It’s all about Irrigation: Case Report
20/01/2022
The Community
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
A case report with 10 months follow up showing the effect of good irrigation protocol on the final result of the root canal treatment.
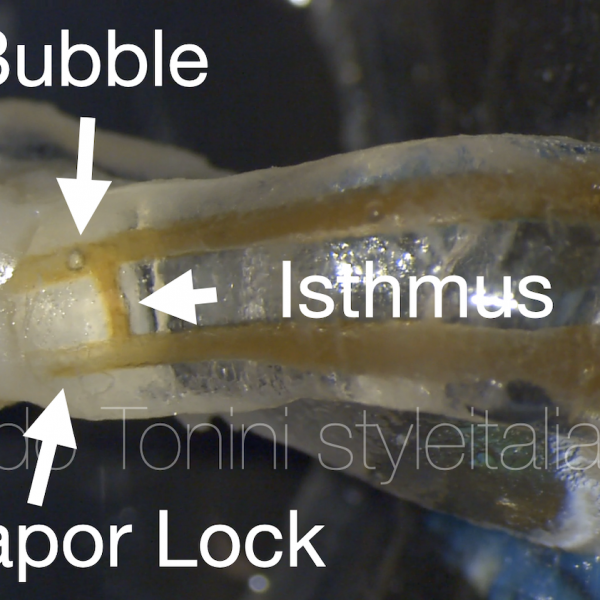
The aim of root canal treatment is to prevent and treat apical periodontitis , with the objective of eliminating microorganisms and necrotic pulp through chemo-mechanical debridement, and providing an adequate root filling in order to seal the canals and prevent reinfection (1,2). However, this objective may be difficult to attain in reality because of the complexity of the internal anatomy of teeth. Residual bacteria and debris may remain relatively unaffected in the missed canal system or even in the unprepared canal walls, isthmuses, lateral canals, apical ramifications, and recesses from oval/flattened canals which may compromise the successful treatment outcome. Thus, a thorough understanding of the number of canals, of the inner-canal morphology, and the variations in all groups of teeth is a basic requirement for successful endodontic therapy. (3)
Anatomical abnormalities of the root canal system are frequently seen in specialist endodontic practice, and represent a challenge to be faced with skill and thoroughness, beginning with an accurate diagnostic phase and devising the most appropriate treatment plan. Fortunately, much progress has been made in endodontic research thanks to technological advances and the evolution of higher performance instruments, which now consent even very complex cases to be resolved with relative ease. (4)

Fig. 1
A 51-year-old female patient was suffering from persistent severe pain from lower right first molar (#46 when shaving any cold fluids, the pain increases severely and may last for a long period of up to an hour. She had these symptoms for many months before the pain intensified and made her wake up from sleep, and she was taking a lot of painkillers, which caused her also gastritis (5) . As for consuming warm drinks, the pain is present, but it does not last for a long time, as it happens from its cold counterpart.
Suddenly the analgesics did not have any effect, but the intake of cold liquids also made the pain disappear completely for a period of several minutes. This prompted her to go to the dentist on the same day.
During clinical examination, it was found that the patient had not any carious lesion at occlusal surface of tooth #46, but by examination of inter-proximal surfaces a large deep distal cavity was found which was confirmed by x-ray . Patient had also pain with percussion.
All of this are typical signs and symptoms of irreversible pulpitis (6) which require pulpectomy and root canal filling, because inflamed vital pulp is not capable of healing. (7)
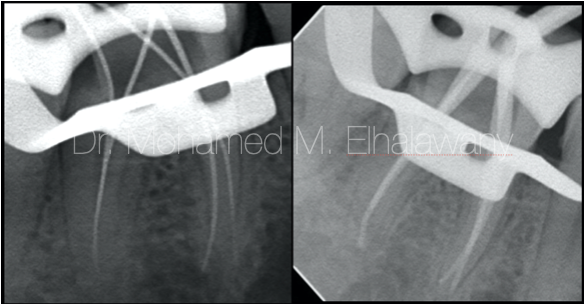
Fig. 2
The treatment of this molar was completed in one session, since in the beginning most of the caries was removed but without complete deroofing of pulp chamber to avoid contamination.(8) And then a complete isolation was done using Rubber dam in-addition to use a liquid dam which is very helpful in sealing off any areas that may have any seepage.(8,9) Complete the pulp chamber opening to make a traditional access opening then the access was refined by using ultrasonic tips leading to the discovery of the four root canals orifices. By using the Apex Locator Working length was measured then it was confirmed using x-rays.
