Radix Entomolaris: Case Report with Clinical Implication
12/01/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
An awareness and comprehensive knowledge of the unusual root canal morphology can contribute to the success of the endodontic procedure. The majority of the mandibular first molars have one mesial and one distal root with two mesial canals and one distal canal. Carabelli was the first one to mention the presence of an additional root in mandibular first molar and called it as radix entomolaris (RE). This additional third root is commonly found distolingual. When the extra root
is present on the mesiobuccal side, it is called as radix paramolaris. Literature suggests the presence of RE in less than 5% population in white Caucasian, African, Eurasian and Indians whereas it is present with a frequency of 5–30% in races with Mongoloid traits such as the Chinese, Eskimos, and Native Americans. This article highlights the clinical approach for identification and modifications in endodontic management of mandibular first molar with RE.

Fig. 1
CASE 1
A 12-year-old female came with a chief complaint of severe pain in the left lower back tooth region since last two days. The pain aggravated on taking hot food and beverages, and lasted for 2–3 hours. On clinical examination, the mandibular left first molar was deeply carious and was diagnosed with irreversible pulpitis. The radiograph of the mandibular right first molar was normal without any periapical changes.
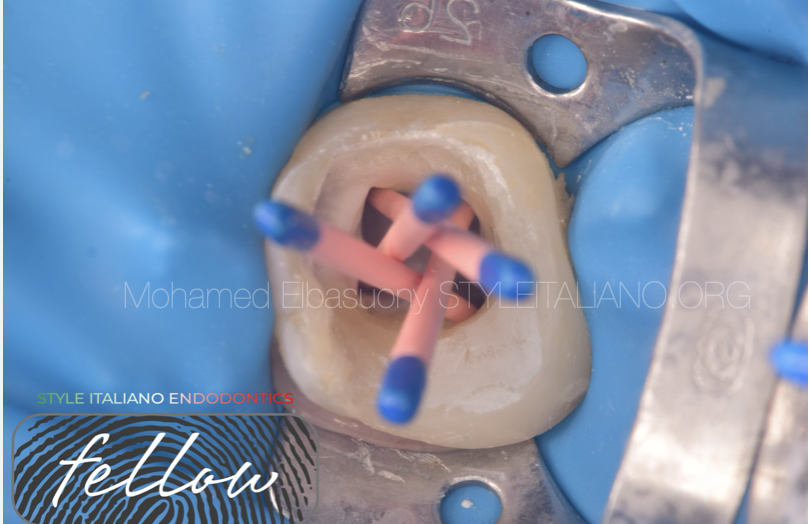
Fig. 2
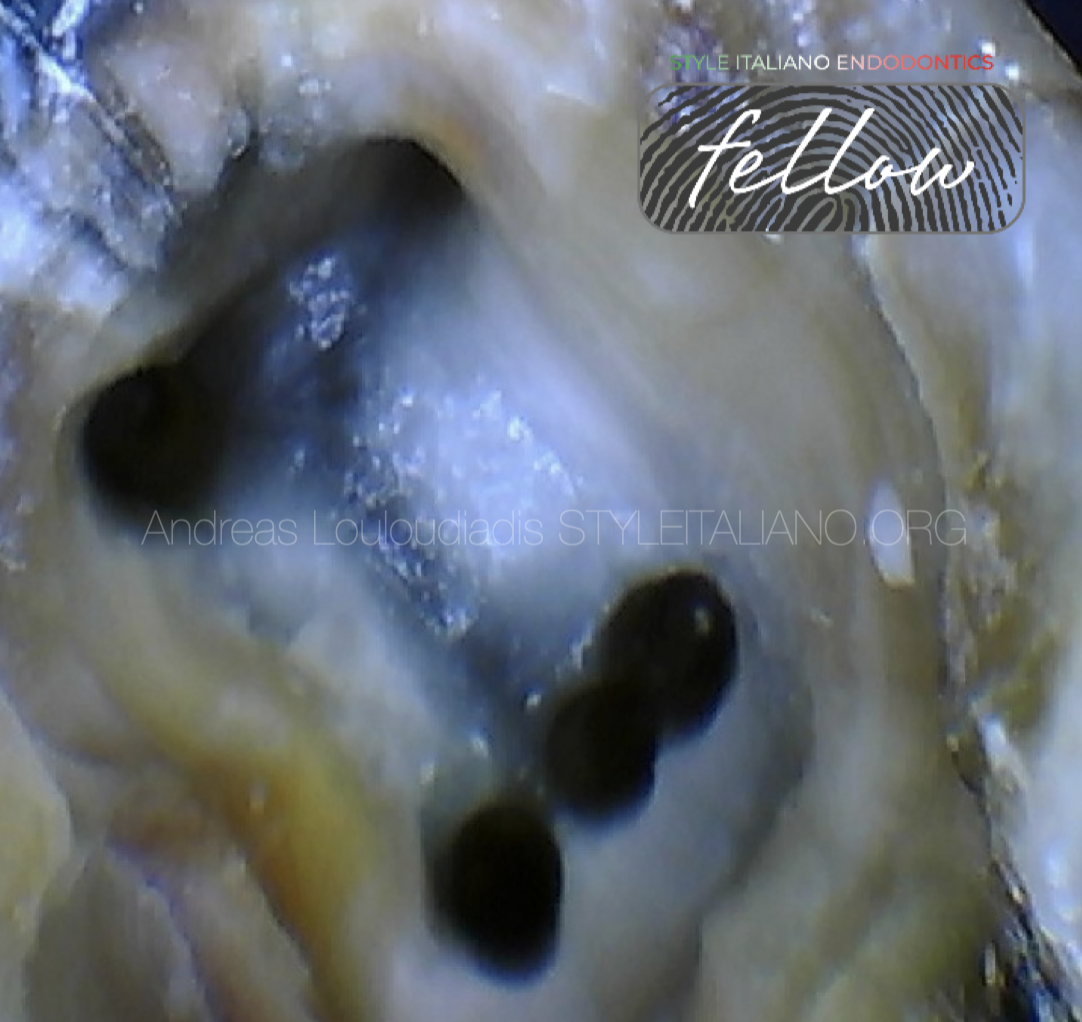
Access cavity preparation was done after rubber dam isolation and under local anesthesia with an endo access bur.pre-endo build up was done. The first distal canal was located towards the buccal side indicating the presence of one additional canal on the lingual side. The shape of the access cavity was modified from triangular to a trapezoidal form to search for the additional canal orifice. DG-16 endodontic explorer was used to locate the root canal orifices and 15 # K-file was used to establish patency of the canals. Working length was determined using apex locator. The canals were cleaned with 2.5% sodium hypochlorite followed by saline and 17% EDTA was used as final flush.
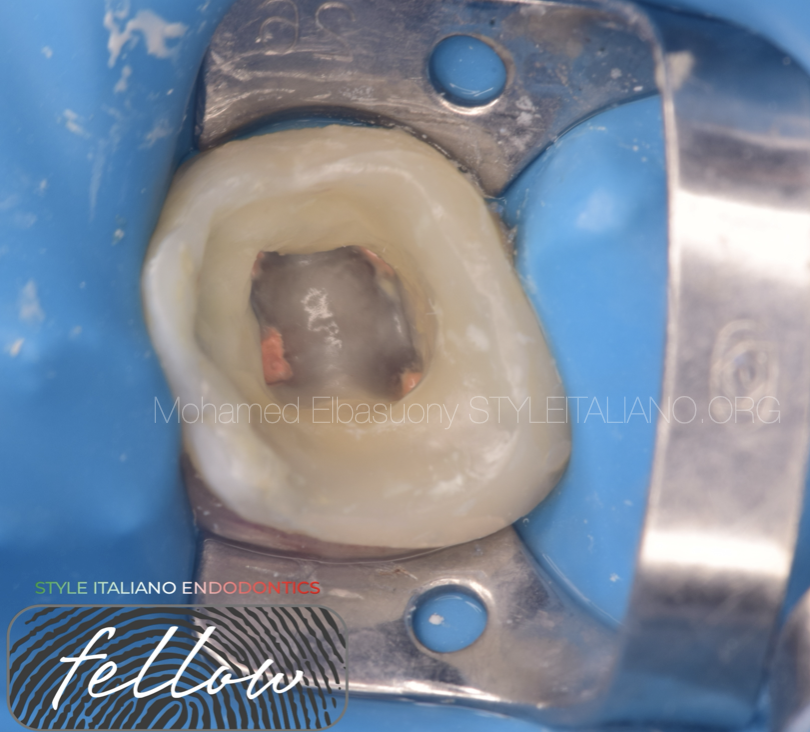
Fig. 3
Obturation was performed with gutta-percha points after application of bioceramic root canal sealer.

