
Does anatomy represent a limit for root canal disinfection?
05/04/2021
Riccardo Tonini
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
From a recent Randomized clinical trial (Comparison of the Effect of Two Endodontic Irrigation Protocols on the Elimination of Bacteria from Root Canal System: A Prospective, Randomized Clinical Trial) it was demonstrated that "there was no statistical difference between irrigation methods. Each protocol resulted in a high frequency of negative cultures. This high frequency of negative cultures obtained in 1 visit is most likely related to an increased volume and depth of irrigation compared with previously reported protocols”.
It is evident that the key is given by the capability of our Irrigants to penetrate in the apical region in a repeatable way and that the liquid exchange/refill is really important in order to avoid the buffering effect.
Aim of this article is to test IrriFlex, a 30G needle made of polypropylene with a back-to-back 2-side vent design, in different clinical conditions such as curved anatomies, .06 and .04 taper canal preparation and wide canals.
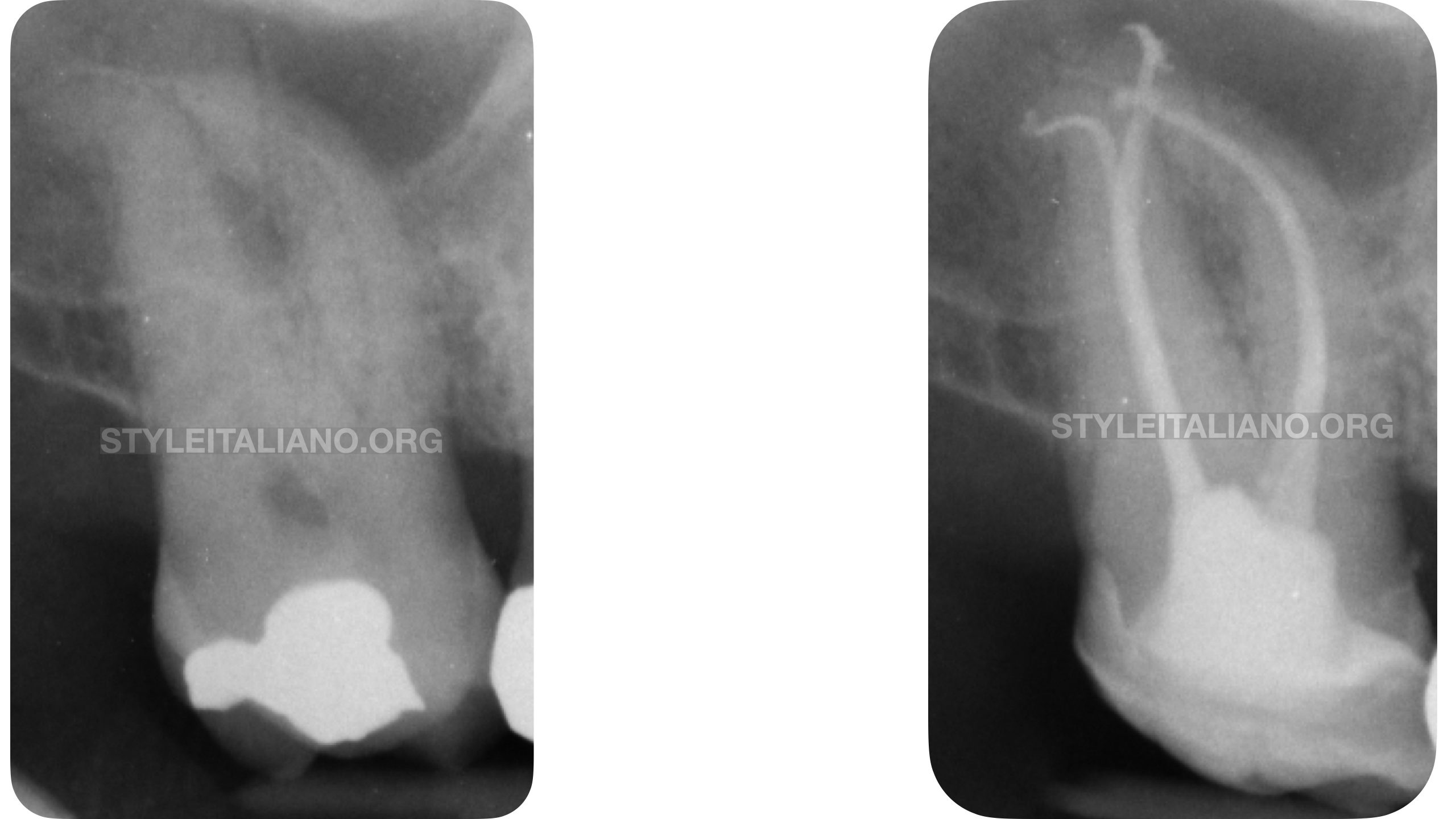
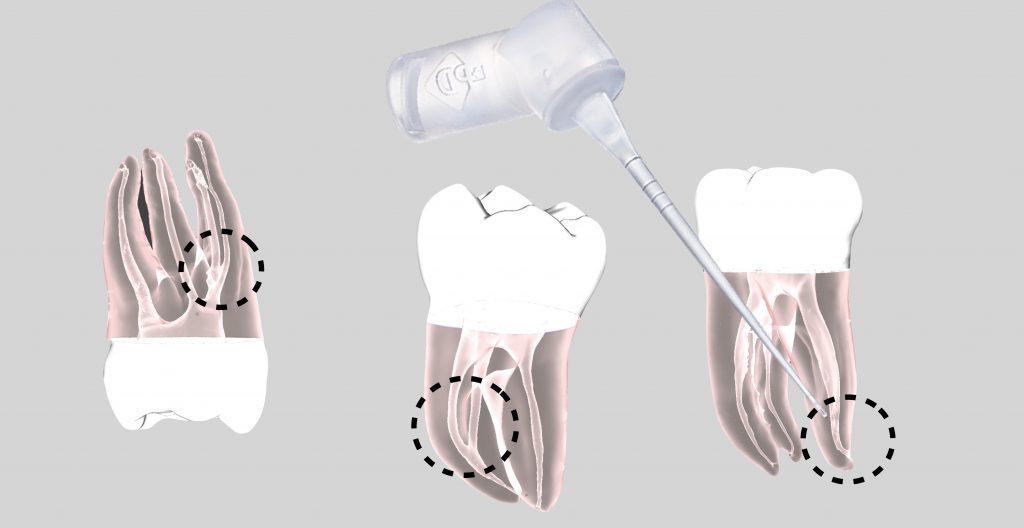
Fig. 1
The objective of a correct disinfection is to reach with IrriFlex an ideal penetration length 2mm shorter than WL. This condition guarantees liquid extrusion in the apical region and a safe control of liquid expulsion.
Curvature location is probably the main limit that a needle could find inside the root canal system. A coronal curvature represents the worst situation, because usually a metal needle is always stuck at the beginning of the radius of curvature.
At the same time, a great limitation is given by the taper of the RCS. A small taper as .04 could be a limit for an ideal needle penetration. The opposite situation happens when we face a wide canal: in this case the risk is more related to the extrusion of liquids over the apex.
