Complexity of the root canal system anatomy
18/01/2025
The Community
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
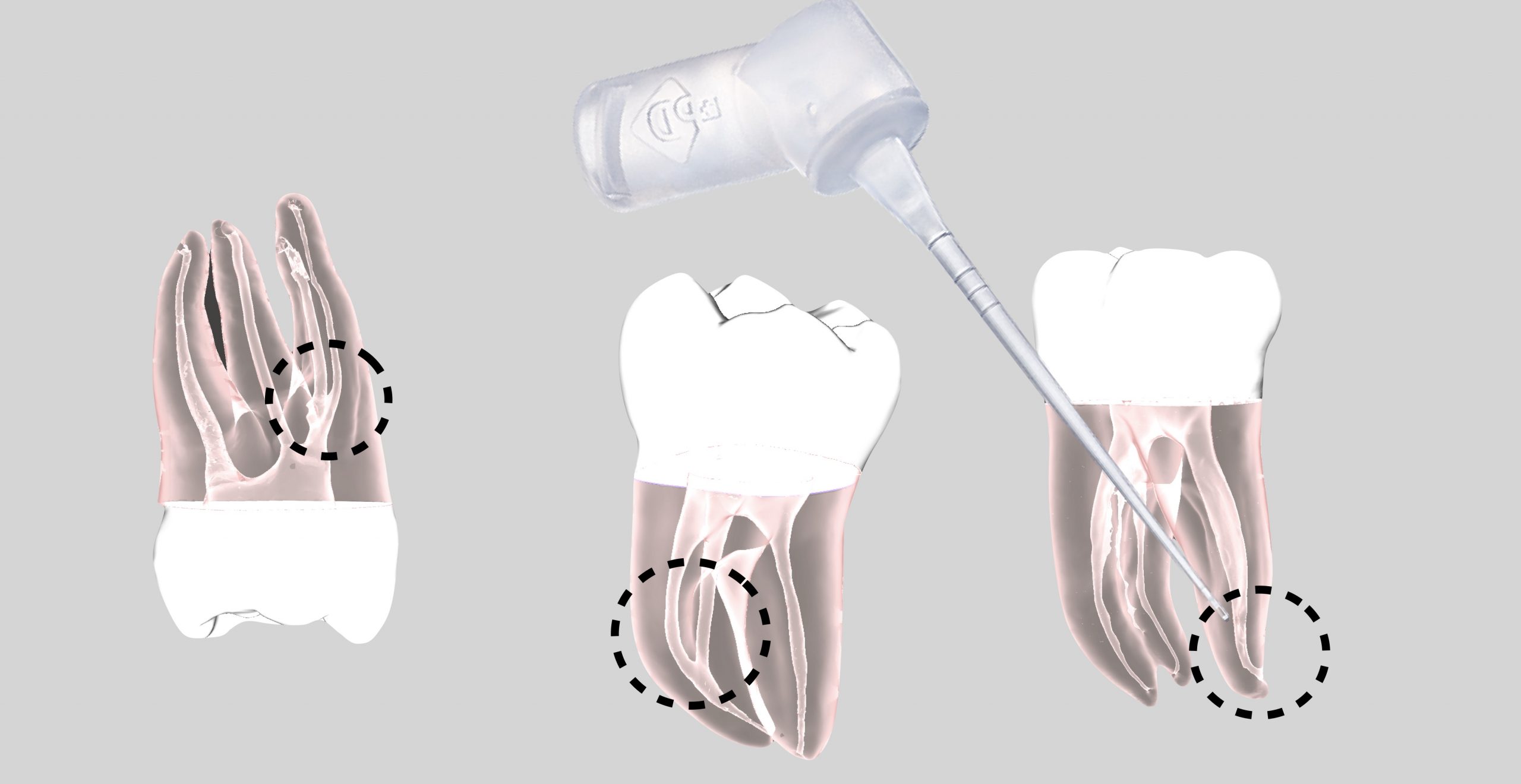
The main goal of root canal treatment is to eliminate the infection in the complex root canal system for the long-term preservation of a functional tooth. Proper debridement of the root canal system, especially in the apical portion, is essential for successful root canal treatment. The complexity of the canal anatomy in the apical region plays a crucial role in reducing the microbial load. clinicians must have a thorough knowledge of the anatomy of the root canal system and its variations, especially in the apical portion.(1)