Fig. 4
Restoration was done with composite resin and a post-obturation radiograph was taken.

Fig. 5
Radiographic workflow.

Fig. 6
CASE 2
A 38-year-old female patient came to my clinic with a history of pain in the lower right side in relation to lower right first molar. On clinical examination, right mandibular first molar was found to be restored with amalgam restoration. Radiographic interpretation revealed the presence of apical periodontitis and pulpotomy. Local anesthesia was administered and rubber dam was applicated.
The old restoration was removed with round bur in combination with ultrasonics in the pulp chamber. The canal orifices were negotiated with DG-16 explorer. The fourth canal was negotiated after slight ultrasonic widening of the distal orifice in respect of low of color.

Fig. 7
Access cavity and four distinct canal orifices.
Sodium hypochlorite was used for disinfection of the root canal system.

Fig. 8
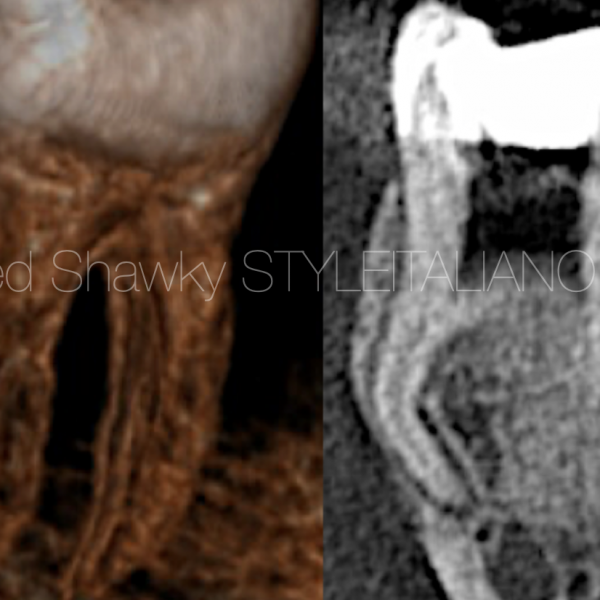
After location and enlargement of the orifice of the RE, initial root canal exploration with small files (size 10 or less) together with radiographical root canal length and curvature determination, and the creation of a glide path before preparation, is step-by-step actions that was taken to avoid procedural errors.
Ultrasonic tips were used to remove the isthmus between the distal canals.

Fig. 9
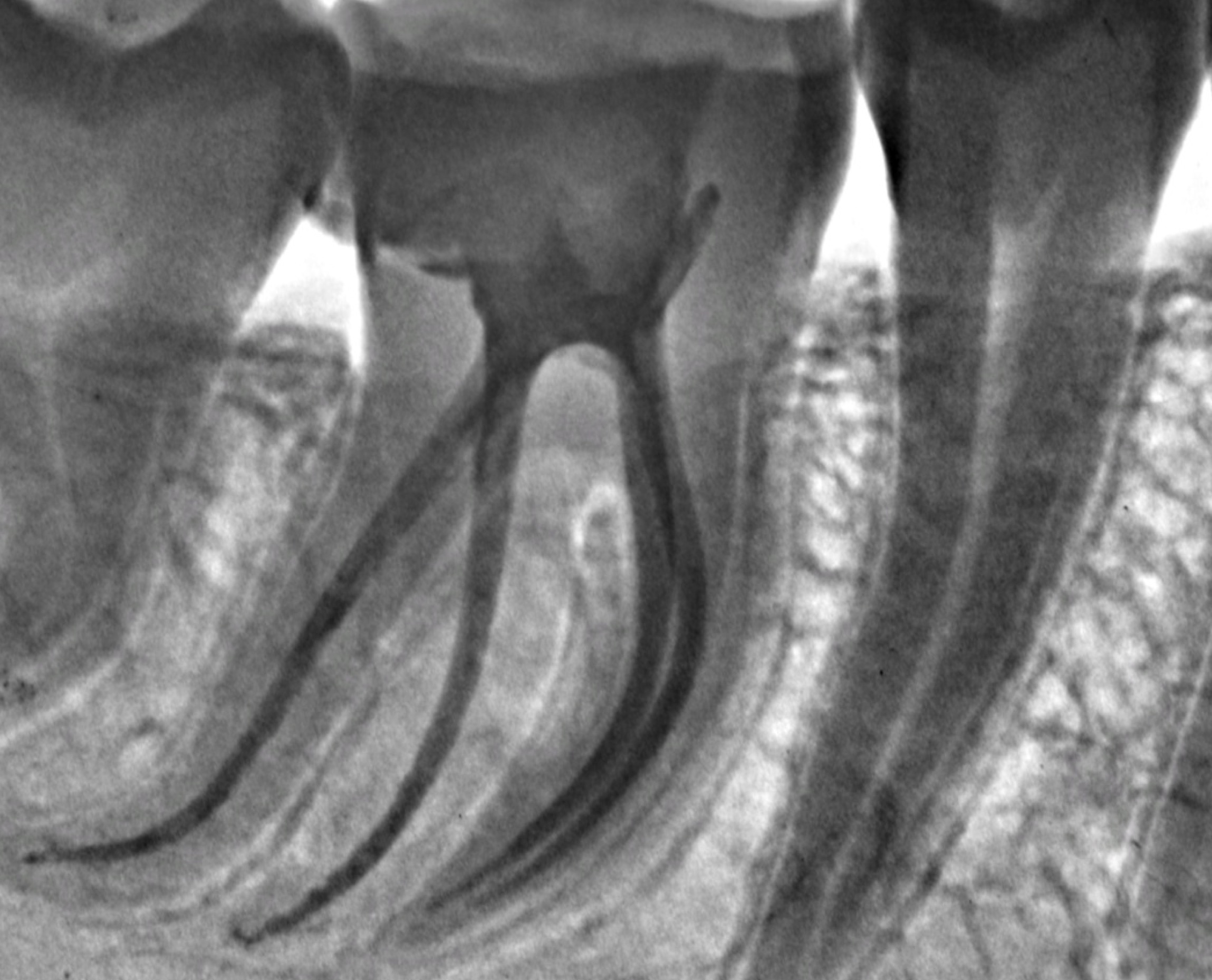
The gutta cone fit, with radiographical exposure, confirmed the presence of an RE.