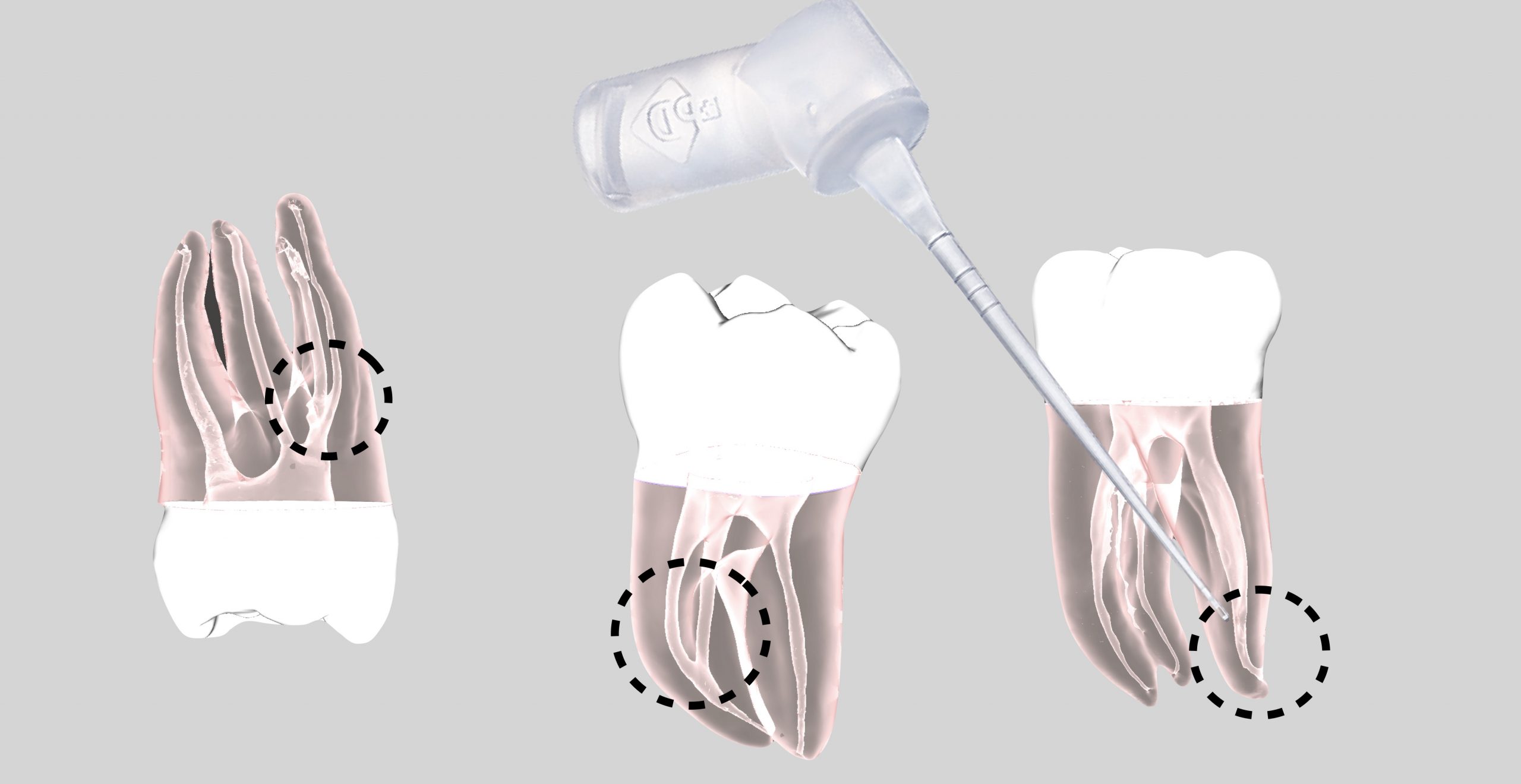
During the Chemo-mechanical preparation of the canals, it was noticed that the Canals were wider in the coronal two thirds in comparison with apical third specially in the distal root, in addition the canal orifices of the distal root was close to each other which puts a high probability that these canals have two orifices and one apex (Type II )(10), and this is what was discovered to be true during preparation
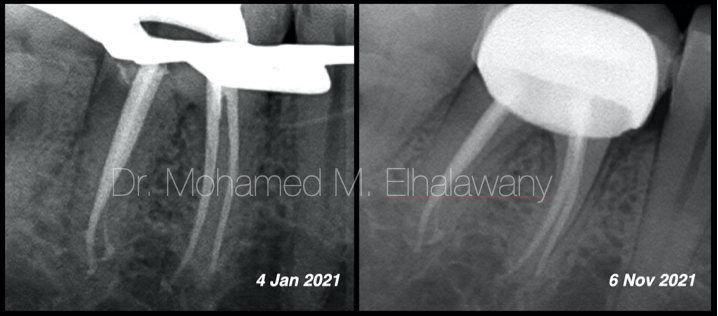
On the Master Cone x-ray، everything seemed fine, so the tooth was obturated using single cone with calcium silicate-based bioceramic sealer and modified vertical compaction.