However, this objective may be difficult to attain in reality because of the complexity of the internal anatomy of teeth. Residual bacteria and debris may remain relatively unaffected in the missed canal system or even in the unprepared canal walls, isthmuses, lateral canals, apical ramifications, and recesses from oval/flattened canals which may compromise the successful treatment outcome. Thus, a thorough understanding of the number of canals, of the inner-canal morphology, and the variations in all groups of teeth is a basic requirement for successful endodontic therapy.(2)
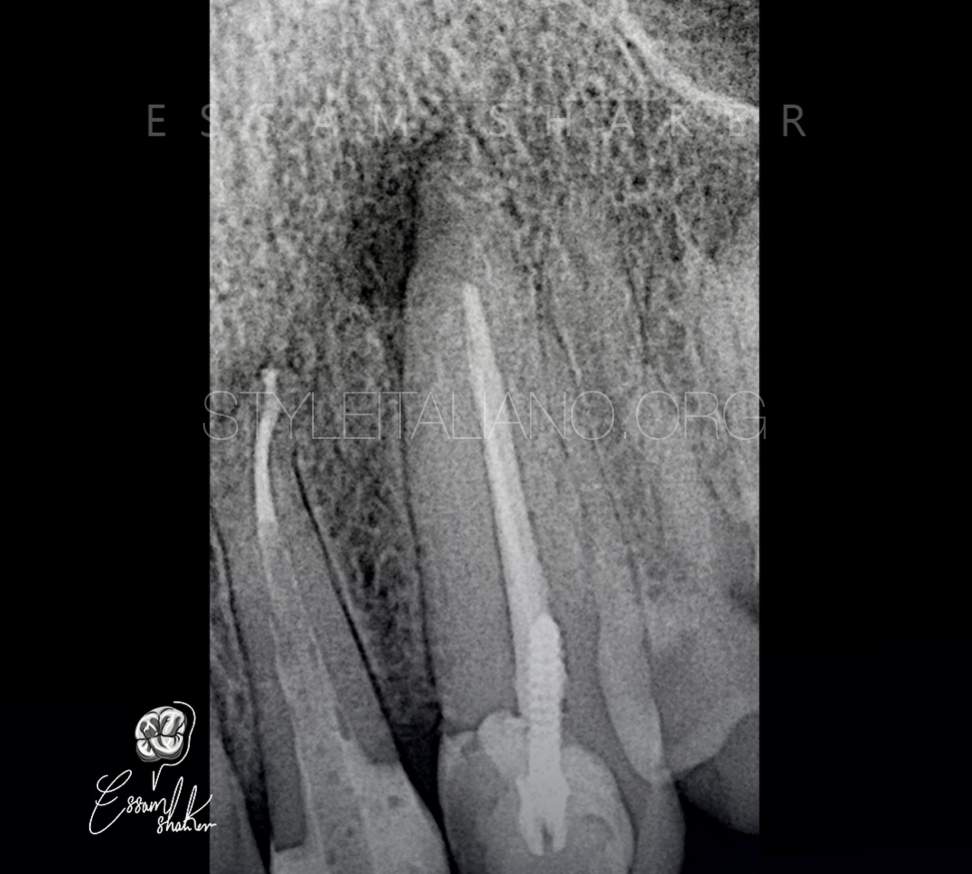
Fig. 1
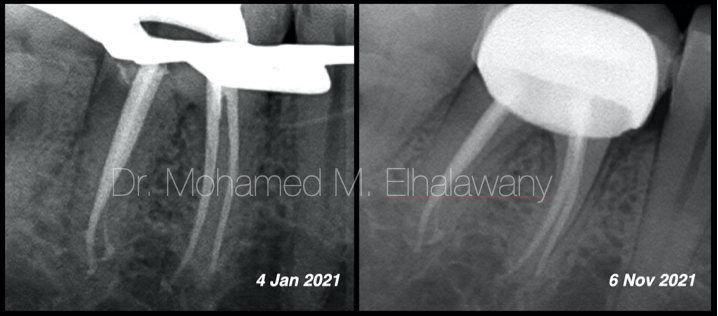
The 40 years old patient was referred to our office by his general dental practitioner for endodontic retreatment.