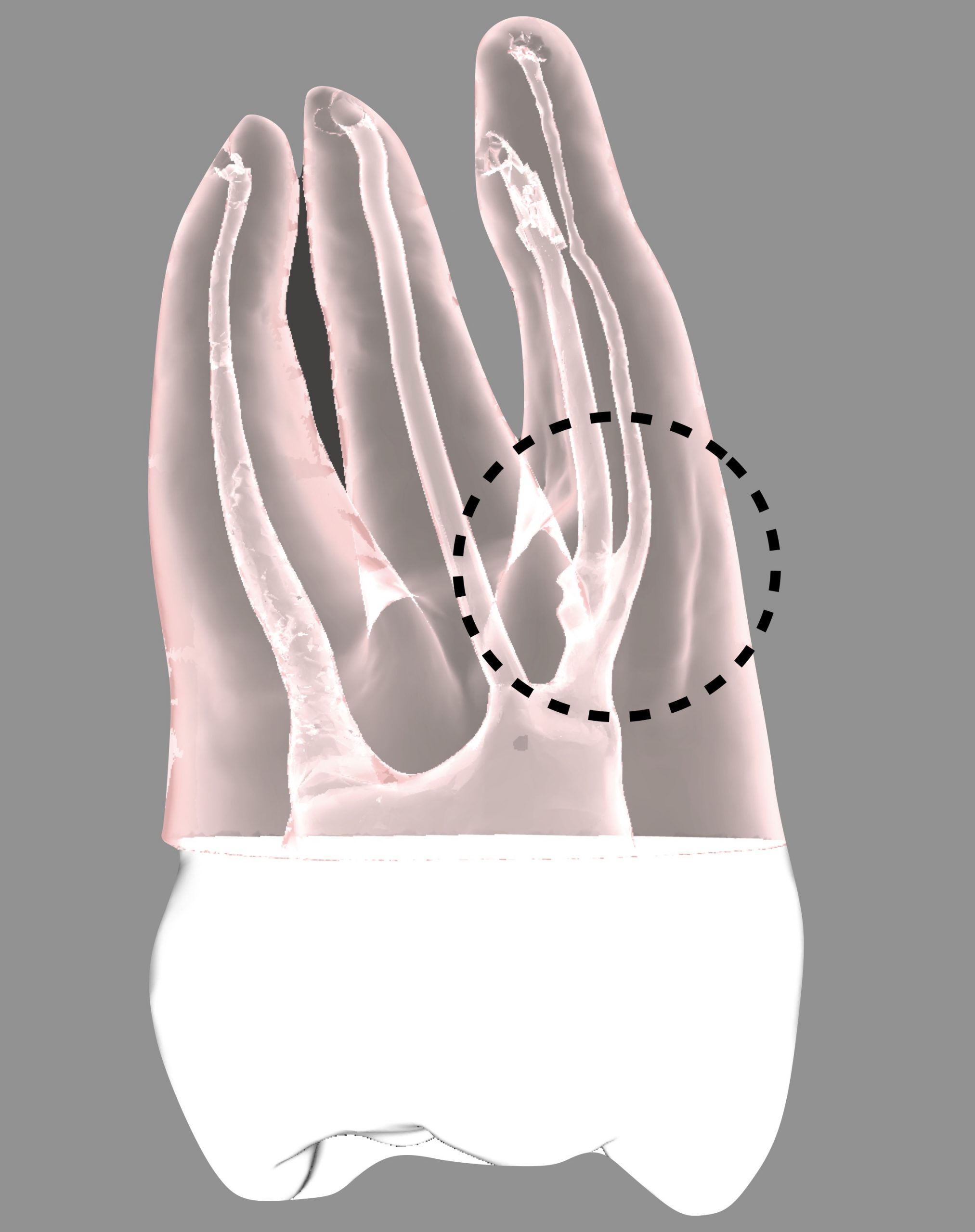
Fig. 2
Typical example of coronal curvatures in thin canals.
The mesial canal has been shaped until 26/.04, but Navitip can reach only half of the root.
On the other hand, IrriFlex is able to reach the apical area, making a perfect liquid exchange.
A 30G metal needle remains 8mm shorter than the WL, while IrriFlex is almost able to reach the WL, remaining 2mm short.

Fig. 3
X-rays of the case shown in the video.