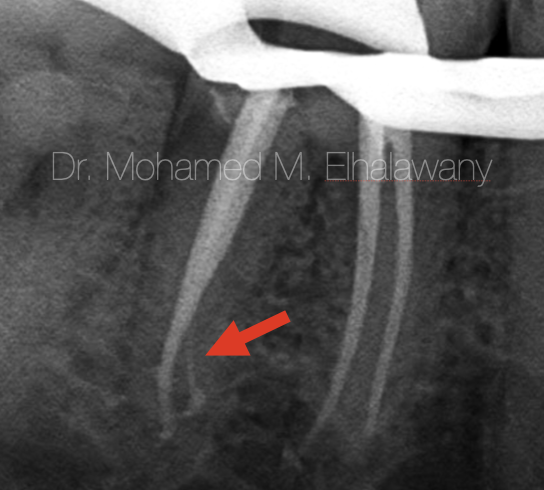
Fig. 3
It was a big shock when examining the post-operative x-rays, as it is clear in the x-rays, the red arrow indicates the presence of a thin canal that was filled by the bioceramic sealer only, Which means that it was cleaned only chemically thanks to the penetration of the irrigating materials and not mechanically by files. which raised a lot of questions:
- Were the two distal canals completely separate (type IV)(10) and did not have the same apex as was believed during the preparation procedure?
- May be was it an accessory canal that was chemically cleaned well .
Many possibilities which need further examination in order to clarify the problem “ if exist” . As each scenario has a different way to deal with it. So for better tooth evaluation,CBCT is requested (34).
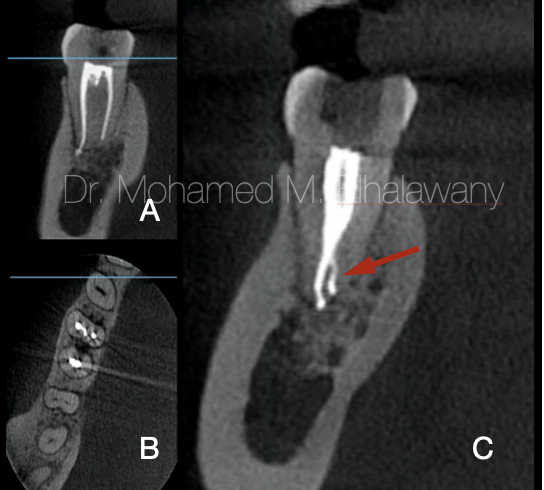
Fig. 4
By means of the CBCT, the entire molar was examined to ensure the quality of preparation for the canals as well as the obturation.
- Coronal view for mesial root shows only two canals which seems to be good prepared and obturated up to the apex.
- Axial view : MBa canal is obturated with its isthmus, the two distal canals are so close to appear one large canal.
- Coronal view for Distal root approve that the canal anatomy Type II (two canals with one apex) in addition to small lingual accessory canal ( red arrow ) .
According to the CBCT analysis result : That canal was an accessory canal that thanks to good irrigation protocol, it was cleaned and duo to the good follow of bioceramic sealer, it was good obturated (33) .