He complained about pain and discomfort associated with his upper left canine.
The preoperative radiographic showing lateral lesion related to the tooth, short fill obturation and metal screw.

Fig. 2
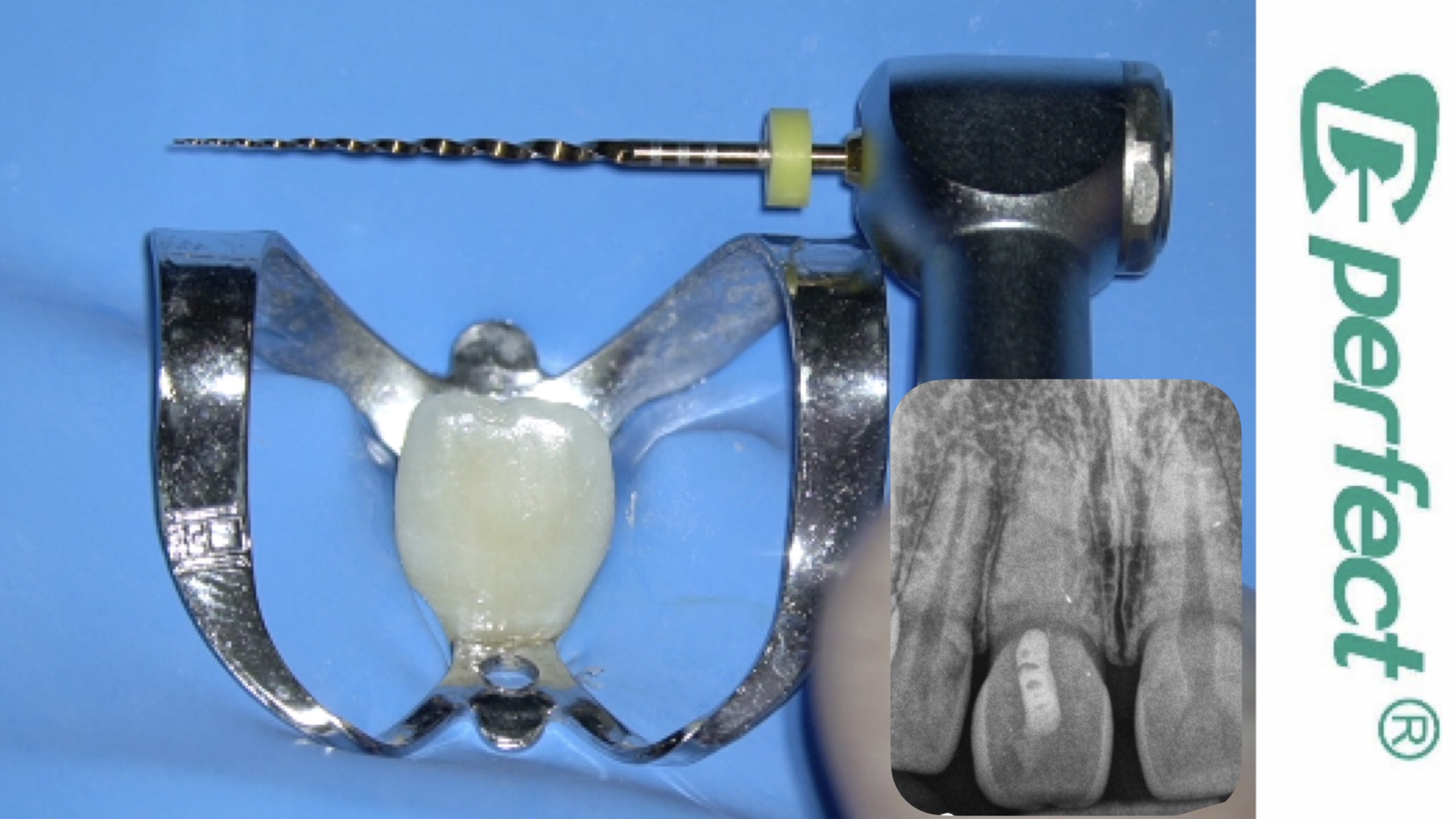
After local anesthesia administration, multiple isolation was applied with rubber dam by using two small wing clamps.
