Management of cervical Perforation, Apical abscess and huge periapical lesion
01/02/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The success of nonsurgical root perforation procedures is directly related to the severity of the initial damage caused to the periodontal tissue, the size and location of the perforation, sealing ability and biocompatibility of the filling material, and the presence or absence of bacterial contamination. Cervical perforation should be sealed immediately after it had occurred. Cases of the inflammatory resorbed apex with huge periapical lesion should be managed with biocompatible hydrophylic material, i.e. calcium silicate cements (MTA, Bioceramics).

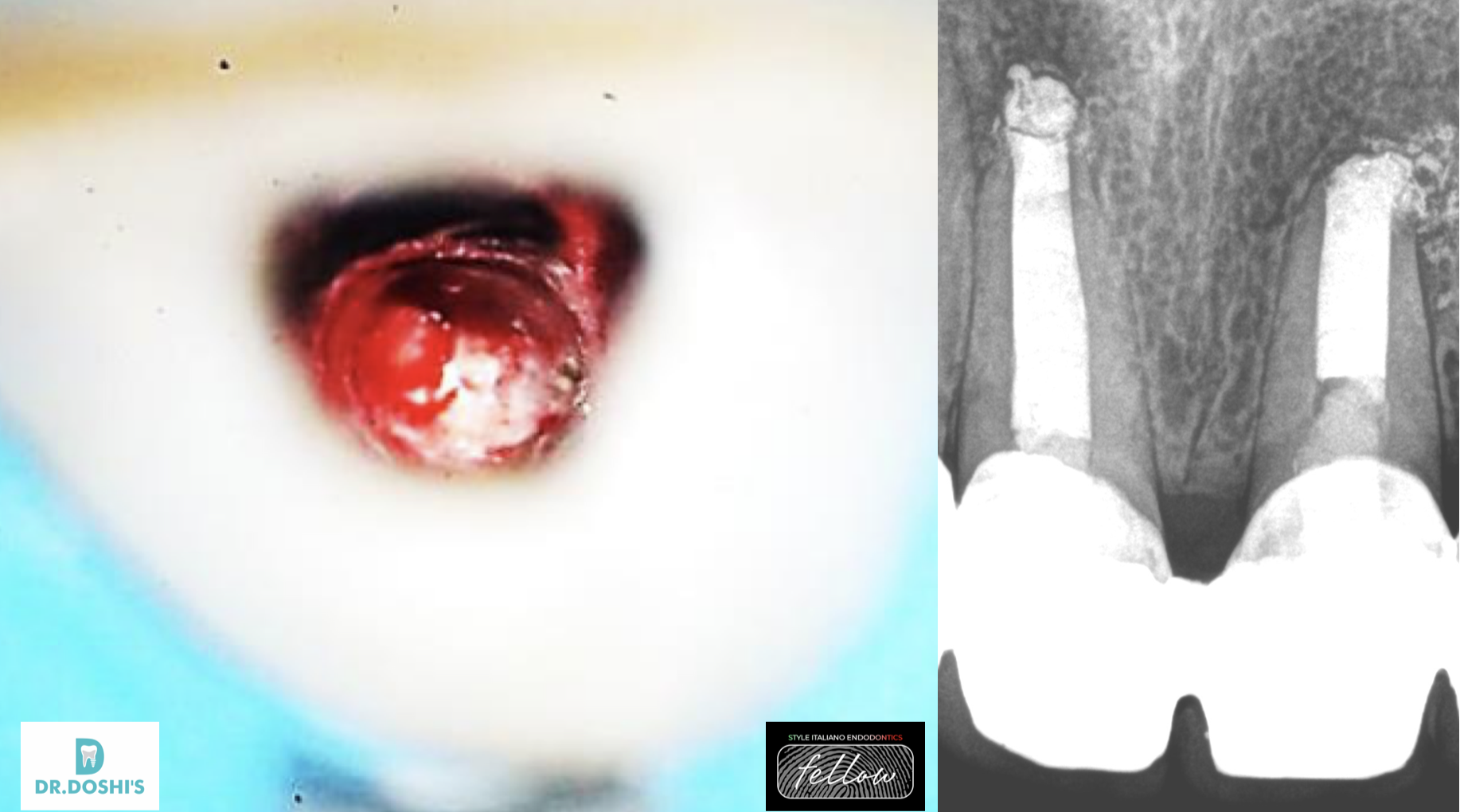
Fig. 1
Initial Appearance
Patient K., 34 yo,
1.1 / 1.2 Acute Apical Abscess «Hot Tooth»
Extremely tender to percussion
Abscess on labial and palatal gingival aspects
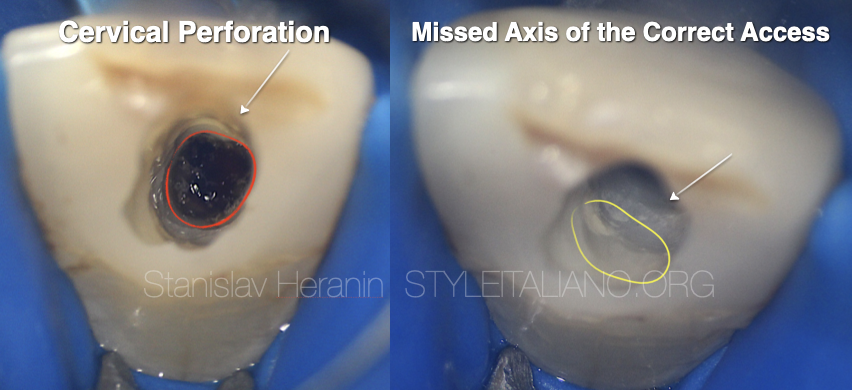
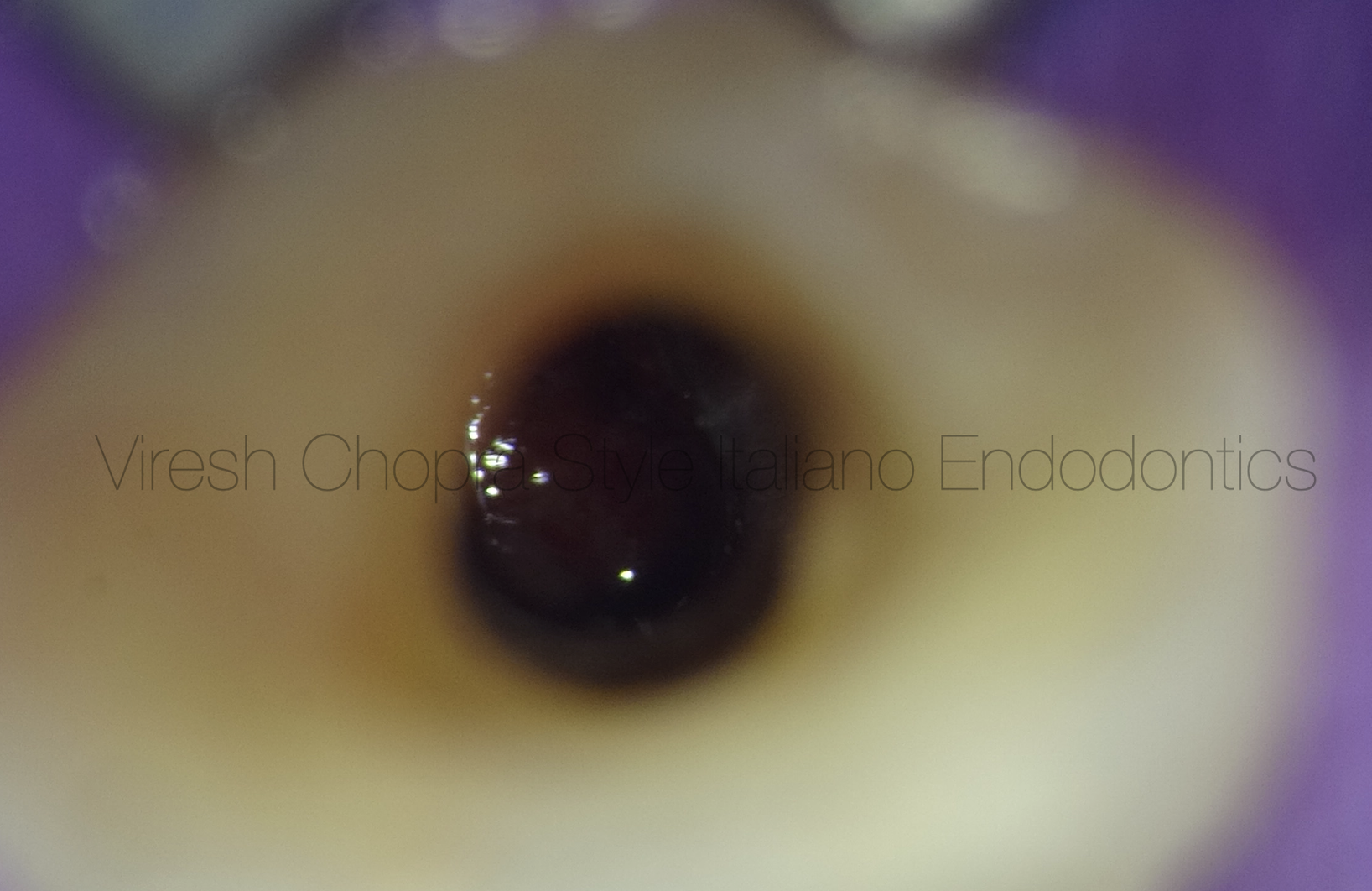
Fig. 2
1.1 Endodontic Access
Revealing of the huge cervical perforation due to missing of the correct Endodontic access
1.1 Endodontic Access
Cervical perforation
Mssing of the correct Endodontic access
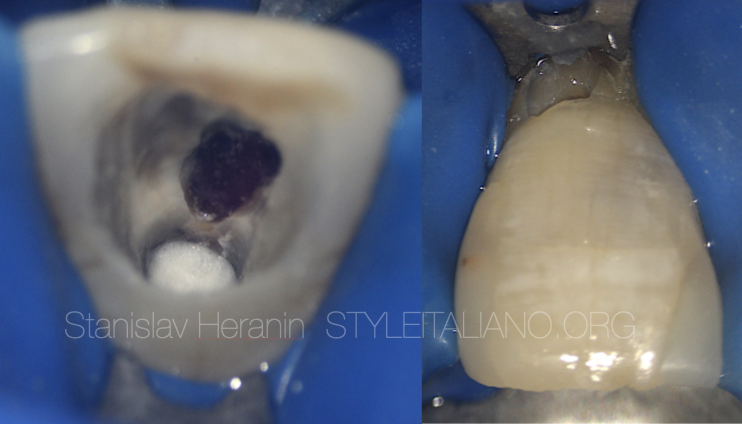
Fig. 3
1st Appointment