Fig. 10
All canals were filled with gutta-percha and bioceramic root canal sealer.
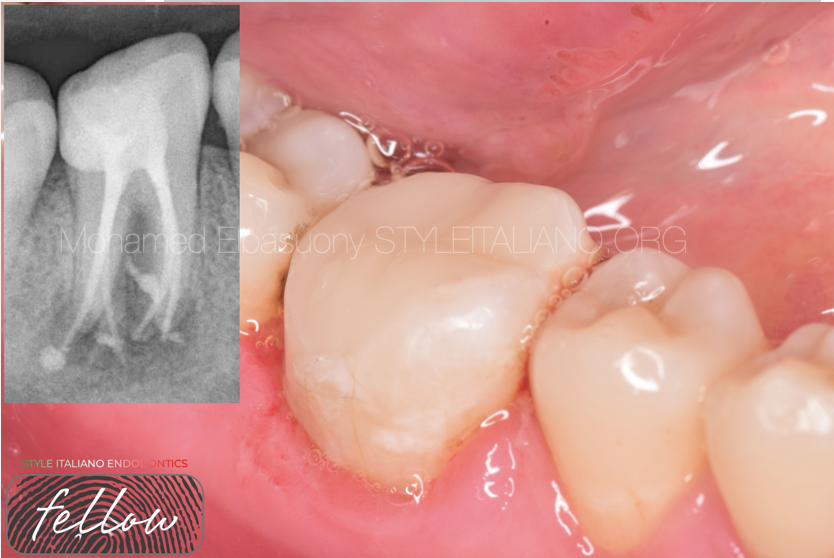
Fig. 11
Restoration was done with composite resin and a post-obturation radiograph was taken.
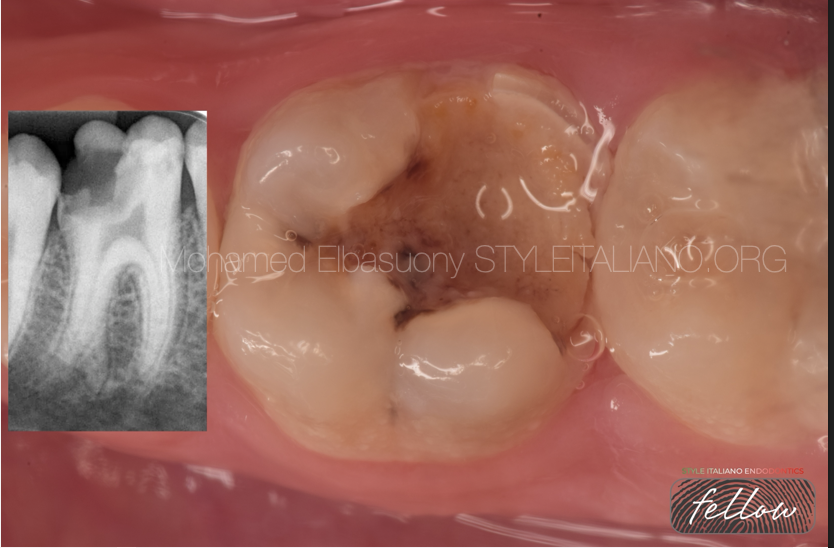
Fig. 12
CASE 3
A 10-year-old female came for endodontic treatment of mandibular right first molar with a chief complaint of severe pain. On clinical examination, The tooth was sensitive to percussion and extensive tooth decay had caused fracture of the distal part of the crown. Radiographically, no signs of periapical pathosis were observed. Local anesthesia was administered and rubber dam was applicated.
The caries lesion was removed with round bur and the missing part of the tooth was restored with composite restoration. The canal orifices were negotiated with DG-16 explorer. The access cavity was enlarged and another root canal orifice was found
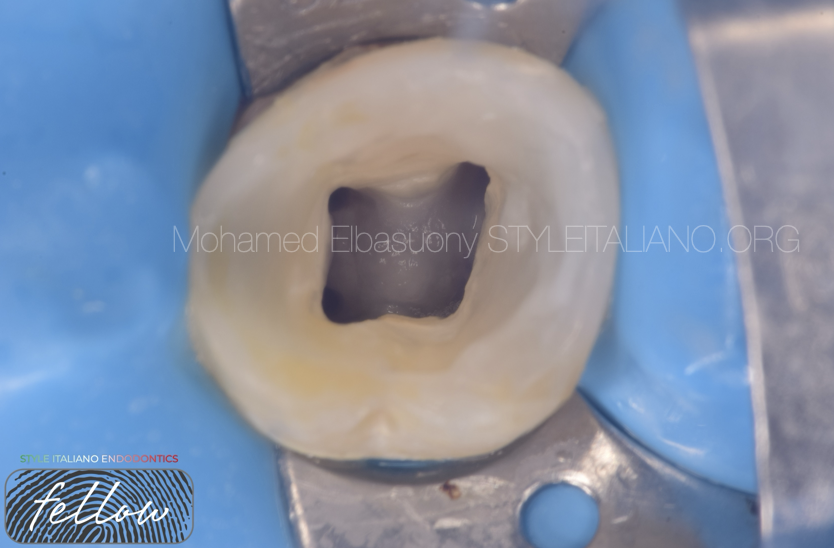
Fig. 13
The first distal canal was located towards the buccal side indicating the presence of one additional canal on the lingual side.