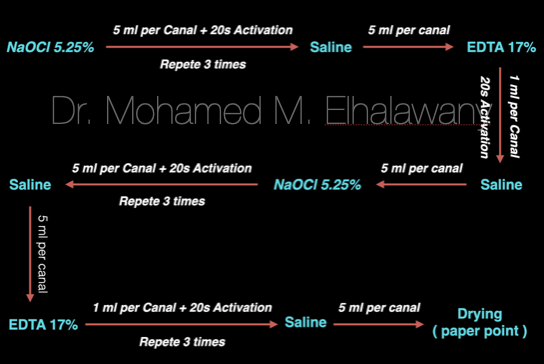
Fig. 5
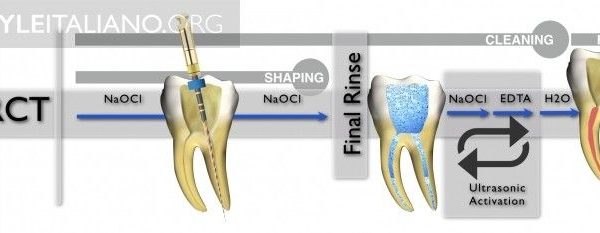
In this case the effect of the good irrigation is undeniable. As shown, this was the irrigation protocol that relied on a group of irrigating materials in an orderly sequence to ensure good chemical cleaning of the root canal system, as each of this materials have a specific function.
Sodium hypochlorite 5,25% ( NaOCl ): the main irrigating solution used to dissolve organic matter and kill microbes effectively (12-15)
Ethylenediaminetetraacetic acid (EDTA): is needed as a final rinse to remove the smear layer.(12-15) But it has been used in this protocol more than once to ensure that the dentinal tubules are open to grantee that NaOCl well reach every point of root canal system.
saline: used between these two irrigants to avoid the chemical interaction between them(12,14)
It was necessary to guarantee the safety and not to pass any of these materials beyond the root apex, also a Gauge 30, double side vented irrigating needle was used to deliver the irrigating material to each canal in depth shorter than the working length by 3 mm.(16)
The activation of irrigant was done by using an ultrasonic activator, the duration of each activation last for 20 sec.(11)

Fig. 6
The author: Dr. Mohamed M. Elhalawany
Conclusions
Irrigation is a key part of successful root canal treatment. It has several important functions, which may vary according to the irrigant used: it reduces friction between the instrument and dentine, improves the cutting effectiveness of the files, dissolves tissue, cools the file and tooth, and furthermore, it has a washing effect and an antimicrobial/antibiofilm effect. Irrigation is also the only way to impact those areas of the root canal wall not touched by mechanical instrumentation.(17)
Much of the research on endodontic irrigation has focused on the effect of irrigation on the smear layer.(17-21) However, smear layer removal can be accomplished relatively easily when correct protocols are followed. A bigger challenge for irrigation may be the areas untouched by the files, such as fins, isthmuses and large lateral canals.(22) Also, large areas in the oval and flat canals may remain untouched despite careful instrumentation. These areas contain tissue remnants and biofilms that only can be removed by chemical means using irrigation. The apical root canal poses a special challenge to irrigation as the balance between safety and effectiveness is particularly important in this area. (23) Small, 30-gauge side-vented needles and/or negative pressure irrigation in the apical canal will secure the best results in this important area.
Ultrasonic irrigation using ultrasonic tips to deliver the solutions directly into the canal space have shown promising results for cleaning even the most difficult areas such as long and narrow isthmuses between two canals.( 24-26)
Sodium hypochlorite (NaOCl) is the most important irrigant in root canal treatment.(27-29) It is the only presently used solution that can dissolve organic matter in the canal. Therefore the use of hypochlorite is of utmost importance in removing necrotic tissue remnants as well as biofilm. (30-32)
Bibliography
- Colombo M, Bassi C, Beltrami R, Vigorelli P, Spinelli A, Cavada A, Dagna A, Chiesa M, Poggio C. Radiographic technical quality of root canal treatment performed by a new rotary single-file system. Ann Stomatl (Roma). 2017 Jul 3;8(1):18-22. doi: 10.11138/ads/2017.8.1.018. PMID: 28736602; PMCID: PMC5507162.
