

Do lateral canals matter?
06/02/2025
Ivan Mirovic
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The importance of treating lateral canals has been a long lasting debate between endodontists. From Schilder and Wein debates in the 80s to nowadays debates between Castellucci and Ricucci, the same question arises. Do laterals matter for the outcome of endodontic treatment?

Fig. 1
The first thing we have to understand is that nature does not create lateral canals. It simply creates root canal systems with portals of exit. This becomes obvious if we take a look at Walter Hess work. This is what we encounter in everyday practice!
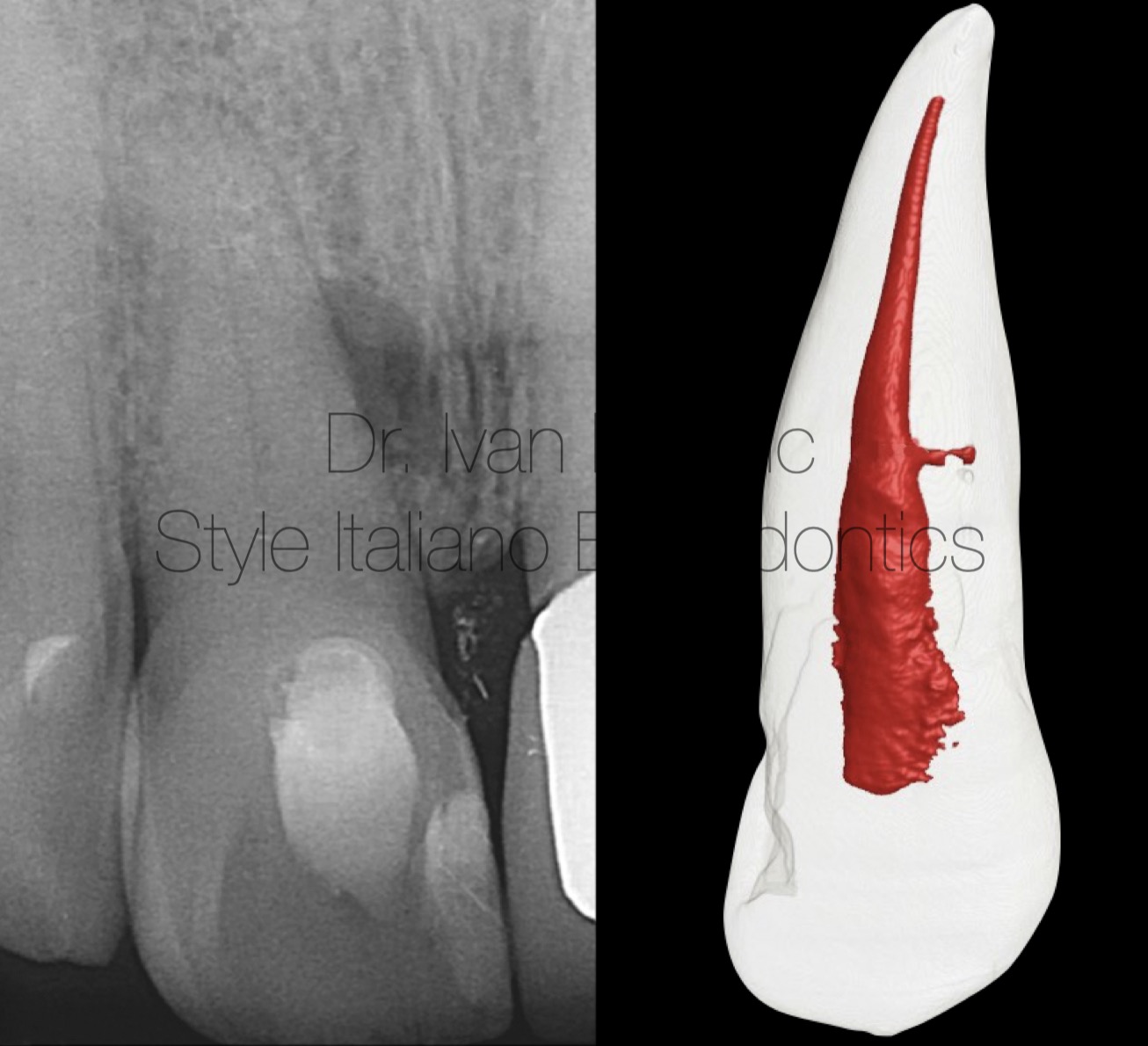
Fig. 2
From clinical point of view it is important to understand two facts:
- Lesions of endodontic origin form in the bone next to the portal of exit, regardless of location along the root surface
- Every portal of exit is potentially significant because it can be the cause of treatment failure
So let's take a look at clinical cases that support those facts.

