Management of Immature Permanent Incisors with wide open apex
26/07/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
A major problem associated with treating traumatized teeth with necrotic pulps and open apices, is achieving an acceptable seal in the apical area. Apexification has traditionally formed an integral part of the treatment of teeth with necrotic pulps with open apices. Apexification is defined as “a method to induce a calcific barrier across an open apex of an immature, pulplesstooth”.
Historically, calcium hydroxide was the material of choice used to induce the formation of an apical hard tissue barrier. However, there are several disadvantages of apexification with calcium hydroxide. The treatment requires multiple appointments over an extended period of time which can last from 3-24 months, repeated number of dressings necessary to complete closure, outcome may be unpredictable resulting in incomplete calcification of bridge, increased risk of fracture after the long-term application of calcium hydroxide, esthetic concerns, and coronal microleakage.
Mineral trioxide aggregate (MTA) has been popularized in endodontics due to a large amount of research indicating the beneficial properties of the material in terms of bio-compatibility, ease of manipulation and placement, and a wide array of applications. It has been used for procedures ranging from direct pulp capping to perforation repair as well as for inducing an artificial barrier in open-apex cases.
MTA is composed of dicalcium and tricalcium silicate, bismuth oxide, and calcium sulfate. Hydration of the powder results in a fine crystalline gel. This solidifies to a hard structure in approximately 6-8 hours.
MTA has several advantages, it can be placed in single visit, is biocompatible, non-mutagenic and non-neurotoxic, can induce hard tissue formation, and has good sealing properties. Mineral trioxide aggregates (MTA) has become the material of choice for artificial apical plug. This article presents a detailed case report of using a novel technique of MTA as an apical barrier in treatment of immature permanent incisors with open apex.

Fig. 1
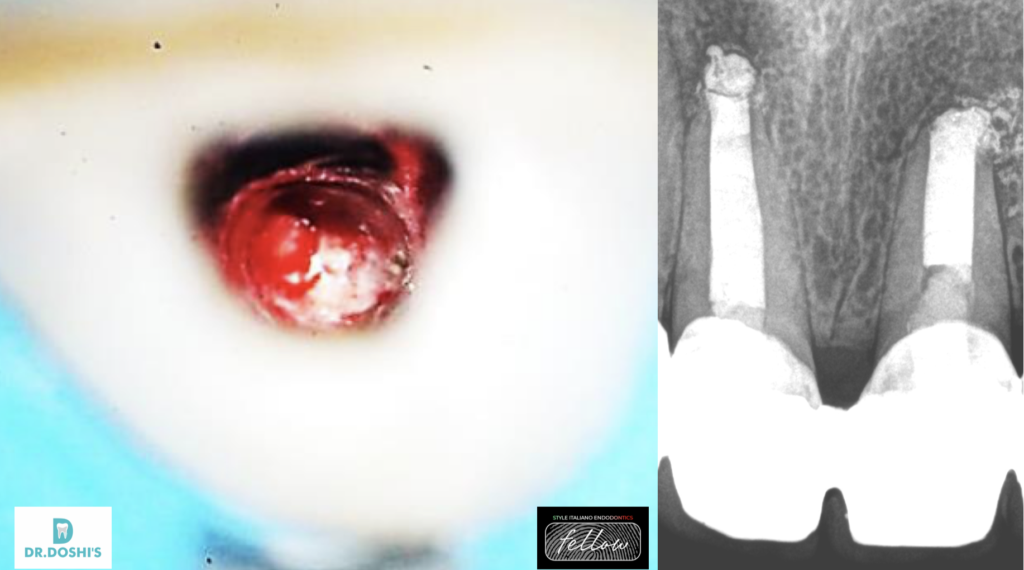
A 22year old male patient presented to practice with a chief complaint of discoloredmaxillary central incisors. Dental history revealed that the patient had histiory of trauma few years back . Clinical examination revealed discolored tooth no.11 and 21. Radiographic examination revealed both central incisors with open apex associated with periapical lesion.
Treatment planning was done and patient was advised to do root
canal therapy followed by Apexification procedure with MTA
followed by prosthetic rehabilitation for discolored central incisors.

Fig. 2
After application of rubber dam , access cavity preparation was done. At this step, ISO 140no.K-file till the working length in the canal revealed wide open apex , the file was loose within the canal and could easily pass beyond the apical limit of the canal.
The canal was then irrigated with 5.25% sodium hyopochlorite using a 30 gauge side vented needle to avoid its apical extrusion and walls of the canal were cleaned using a circumferential filing motion and calcium hydroxide medication was placed inside the canal.

Fig. 3
MTA carrier or Messing Gun or Dovgan carrirer used under operating microscope to place the MTA in open apex.