- Chugal NM, Clive JM, Spangberg LSW. Endodontic infection: some biologic and treatment factors associated with outcome. Oral Surg, Oral Med, Oral Pathol, Oral Radiol and Endod. 2003;96:81–90.
- H. M. A. Ahmed, N. Ibrahim, N. S. Mohamad, P. Nambiar, R. F. Muhammad, M. Yusoff, P. M. H. Dummer, Application of a new system for classifying root and canal anatomy in studies involving micro‐computed tomography and cone beam computed tomography: Explanation and elaboration, International Endodontic Journal, 10.1111/iej.13486, 54, 7, (1056-1082), (2021).
- Migliau G, Pepla E, Besharat LK, Gallottini L. Resolution of endodontic issues linked to complex anatomy. Ann Stomatol (Roma). 2014 Mar 31;5(1):34-40. PMID: 24753800; PMCID: PMC3974551.
- Benyamin R, Trescot AM, Datta S, Buenaventura R, Adlaka R, Sehgal N, Glaser SE, Vallejo R. Opioid complications and side effects. Pain Physician. 2008 Mar;11(2 Suppl):S105-20. PMID: 18443635.
- Bender IB. Reversible and irreversible painful pulpitides: diagnosis and treatment. Aust Endod J. 2000 Apr;26(1):10-4. doi: 10.1111/j.1747-4477.2000.tb00144.x. PMID: 11359291.
- Lin LM, Ricucci D, Saoud TM, Sigurdsson A, Kahler B. Vital pulp therapy of mature permanent teeth with irreversible pulpitis from the perspective of pulp biology. Aust Endod J. 2020 Apr;46(1):154-166. doi: 10.1111/aej.12392. Epub 2019 Dec 21. PMID: 31865629.
- EUROPEAN SOCIETY OF ENDODONTOLOGY: Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int. Endod. J. 39:921-30, 2006.
- Lin PY, Huang SH, Chang HJ, Chi LY. The effect of rubber dam usage on the survival rate of teeth receiving initial root canal treatment: a nationwide population-based study. J Endod. 2014 Nov;40(11):1733-7. doi: 10.1016/j.joen.2014.07.007. Epub 2014 Aug 28. PMID: 25175849.
- Torres, Andres & Jacobs, Reinhilde & Lambrechts, Paul & Brizuela, Claudia & Cabrera, Carolina & Concha, Guillermo & Pedemonte, María. (2015). Characterization of mandibular molar root and canal morphology using cone beam computed tomography and its variability in Belgian and Chilean population samples. Imaging science in dentistry. 45. 95-101. 10.5624/isd.2015.45.2.95.
- Nagendrababu V, Jayaraman J, Suresh A, Kalyanasundaram S, Neelakantan P. Effectiveness of ultrasonically activated irrigation on root canal disinfection: a systematic review of in vitro studies. Clin Oral Investig. 2018 Mar;22(2):655-670. doi: 10.1007/s00784-018-2345-x. Epub 2018 Jan 25. PMID: 29372445.
- Haapasalo M, Shen Y, Wang Z, Gao Y. Irrigation in endodontics. Br Dent J. 2014 Mar;216(6):299-303. doi: 10.1038/sj.bdj.2014.204. PMID: 24651335.
- Kandaswamy D, Venkateshbabu N. Root canal irrigants. J Conserv Dent. 2010 Oct;13(4):256-64. doi: 10.4103/0972-0707.73378. PMID: 21217955; PMCID: PMC3010032.
- Prado M, Santos Júnior HM, Rezende CM, Pinto AC, Faria RB, Simão RA, Gomes BP. Interactions between irrigants commonly used in endodontic practice: a chemical analysis. J Endod. 2013 Apr;39(4):505-10. doi: 10.1016/j.joen.2012.11.050. Epub 2013 Jan 30. PMID: 23522546.
- Chubb DWR. A review of the prognostic value of irrigation on root canal treatment success. Aust Endod J. 2019 Apr;45(1):5-11. doi: 10.1111/aej.12348. PMID: 30980478.
- Uzunoglu-Özyürek E, Karaaslan H, Türker SA, Özçelik B. Influence of size and insertion depth of irrigation needle on debris extrusion and sealer penetration. Restor Dent Endod. 2017 Dec 22;43(1):e2. doi: 10.5395/rde.2018.43.e2. PMID: 29487833; PMCID: PMC5816991.