The access cavity was driven by removing the composite around the screw using round and fissure burs. Then, ultrasonic tips were used to remove all the composite that touches the screw.

Fig. 3
Clinical image after remove all the composite around the screw.
Ultrasonic vibration is one of the most common methods used to remove posts. The ultrasonic tip is used around the post in an anticlockwise direction to help loosen and unscrew it.
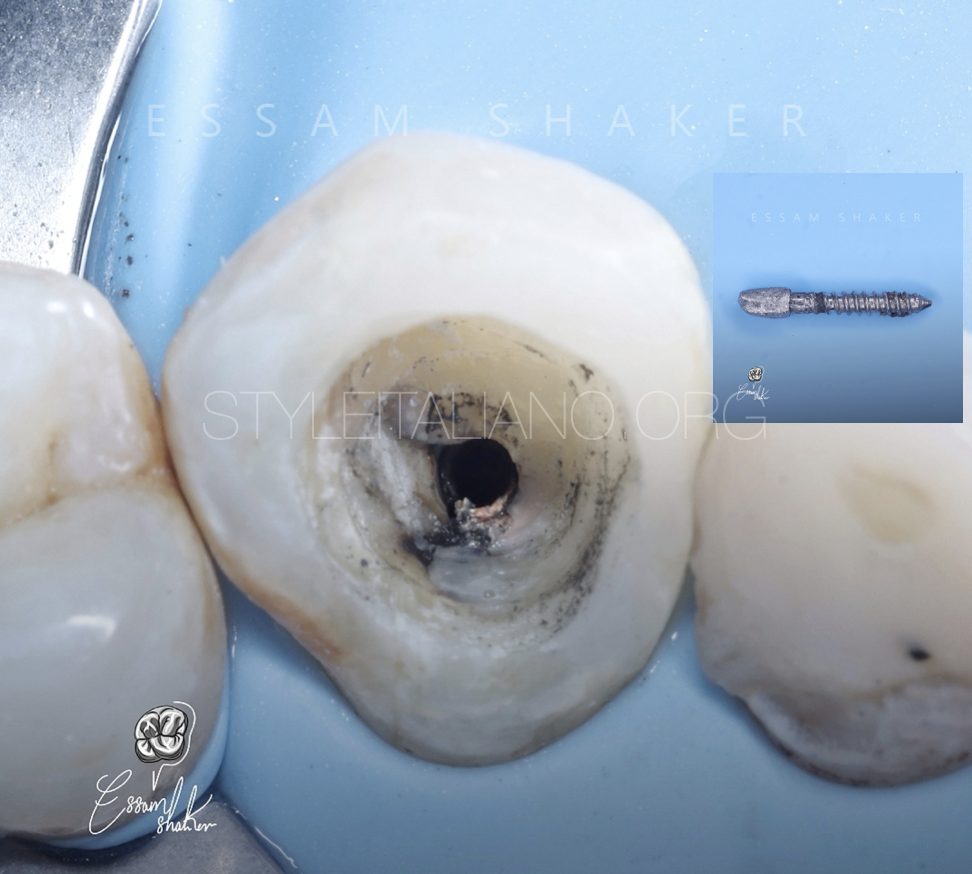
Fig. 4
Clinical image after remove the screw.
The old gutta percha in the coronal and middle third was removed with rotary files size 20/0.4% and 25/0.4%
After bypass the ledge in the apical third, the glide path achieved by using K files size 8,10,15.
The working length determined with apex locator and confirmed with IOPA radiograohy.