Fig. 14
Irrigation and sonic activation was performed.

Fig. 15
Master cone radiograph was taken, canals were dried with absorbent paper points.

Fig. 16
Obturation was performed with gutta-percha points in combination with bioceramic root canal sealer.

Fig. 17
Composite resin was used for coronal restoration, and a post-obturation radiograph was obtained.

Fig. 18
About the author:
Mohamed Elbasuony
BDS from faculty of dentistry, Mansoura university in 2013.
Diploma in Endodontics at faculty of dentistry, Mansoura university in 2018.
Enrolled in the MSc in Endodontics at faculty of dentistry, Mansoura university in 2020.
StyleItaliano Endodontics Fellow
Endodontic Specialist.
Conclusions
Conclusion
An accurate diagnosis, adequate chemomechanical preparation, and three-dimensional obturation determine the success of root canal therapy. As the orifice of RE is distolingually located, the shape of access cavity should be modified from classical triangular form to trapezoidal or rectangular form to better locate the orifice of distolingual root. Care must be taken to avoid excessive removal of dentin or gauging during access cavity preparation, as this may weaken the tooth structure. Proper interpretation of radiographs taken at different horizontal angulations may help to identify a number of roots and their morphology.
Bibliography
- Carlsen, O. L. E., & Alexandersen, V. (1990). Radix entomolaris: identification and morphology. European Journal of Oral Sciences, 98(5), 363-373.
- De Moor, R. J. G., Deroose, C. A. J. G., & Calberson, F. L. G. (2004). The radix entomolaris in mandibular first molars: an endodontic challenge. International endodontic journal, 37(11), 789-799.