Fig. 4
Three weeks later the canals thoroughly irrigated with saline to wash out any remnants of the Ca(OH)2 dressing and 17% liquid EDTA for removal of the smear layer and the canal was then dried with paper points
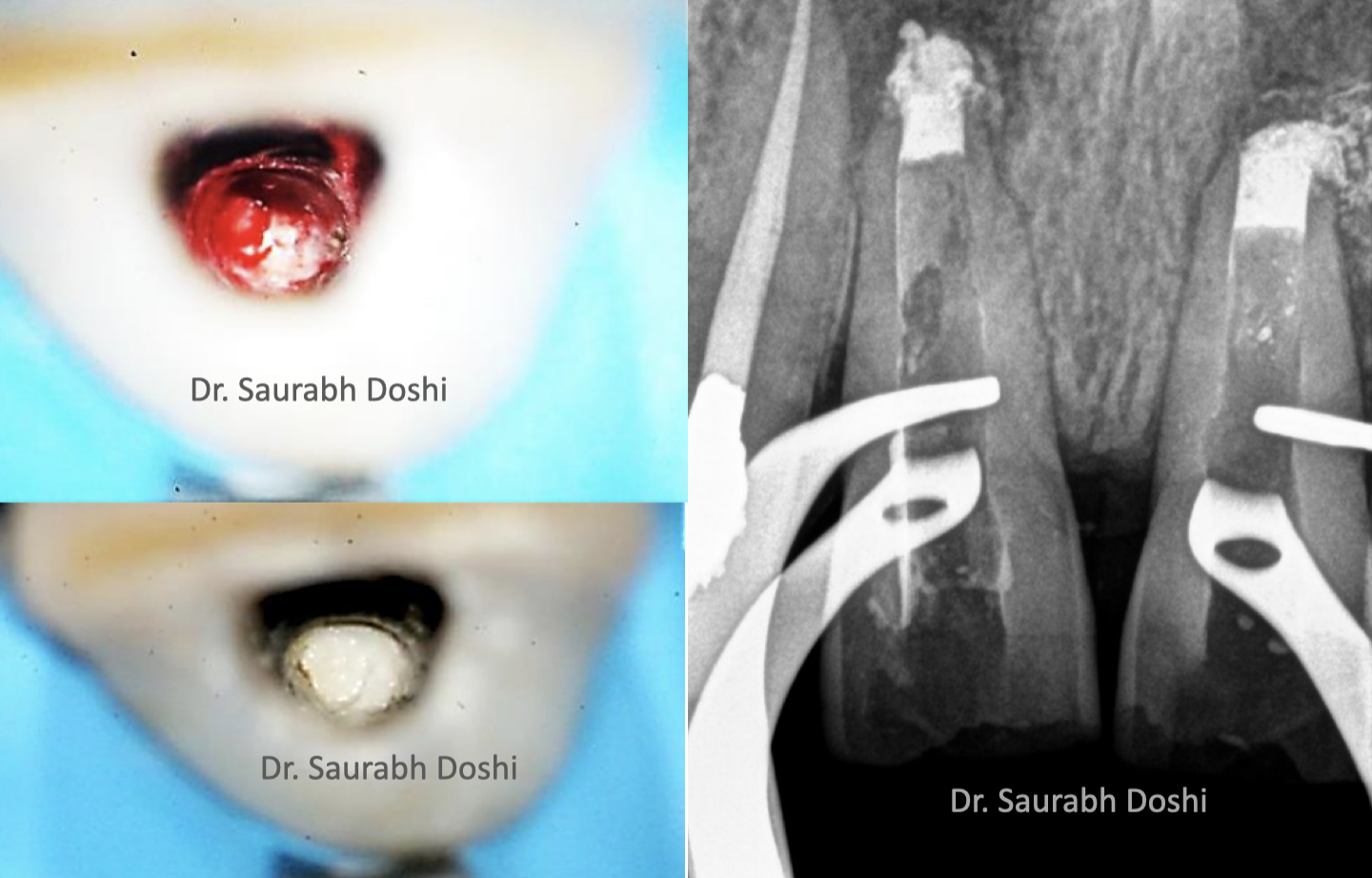
Fig. 5
Once the bleeding stopped, spot check of root canal was done under microscope. The wide open apex was clearly visible under magnification.
Once the canal was shaped and disinfected with irritants it was decided to obturate the complete canal with Calcium Silicate cement (MTA). The reason for choosing MTA as an obturatingmaterial is that there is resorption evident along the length of the root canal wall. Therefore, it would be justified to place a material that can initiate bone formation along the whole surface.
White MTA was then mixed with distilled water according to manufacturer’s instructions and 3-5 mm of MTA plug was subsequently placed at the apex .
Butt end of a paper point was used to compact the material and clear out any excess from the walls. Moistened gauze was placed in the remainder of the canal and the access cavity sealed using glass ionomer cement.
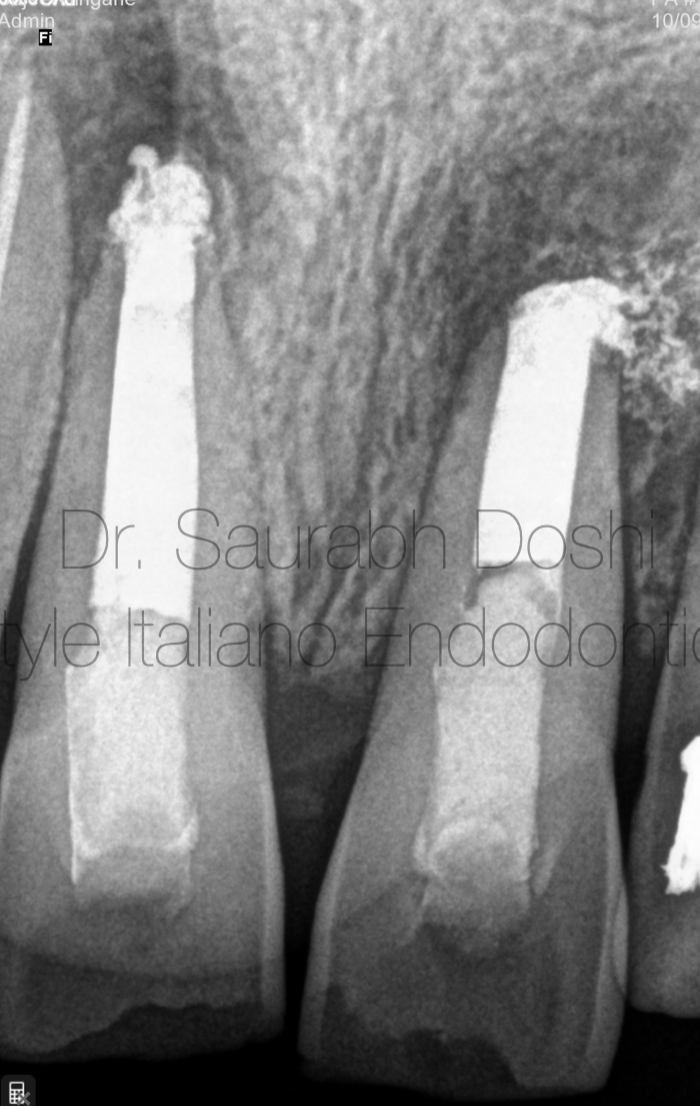
Fig. 6
Since the MTA takes around 6-8 hours for complete setting, the patient was called on the next day and the moist gauze was removed and a plugger was used to check the consistency of the MTA and to examine if the material was thoroughly set. Full length of the root canal was obturated with MTA and verified on the periapical radiograph . The patient was advised full coverage prosthesis.