Then the canal was prepared and shaped with 25.06%
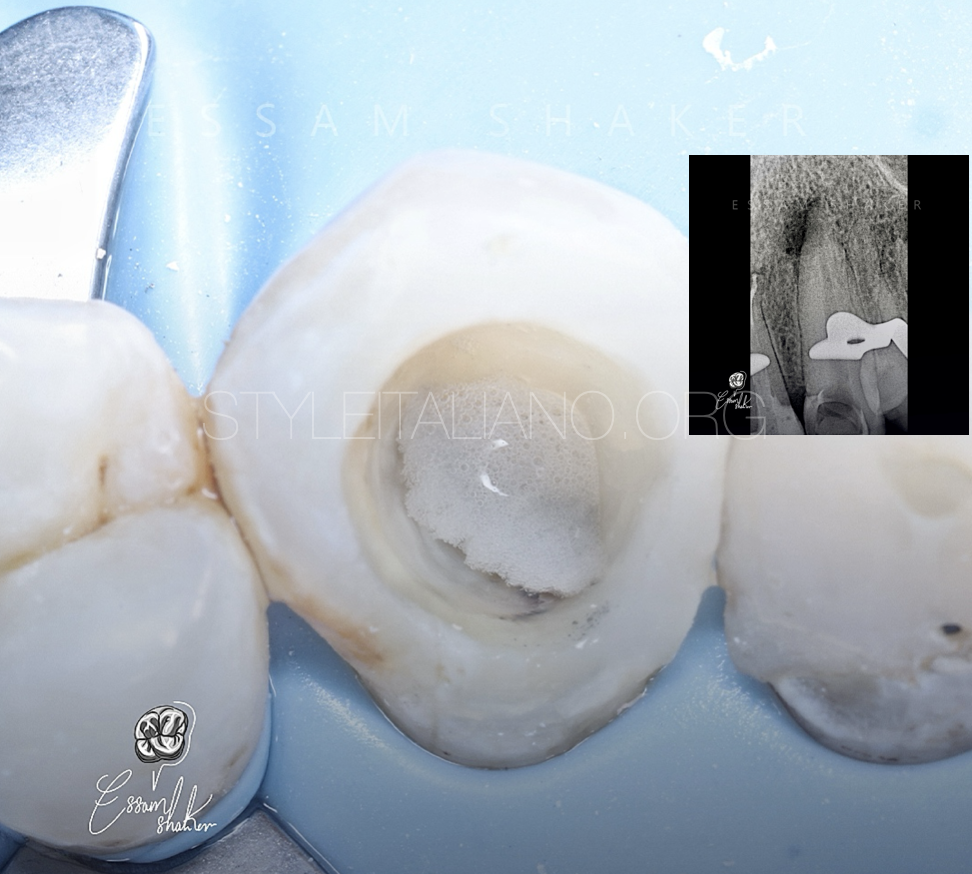
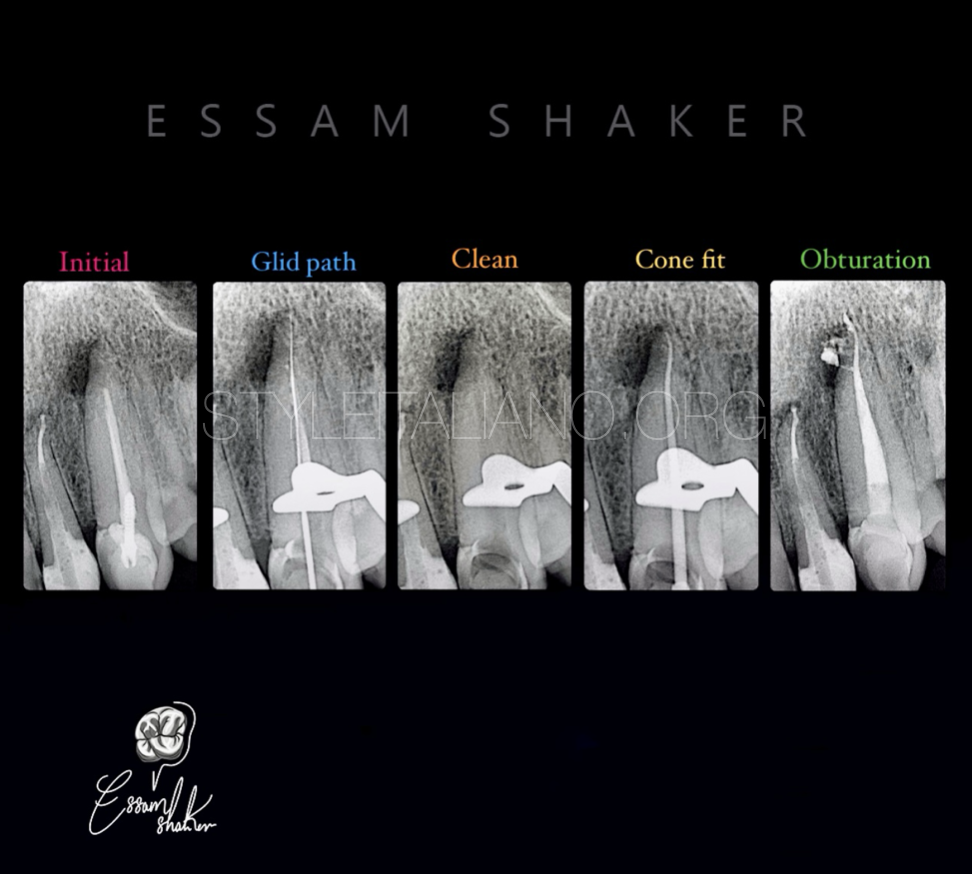
Fig. 5
Fig;5
In this case the effect of the good irrigation is undeniable. As shown, this was the irrigation protocol that relied on a group of irrigating materials in an orderly sequence to ensure good chemical cleaning of the root canal system, as each of this materials have a specific function.