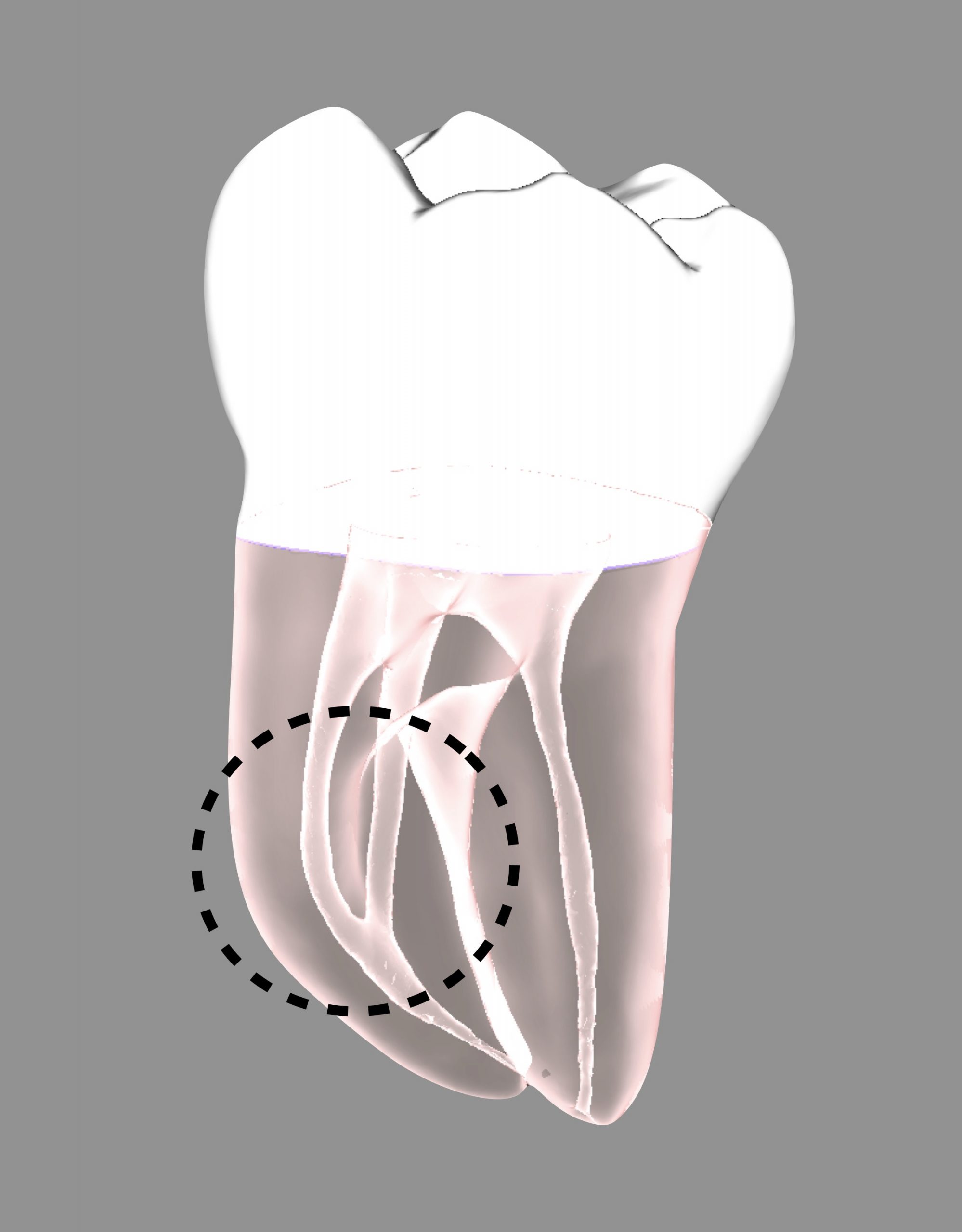
Fig. 4
Coronal curvature in MB root.
The anatomy of this model was obtained by taking a MICRO CT of a tooth. The mesial root shows a curvature at the middle of the root.