Fig. 7
A 12 months follow-up revealed the reduction of the lesion.

Fig. 8
Dr. Saurabh Doshi
2015:Diploma in Laser Dentistry (Austria)
2017: Master with honour in Endodontics from M.A Rangoowala Dental College and research centre. Pune. India .
2021: Diplomate of Indian Board od Endodontics from prestigious Indian Endodontic Society, acclaimed and internationally.
Author of the book "the Root Canal Obturation - Past,Present and Future".
Saurabh Doshi has been a speaker in various Indian Dental Associations Forums .
A passionate clinician, avid sportsman and a doting father.
Conclusions
MTA showed favourable material for obturation as it results in good periapical seal at open apices by delivering the MTA right at the apex where it comes in contact with the periapical tissues. This method of MTA compaction using devices that allow the delivery of MTA into the apical area directly shows superior apical seal and will surely serve as a better technique for the operator to produce a successful treatment outcome.
Bibliography
Torabinejad M, WatsonTF, Pitt Ford TR. Sealing ability of a mineral trioxide aggregate when used as a root end filling material. J Endod 1993;19:591.
Torabinejad M, Chivian N. Clinical application of mineral trioxide aggregate; J Endod 1999;25:197-205.
Koh ET, McDonald F, Pitt Ford TR, Torabinejad M. Cellular response to Mineral Trioxide aggregate. J Endod 1998;24:543 ^ 7.
Torabinejad M, Smith PW, KatteringJD, Pitt FordTR. Comparative investigation of marginal adaptation of MineralTrioxide Aggregate and other commonly used root-end filling materials. J Endod 1995;21:295^9