1.1 Endodontic Access
Cervical perforation & Granulation tissue
Gaining true access

Fig. 4
1st Appointment
1.1 Treatment options
Gaining true access, Desobturation, Copious 5.25% NaOCl irrigation with PUI, Calcium Hydroxide dressing
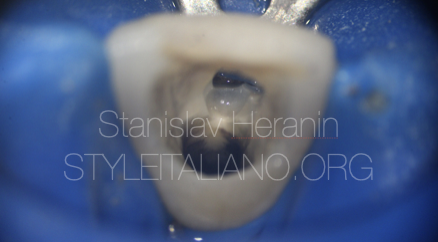
Fig. 5
1st appointment
1.1 Final appearance
1st appointment
1.1 Final appearance

Fig. 6
2nd Appointment
Asymptomatic
1.1 / 1.2 Treatment options
Copious 5.25% NaOCl irrigation with PUI, MTA plugs
Cervical perforation restored with the composite
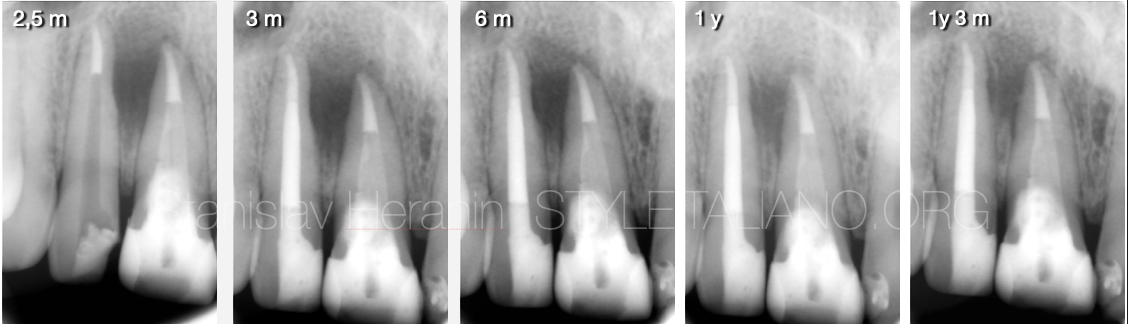
Fig. 7
Follow-ups

Fig. 8
2,5 y Follow-up
1.1 / 1.2 Asymptomatic
Scar remains on the labial aspect
Healthy marginal gingiva
Complete healing of the periapical lesion

Fig. 9
About the author:
Dr Stanislav Heranin
1999: Graduated in Dentistry from the Ukrainian Medical Stomatological Academy - Faculty of Dentistry
1999-2001 - Postgraduate Education (UMSA)
2001-2012 - Professor Assistant - Department of Therapeutic Dentistry (UMSA)
2012-2019 - Professor Assistant - Department of Postgraduate Education of Dental Practitioners (UMSA)
2011: PhD in Dentistry (Ukrainian Medical Stomatological Academy)
2023 until now Associate Professor at The Department of Dentistry – School of Medicine - V.N.Karazin