The mesial root has been shaped up to 25/.06, but Navitip is not able to move over the curvature. Conversely, IrriFlex can reach in a repeatable way the apical third
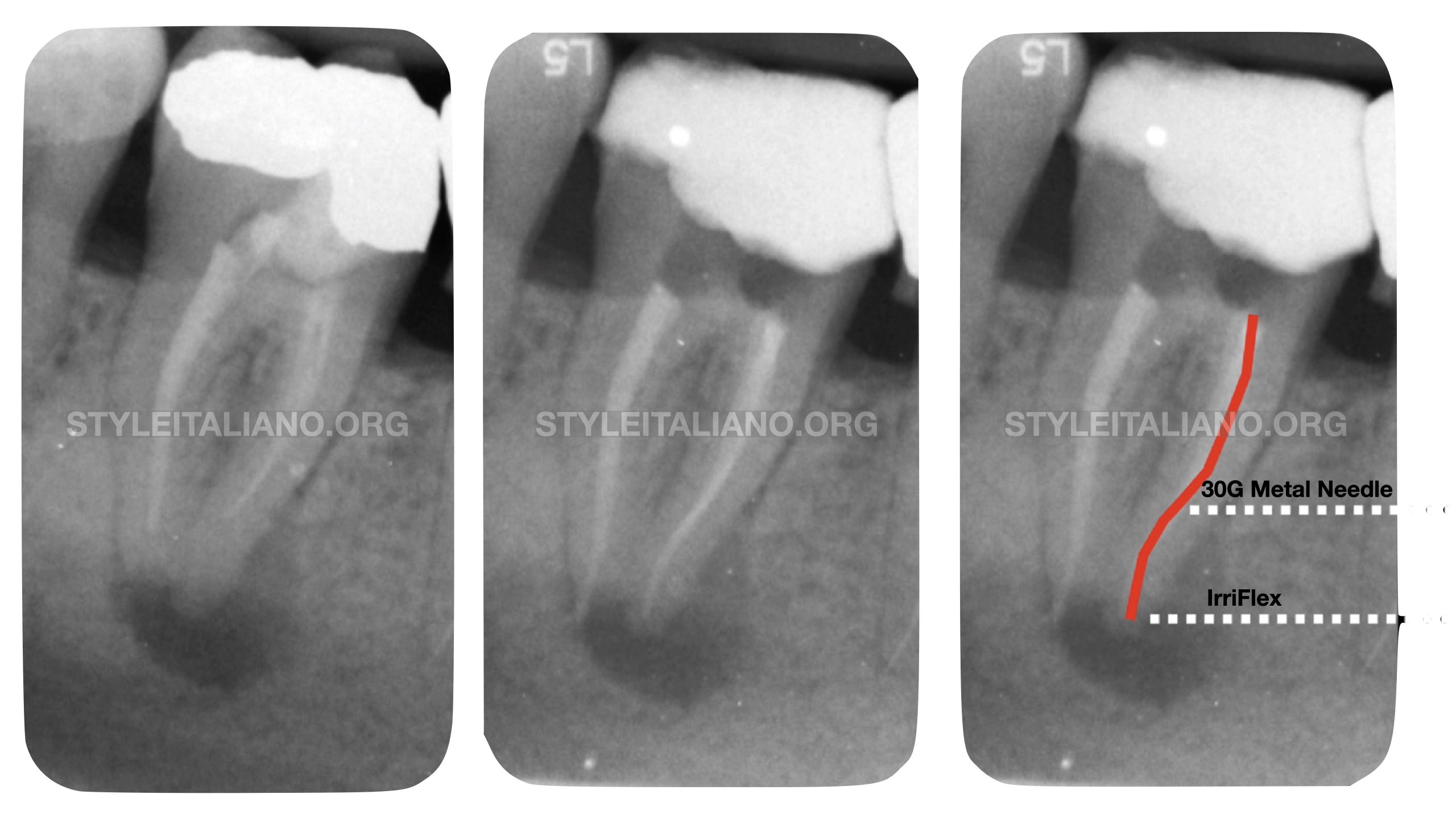
Fig. 5
Comparative penetration between a 30G metal needle and IrriFlex in a lower molar with middle root curvature.