- Haapasalo, M., Shen, Y., Wang, Z. et al. Irrigation in endodontics. Br Dent J 216, 299–303 (2014). https://doi.org/10.1038/sj.bdj.2014.204
- Loel D A . Use of acid cleanser in endodontic therapy. J Am Dent Assoc 1975; 90: 148–151.
- Baumgartner J C, Brown C M, Mader C L, Peters D D, Shulman J D . A scanning electron microscopic evaluation of root canal debridement using saline, sodium hypochlorite, and citric acid. J Endod 1984; 10: 525–531.
- Baumgartner J C, Mader C L . A scanning electron microscopic evaluation of four root canal irrigation regimens. J Endod 1987; 13: 147–157.
- Czonstkowsky M, Wilson E G, Holstein F A . The smear layer in endodontics. Dent Clin North Am 1990; 34: 13–25.
- Haapasalo M, Shen Y, Qian W, Gao Y . Irrigation in endodontics. Dent Clin North Am 2010; 54: 291–312.
- Park E, Shen Y, Khakpour M, Haapasalo M . Apical pressure and extent of irrigant flow beyond the needle tip during positive-pressure irrigation in an in vitro root canal model. J Endod 2013; 39: 511–515.
- Carr G B, Schwartz R S, Schaudinn C, Gorur A, Costerton J W . Ultrastructural examination of failed molar retreatment with secondary apical periodontitis: an examination of endodontic biofilms in an endodontic retreatment failure. J Endod 2009; 35: 1303–1309.
- Klyn S L, Kirkpatrick T C, Rutledge R E . In vitro comparisons of debris removal of the EndoActivator system, the F file, ultrasonic irrigation, and NaOCl irrigation alone after hand-rotary instrumentation in human mandibular molars. J Endod 2010; 36: 1367–1371.
- Johnson M, Sidow S J, Looney S W, Lindsey K, Niu L N, Tay F R . Canal and isthmus debridement efficacy using a sonic irrigation technique in a closed-canal system. J Endod 2012; 38: 1265–1268.
- Siqueira JF Jr, Rôças I N, Favieri A, Lima K C . Chemomechanical reduction of the bacterial population in the root canal after instrumentation and irrigation with 1%, 2.5%, and 5.25% sodium hypochlorite. J Endod 2000; 26: 331–334.
- Dunavant T R, Regan J D, Glickman G N, Solomon E S, Honeyman A L . Comparative evaluation of endodontic irrigants against Enterococcus faecalis biofilms. J Endod 2006; 32: 527–531.
- Williamson A E, Cardon J W, Drake D R . Antimicrobial susceptibility of monoculture biofilms of a clinical isolate of Enterococcus faecalis. J Endod 2009; 35: 95–97.
- Beltz R E, Torabinejad M, Pouresmail M . Quantitative analysis of the solubilizing action of MTAD, sodium hypochlorite, and EDTA on bovine pulp and dentin. J Endod 2003; 29: 334–337.
- Cobankara F K, Ozkan H B, Terlemez A . Comparison of organic tissue dissolution capacities of sodium hypochlorite and chlorine dioxide. J Endod 2010; 36: 272–274.
- Stojicic S, Zivkovic S, Qian W, Zhang H, Haapasalo M . Tissue dissolution by sodium hypochlorite: effect of concentration, temperature, agitation, and surfactant. J Endod 2010; 36: 1558–1562
- Kharouf, Naji, Youri Arntz, Ammar Eid, Jihed Zghal, Salvatore Sauro, Youssef Haikel, and Davide Mancino. 2020. "Physicochemical and Antibacterial Properties of Novel, Premixed Calcium Silicate-Based Sealer Compared to Powder–Liquid Bioceramic Sealer" Journal of Clinical Medicine 9, no. 10: 3096. https://doi.org/10.3390/jcm9103096
- Use of Cone Beam Computed Tomography in Endodontics, William C. Scarfe, Martin D. Levin, David Gane, Allan G. Farman, Int J Dent. 2009; 2009: 634567. Published online 2010 Mar 31. doi: 10.1155/2009/634567., PMCID: PMC2850139