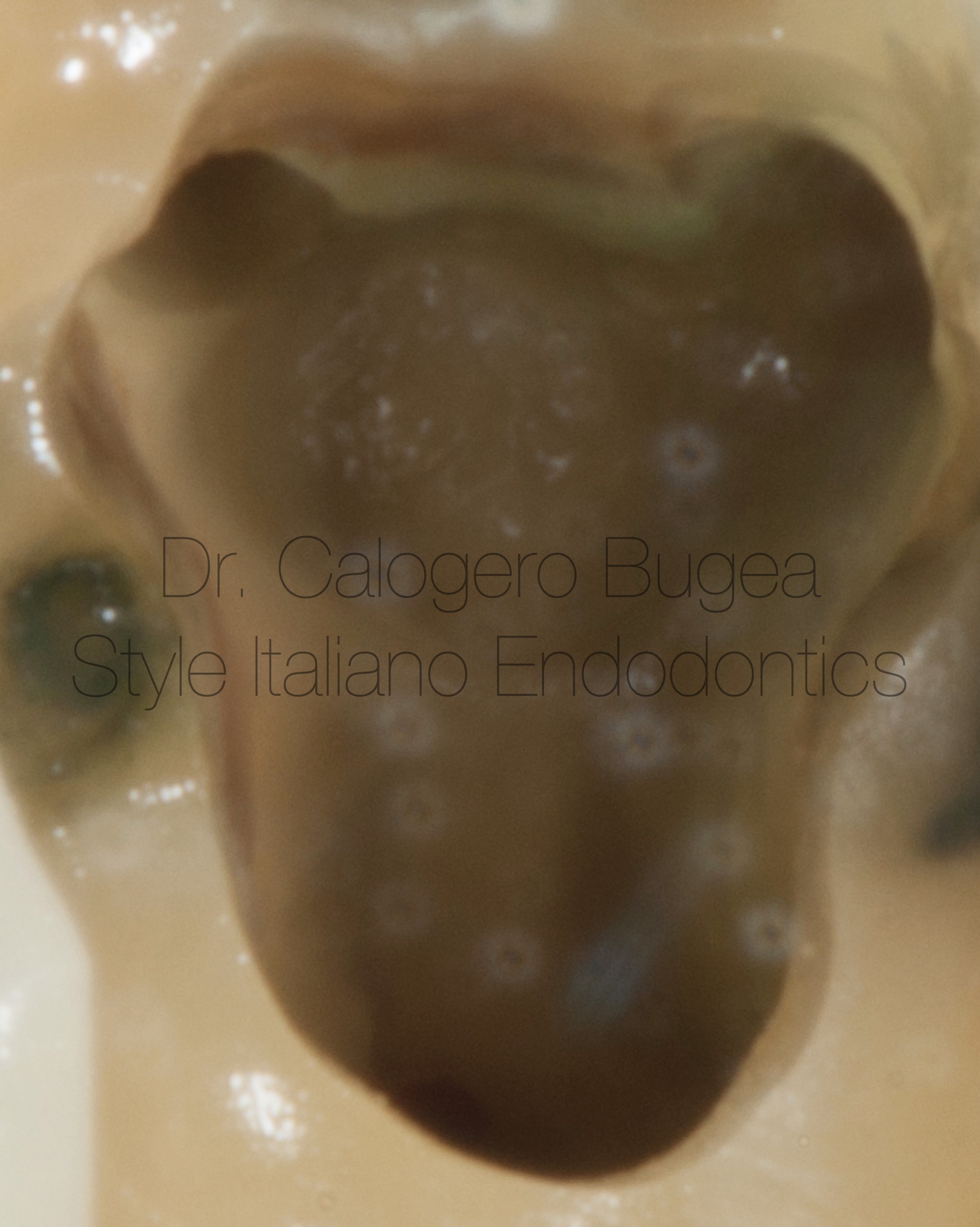
Fig. 7
Pulp chamber after the shaping

Fig. 8
Cone fit in the distal canal.
In the medial canal I used guttacore
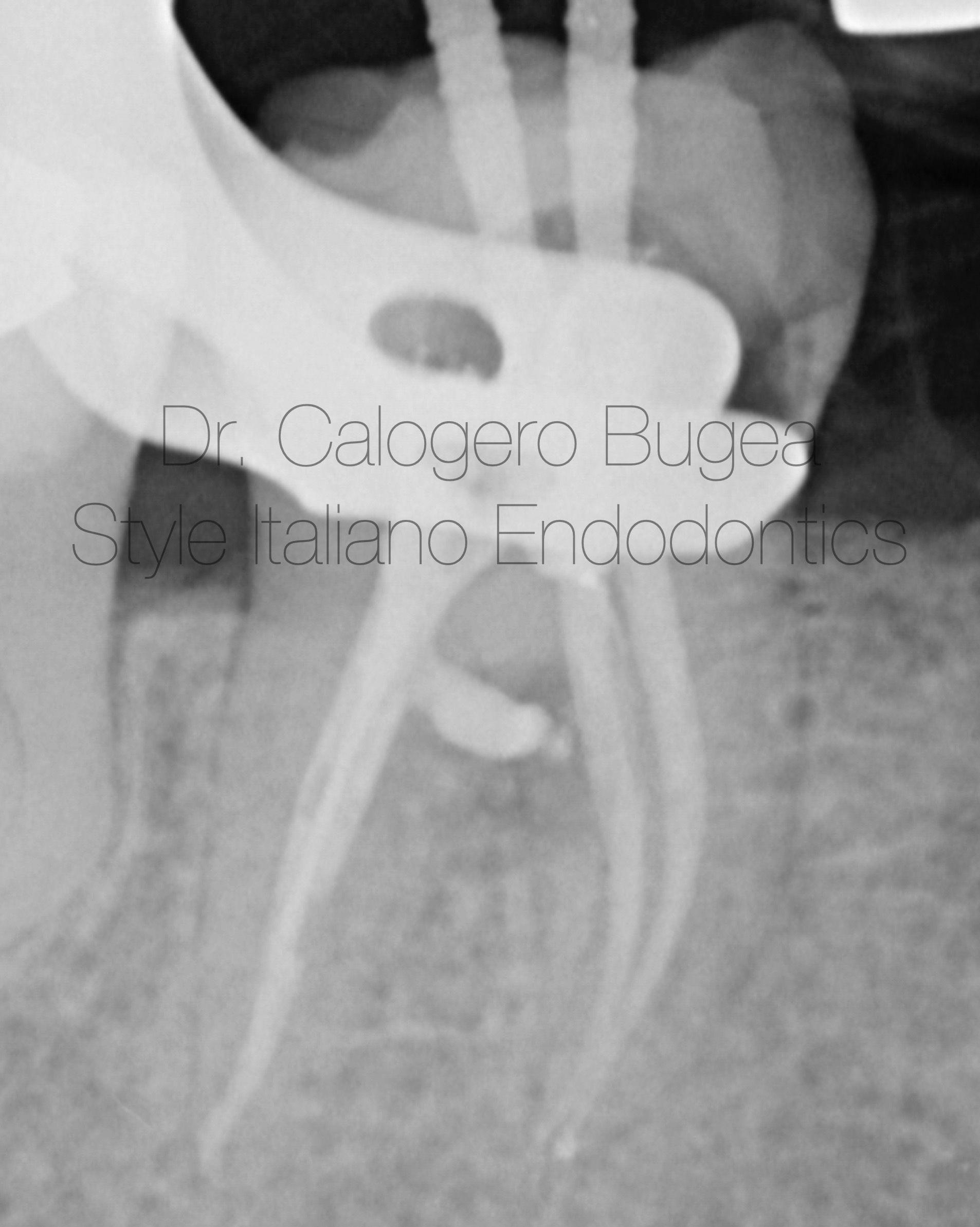
Fig. 9
The post-obturation radiograph revealed a significant extrusion of gutta-percha precisely at the furcation level, from the distal canal. My initial thought was that given the extent of the lesion, gutta-percha might not provide an adequate seal, and that MTA would have been the correct material to ensure a better prognosis.

Fig. 10
Therefore, I chose to remove the filling material from the root canal system. Fortunately, during the removal process, the excess material extruded through the fistula on the buccal side.

Fig. 11
Careful observation of the coronal third allowed me to identify the area that needed to be sealed with MTA. Thanks to the use of the MAP System, I was able to place the MTA with confidence
Fig. 12
Image of the area properly filled with MTA

Fig. 13
A week later, the fistula had disappeared, and the white MTA had completely hardened and slightly changed color, as typically occurs

Fig. 14
Final xray

Fig. 15
I had advised the patient to protect that tooth due to the presence of several cracks and the absence of both marginal ridges, but for financial reasons, she preferred to postpone the prosthetic treatment.
Seven years later, the lingual portion fractured, but fortunately it was manageable prosthetically without the need for periodontal surgery. The fistula completely disappeared, and the radiolucent area at the furcation also resolved.
Conclusions
Careful analysis of the initial radiograph is extremely important for optimal case management. In the presence of perforations or large lateral canals, MTA is able to achieve a better seal compared to thermoplasticized gutta-percha.
Bibliography
1.Gorni FG, Andreano A, Ambrogi F, et al. Patient and clinical characteristics associated with primary healing of iatrogenic perforation after root canal treatment: results of a long-term Italian study. J Endod. 2016;42 (2):211-215.
2. American Association of Endodontists. Treatment Options for the Compromised Tooth: A Decision Guide .
3. Roda RS, Gettleman BH. In: Hargreaves KM, Cohen S, Berman LH, eds. Cohen’s Pathways of the Pulp. 10th ed. St. Louis, MO: Mosby Elsevier:941-942