Shaping 25/.06.
With IrriFlex it is always possible to reach the desired length, while with the metal needle the final position is really shorter than ideal penetration
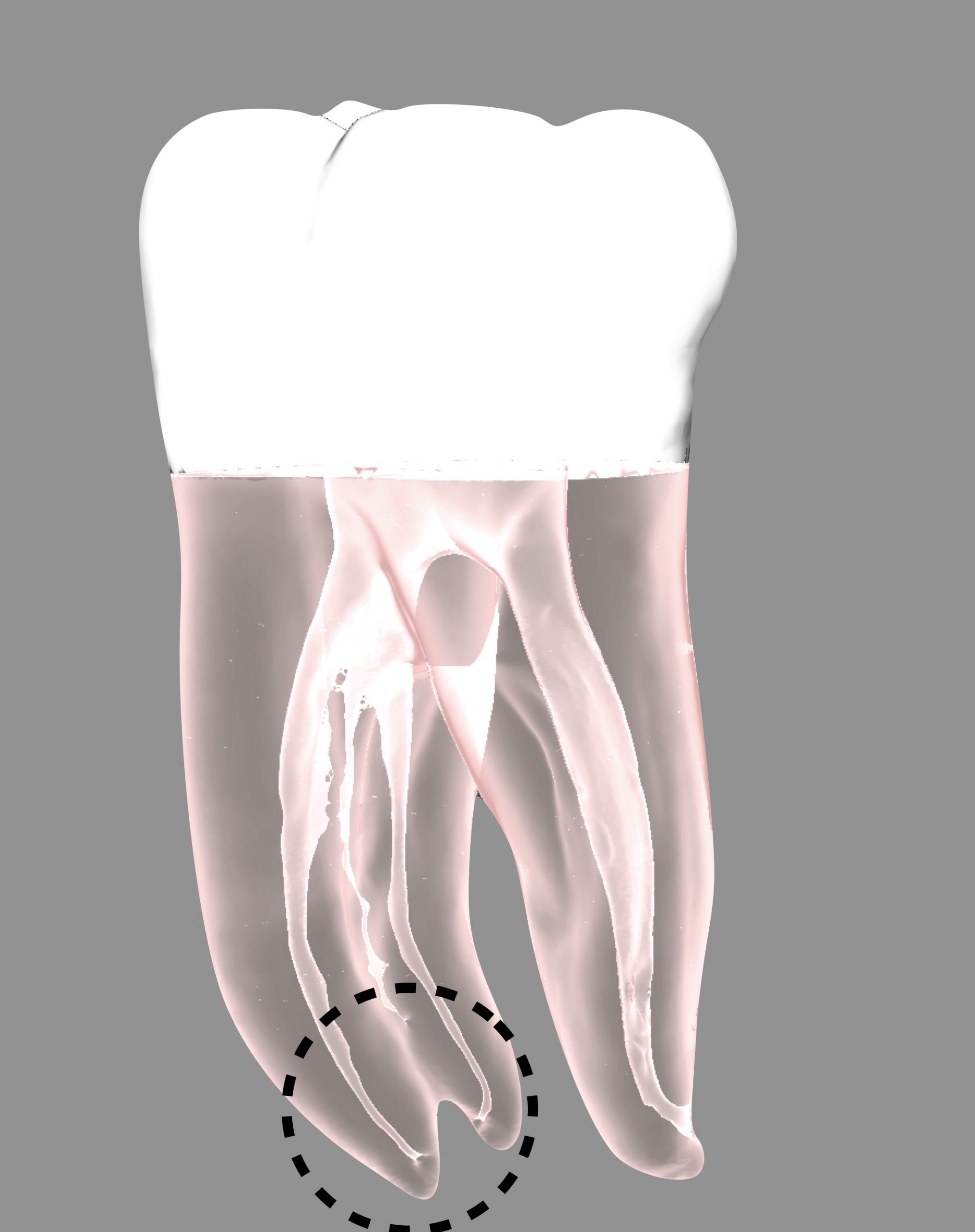
Fig. 6
Lower first molar with apical curvatures.