Fig. 3
This patient was presented with a buccal swelling in the region of lower left second premolar. On preoperative radiograph it was obvious that primary treatment was failing. It was interesting that lesion was located on the lateral side of the root.

Fig. 4
Non surgical retreatment was performed and two canals, which were joining in the common apical foramen, were filled to their full apical and lateral extent. Notice the previously untreated lateral canal which was related to lateral lesion.

Fig. 5
Six month follow up radiograph showing the lesion completely healed. So, does it matter that we filled lateral canal? For this patient it did!
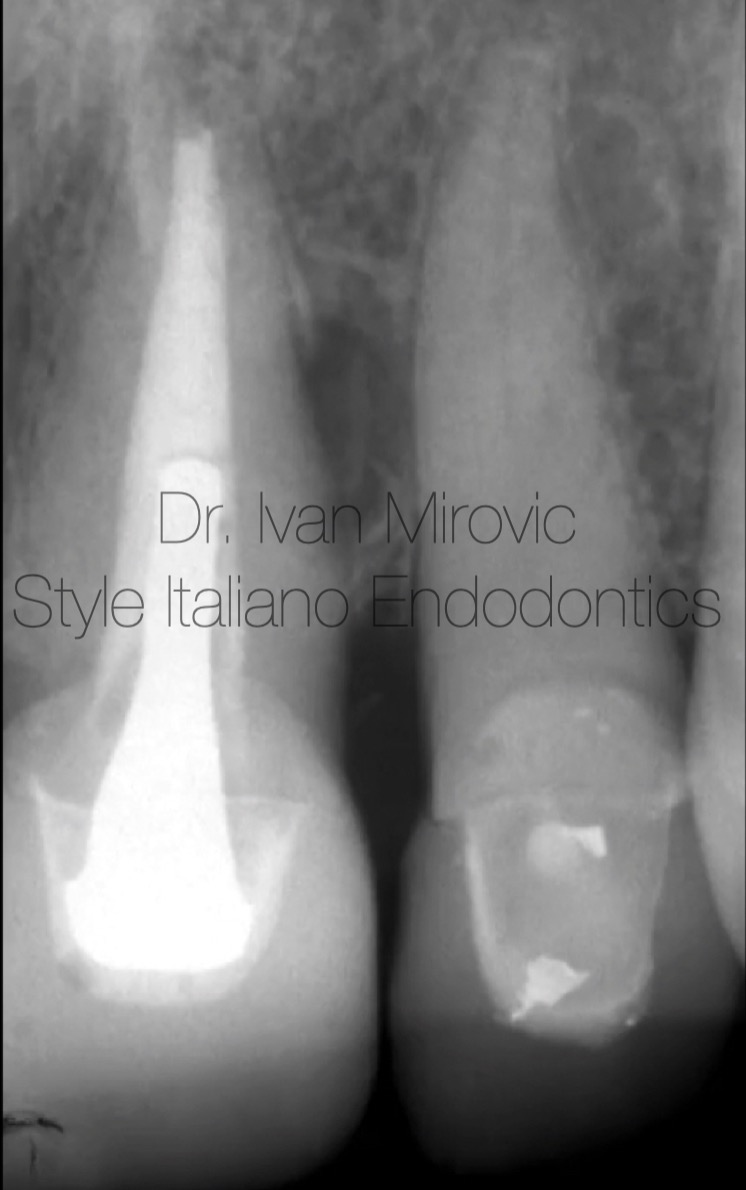
Fig. 6
Case of upper central incisor (Courtesy, Dr. Clifford J. Ruddle). The lesion was on the lateral side of the root. Notice the absence of lesion in the apical part. What was the reason of failure?
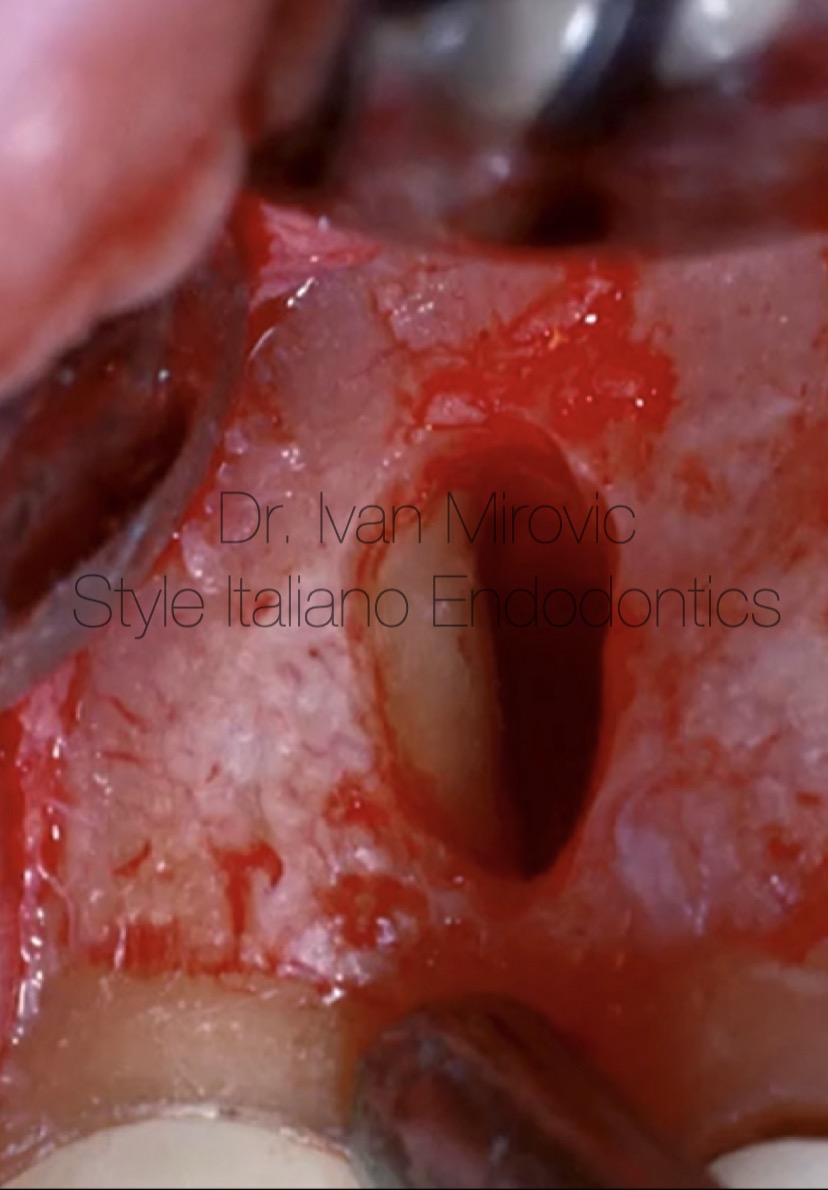
Fig. 7
After raising a flap it was obvious that treatment was failing because of untreated lateral canal.