Sodium hypochlorite 5,25% ( NaOCl ): the main irrigating solution used to dissolve organic matter and kill microbes effectively (3)
Ethylenediaminetetraacetic acid (EDTA): is needed as a final rinse to remove the smear layer.(12-15) But it has been used in this protocol more than once to ensure that the dentinal tubules are open to grantee that NaOCl well reach every point of root canal system.
saline: used between these two irrigants to avoid the chemical interaction between them(4)
It was necessary to guarantee the safety and not to pass any of these materials beyond the root apex, also a Gauge 30, double side vented irrigating needle was used to deliver the irrigating material to each canal in depth shorter than the working length by 3 mm.(5)
The activation of irrigant was done by using an ultrasonic activator, the duration of each activation last for 20 sec.(6)
The image shows the tooth immediately after sodium hypochlorite activation.

Fig. 6
Clinical image and radiographic image show the cone fit.

Fig. 7
The obturation done with modified hydraulic obturation with premixed Bioceramic cement.

Fig. 8
Single appointment root canal retreatments presented a favorable success rate. Only preoperative lesion size had a significant effect on on the outcome where the lesions small than 5mm performed significantly better healing(7).
Clinical image after complete the obturation in single appointment.
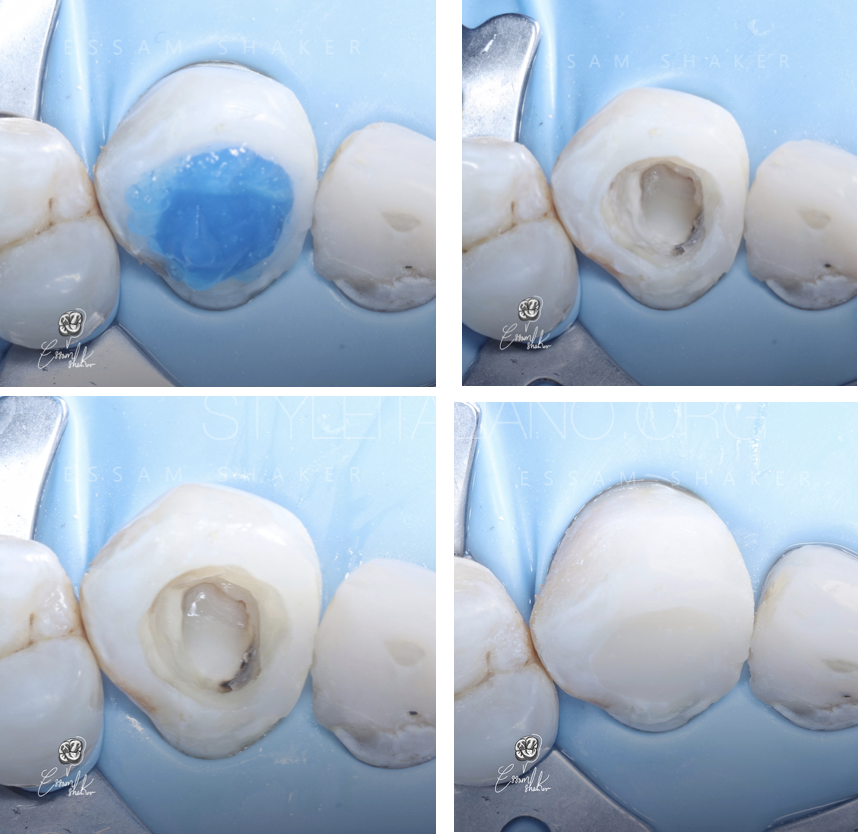
Fig. 9
Restore the tooth with a direct composite restoration in the same appointment.