Kharkiv National University
Private Dental Practice - Dental Centre “Machaon” (Poltava, Ukraine)
Founder of the Educational Centre EndoDiscovery
Past-President of the Ukrainian Academy of Esthetic Dentistry
Board Member of the Ukrainian Endodontic Association
Member of the Ukrainian Endodontic Society
Member of International Jury of Dental Restorative Contest ”Prisma-Championship”
Board member of the International Journal “Ukrainian Dental Journal”
Conclusions
Success or failure depend on the ability to access the perforation area and promote an appropriate sealing.
Visual control of every single manipulation under the operational microscope gives the is the crucial factor in daily practice. Cervical perforations often can be fixed with regular composite restoration, resulting in acceptable result and gum recession. Placement of the traditional MTA plug in open apices give the opportunity to achieve good results. The advantages of using MTA as a root canal obturation material include superior sealing ability, improved fracture resistance, repair and regeneration of supporting tissues, and resolution of resorptive defects.
Bibliography
- Martin RL, Monticelli F, Brackett WW, Loushine RJ, Rockman RA, Ferrari M, Pashley DH, Tay FR. Sealing properties of mineral trioxide aggregate orthograde apical plugs and root fillings in an in vitro apexification model. J Endod. 2007 Mar;33(3):272-5. doi: 10.1016/j.joen.2006.11.002. Epub 2007 Jan 4. PMID: 17320712.
- Mathew AI, Lee SC, Rossi-Fedele G, Bogen G, Nagendrababu V, Ha WN. Comparative Evaluation of Mineral Trioxide Aggregate Obturation Using Four Different Techniques-A Laboratory Study. Materials (Basel). 2021 Jun 7;14(11):3126. doi: 10.3390/ma14113126. PMID: 34200233; PMCID: PMC8201240.
- Castellucci A. The use of mineral trioxide aggregate in clinical and surgical endodontics. Dent Today. 2003 Mar;22(3):74-81. PMID: 12705015
- Giovarruscio M, Uccioli U, Malentacca A, Koller G, Foschi F, Mannocci F. A technique for placement of apical MTA plugs using modified Thermafil carriers for the filling of canals with wide apices. Int Endod J. 2013 Jan;46(1):88-97. doi: 10.1111/j.1365-2591.2012.02115.x. Epub 2012 Nov 9. PMID: 23137342
- Torabinejad M, Parirokh M, Dummer PMH. Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview - part II: other clinical applications and complications. Int Endod J. 2018 Mar;51(3):284-317. doi: 10.1111/iej.12843. Epub 2017 Oct 11. PMID: 28846134