Fig. 8
In this case lateral canal was treated with surgical approach.
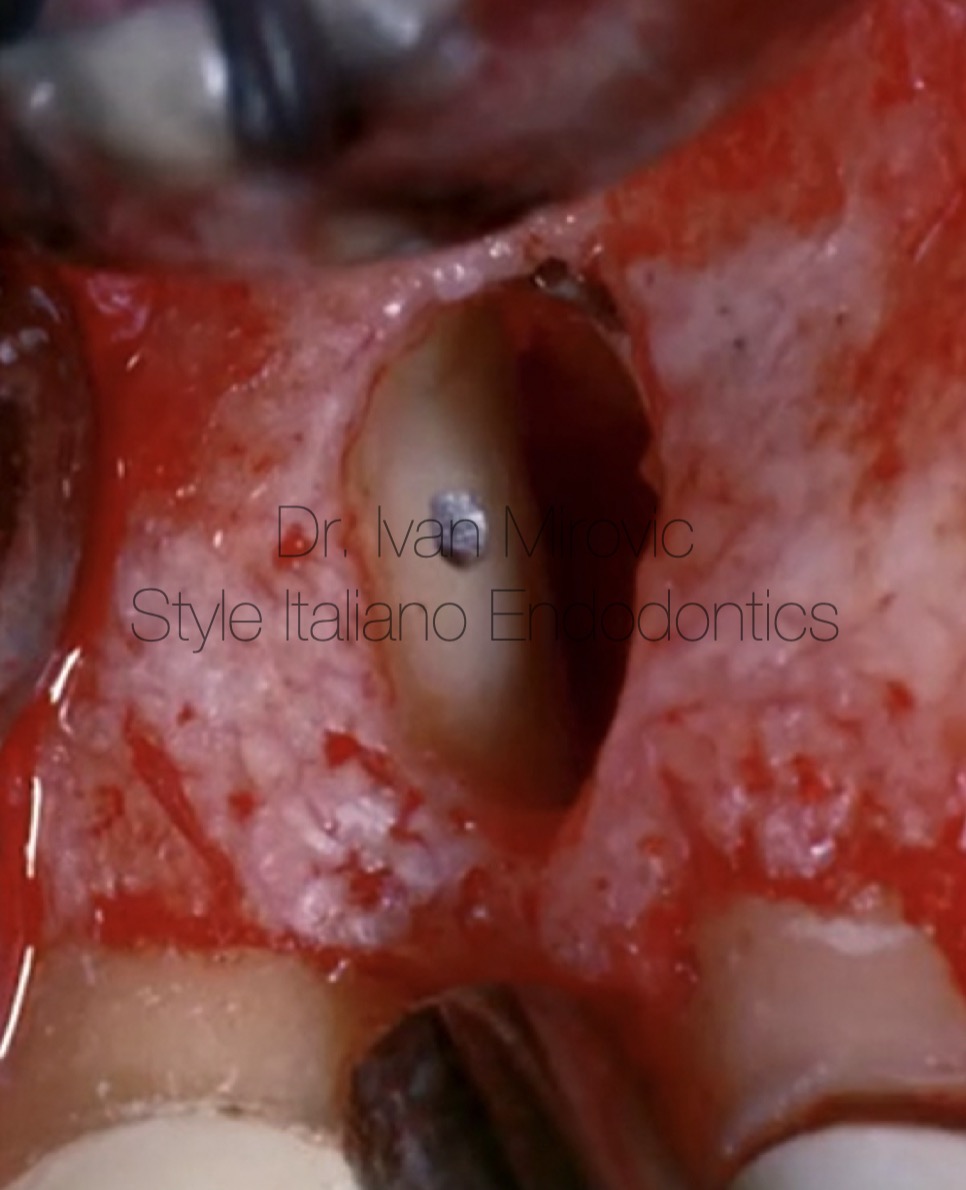
Fig. 9
Lateral canal filled with amalgam.