Fig. 10
Anatomical abnormalities of the root canal system are frequently seen in specialist endodontic practice, and represent a challenge to be faced with skill and thoroughness, beginning with an accurate diagnostic phase and devising the most appropriate treatment plan. Fortunately, much progress has been made in endodontic research thanks to technological advances and the evolution of higher performance instruments, which now consent even very complex cases to be resolved with relative ease(8).

Fig. 11
Dr. ISAM SHAKIR ALWAN
.Graduated with BDS from University of Alkafeel in 2021.
.My passion in Endodontics started during my training at university.
Have certificate many courses in basic, advanced Endodontics and Endodontics microsurgery.
Key Opinion Leader for MARUCHI.
My work is committed to microscopic Endodontics and aesthetic dentistry.
Conclusions
The case report may demonstrate that the effect unobturated lateral canal can participate in failure of root canal treatment, especially that the lesion was in a proximity to a lateral canal in the radiograph. To overcome such a problem, magnification and ultrasonic devices are mandatory. In addition, bioceramic materials may have a significant rule in perfect 3D obturation complex root canal systems.
Bibliography
1-Mamat R, Nik Abdul Ghani NR. The Complexity of the Root Canal Anatomy and Its Influence on Root Canal Debridement in the Apical Region: A Review. Cureus. 2023 Nov 18;15(11):e49024. doi: 10.7759/cureus.49024. PMID: 38111413; PMCID: PMC10727774.
2-Ahmed HMA, Ibrahim N, Mohamad NS, Nambiar P, Muhammad RF, Yusoff M, Dummer PMH. Application of a new system for classifying root and canal anatomy in studies involving micro-computed tomography and cone beam computed tomography: Explanation and elaboration. Int Endod J. 2021 Jul;54(7):1056-1082. doi: 10.1111/iej.13486. Epub 2021 Apr 18. PMID: 33527452.
3-Haapasalo M, Shen Y, Wang Z, Gao Y. Irrigation in endodontics. Br Dent J. 2014 Mar;216(6):299-303. doi: 10.1038/sj.bdj.2014.204. PMID: 24651335.
4-Prado M, Santos Júnior HM, Rezende CM, Pinto AC, Faria RB, Simão RA, Gomes BP. Interactions between irrigants commonly used in endodontic practice: a chemical analysis. J Endod. 2013 Apr;39(4):505-10. doi: 10.1016/j.joen.2012.11.050. Epub 2013 Jan 30. PMID: 23522546.
5-Uzunoglu-Özyürek E, Karaaslan H, Türker SA, Özçelik B. Influence of size and insertion depth of irrigation needle on debris extrusion and sealer penetration. Restor Dent Endod. 2017 Dec 22;43(1):e2. doi: 10.5395/rde.2018.43.e2. PMID: 29487833; PMCID: PMC5816991.
6-Nagendrababu V, Jayaraman J, Suresh A, Kalyanasundaram S, Neelakantan P. Effectiveness of ultrasonically activated irrigation on root canal disinfection: a systematic review of in vitro studies. Clin Oral Investig. 2018 Mar;22(2):655-670. doi: 10.1007/s00784-018-2345-x. Epub 2018 Jan 25. PMID: 29372445.
7-Eyuboglu TF, Olcay K, Özcan M. A clinical study on single-visit root canal retreatments on consecutive 173 patients: frequency of periapical complications and clinical success rate. Clin Oral Investig. 2017 Jun;21(5):1761-1768. doi: 10.1007/s00784-016-1957-2. Epub 2016 Sep 22. PMID: 27660159.
8-Migliau G, Pepla E, Besharat LK, Gallottini L. Resolution of endodontic issues linked to complex anatomy. Ann Stomatol (Roma). 2014 Mar 31;5(1):34-40. PMID: 24753800; PMCID: PMC3974551.