The mesial canals have been shaped up to 26/.04. The video shows how Navitip is blocked at the middle part of the root; on the contrary IrriFlex can move down and bypass also the apical curvature.

Fig. 7
Deep apical curvature in a lower molar. Shaping 20/.06.
3d recostruction
Clinical view of IrriFlex use

Fig. 8
A great challenge for cleaning could be represented also by a wide canal and a wide apex. Every needle can reach the ideal WL, but the risk is to extrude liquid beyond the apex and not remove in an afferent way the debris from the walls. IrriFlex is safe even in this case, and it is really effective for smear layer removal.
The clinical case has been managed with the Print&Try technique. An huge irregular apex has been sealed with MTA after a cleaning protocol. The video shows the power of the turbulence created by the safe extrusion of Hypochloryte from IrriFlex tip.
Conclusions
The use of the right needle represents a real revolution in the daily practice. The deep disinfection is the key for a repeatable success in Endodontics, but which is the ideal device?
IrriFlex is useful in all clinical scenarios and it has not limitations as curvatures and narrow canals. Its usability is evident also when we have to treat wide canals in a safe way.
Bibliography
Ahmad, M., Pitt Ford, T. J., & Crum, L. A. (1987). Ultrasonic debridement of root canals: acoustic streaming and its possible role. Journal of Endodontics, 13(10), 490–499. https://doi.org/10.1016/s0099-2399(87)80016-x
Azim, A. A., Aksel, H., Zhuang, T., Mashtare, T., Babu, J. P., & Huang, G. T.-J. (2016). Efficacy of 4 Irrigation Protocols in Killing Bacteria Colonized in Dentinal Tubules Examined by a Novel Confocal Laser Scanning Microscope Analysis. Journal of Endodontics, 42(6), 928–934. https://doi.org/10.1016/j.joen.2016.03.009
Ballal, N. V., Gandhi, P., Shenoy, P. A., & Dummer, P. M. H. (2020). Evaluation of various irrigation activation systems to eliminate bacteria from the root canal system: A randomized controlled single blinded trial. Journal of Dentistry, 99(June). https://doi.org/10.1016/j.jdent.2020.103412
Ballal, N. v., Gandhi, P., Shenoy, P. A., Shenoy Belle, V., Bhat, V., Rechenberg, D. K., & Zehnder, M. (2019). Safety assessment of an etidronate in a sodium hypochlorite solution: randomized double-blind trial. International Endodontic Journal, 52(9), 1274–1282. https://doi.org/10.1111/iej.13129
Bao, P., Shen, Y., Lin, J., & Haapasalo, M. (2017). In Vitro Efficacy of XP-endo Finisher with 2 Different Protocols on Biofilm Removal from Apical Root Canals. Journal of Endodontics, 43(2), 321–325. https://doi.org/10.1016/j.joen.2016.09.021
Basrani, B., Santos, J. M., Tjäderhane, L., Grad, H., Gorduysus, O., Huang, J., Lawrence, H. P., & Friedman, S. (2002). Substantive antimicrobial activity in chlorhexidine-treated human root dentin. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics, 94(2), 240–245. https://doi.org/10.1067/moe.2002.124002
Baugh, D., & Wallace, J. (2005). The role of apical instrumentation in root canal treatment: a review of the literature. Journal of Endodontics, 31(5), 333–340. https://doi.org/10.1097/01.don.0000145422.94578.e6
Baumgartner, J. C., & Cuenin, P. R. (1992). Efficacy of several concentrations of sodium hypochlorite for root canal irrigation. Journal of Endodontics, 18(12), 605–612. https://doi.org/10.1016/S0099-2399(06)81331-2