Fig. 10
Follow up radiograph shows complete healing.

Fig. 11
Pre operative radiograph of upper first molar with large lesion on palatal root.

Fig. 12
Post operative x ray demonstrates four portals of exit in palatal canal. Which one is important and which ones are not if the laterals do not matter? It is rational, from clinical and scientific point of view, that we want them all! Study by West found that all the failures (100 percent) demonstrated at least one underfilled portal of exit.

Fig. 13
Complete healing after one year.
Conclusions
Endodontics procedures should be directed towards complete cleaning of root canal systems followed by three dimensional obturation. Predictable success with poorly obturated root canal systems is not a clinical reality.
Bibliography
- Berutti E, Castelluci A: Cleaning and shaping the root canal system. In: Castellucci A, editor. Endodontics, Vol. II. Florence: Tridente S.r.l; 2006. p. 396-437
2. Schilder H. Filling root canals in three dimensions, Dent Clin North Am; 723-744, November 1967.
3. Ruddle CJ: Ch. 25, Nonsurgical endodontic retreatment. In Pathways of the Pulp, 8th ed., Cohen S, Burns RC, eds., St. Louis: Mosby, pp. 875-929, 2002
4. Ruddle CJ: Endodontic disinfection: tsunami irrigation, Endodontic Practice 11;1, pp. 7-15, 2008.
5. West JD. Endodontic failures marked by lack of three- dimensional seal.The Endodontic Report Fall/Winter: 9,1987.



