Radix entomolaris- a case series
11/07/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Endodontic treatment entails thorough chemo-mechanical debridement and disinfection of the pulp spaces, followed by placement of an inert biocompatible material to allow hermetic sealing of the root canal system. Inability to meet either of these objectives can inadvertently lead to endodontic failure. Concomitantly, an awareness of normal and aberrant root canal morphology is a key contributing factor for successful endodontic outcome.
Majority of mandibular molars have 2 roots (mesial and distal) with 3-4 corresponding canals. One of the major variants in mandibular molars is the presence of an additional third root (radix molaris RM), present either disto-lingually called radix entomolaris (RE) or mesio-buccally called radix paramolaris (RP). Radix entomolaris (RE) was first reported in literature by Carabelli (1844) and the term was coined by Bolk in 1915. (1) These additional roots when present, maybe partially fused or separate, and are usually smaller and more curved than the other roots. (2)
This case series highlights the prevelance, classification and clinical considerations of treatment of mandibular molars with RE.

Fig. 1
The incidence and prevalence of RE varies in different ethnic groups.
RE is known to be a dominant genetic trait in pure Eskimo and Eskimo/Caucasian mixes and due to its high incidence in these populations, the RE is considered to be a normal morphological variant
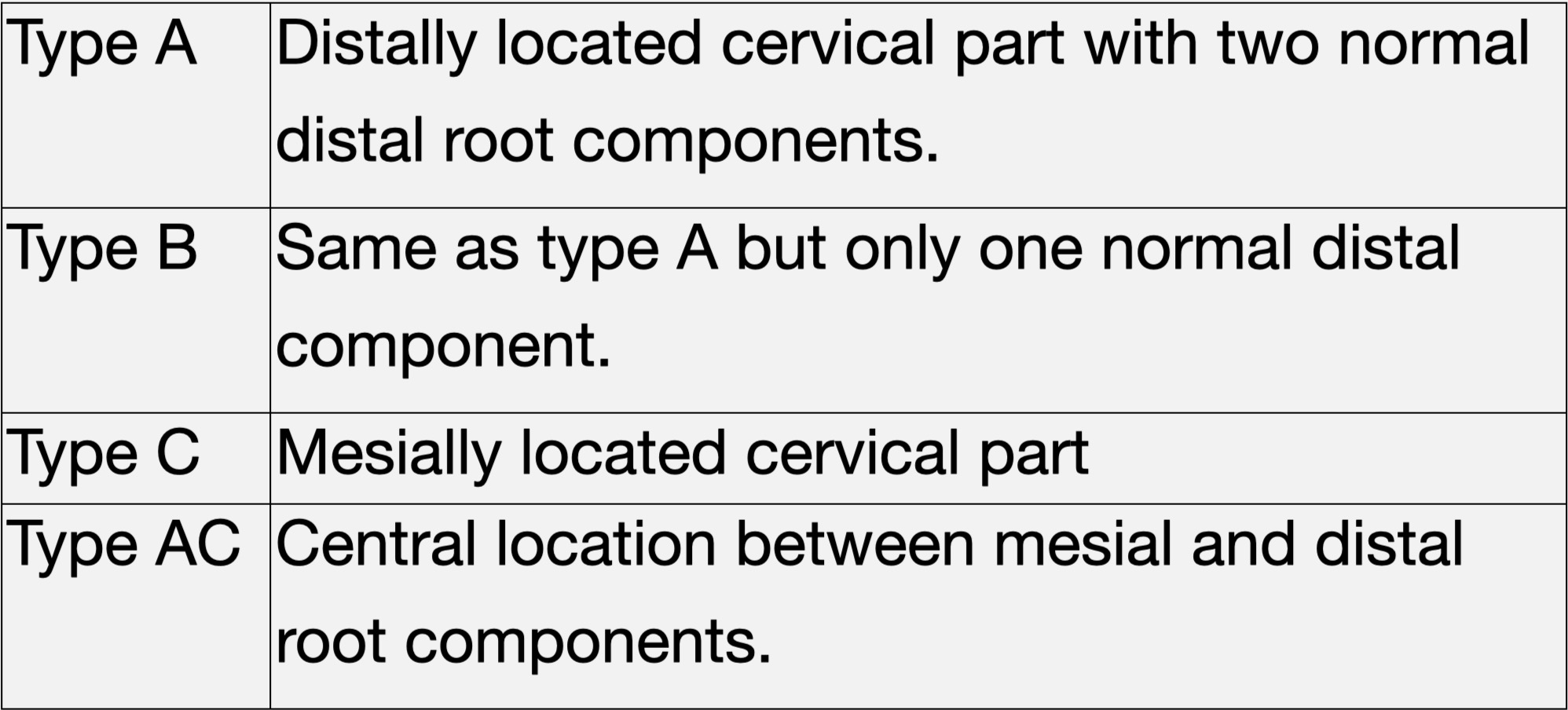
Fig. 2
Carlsen and Alexanderson classification based on the location of the cervical part of the RE: (4)
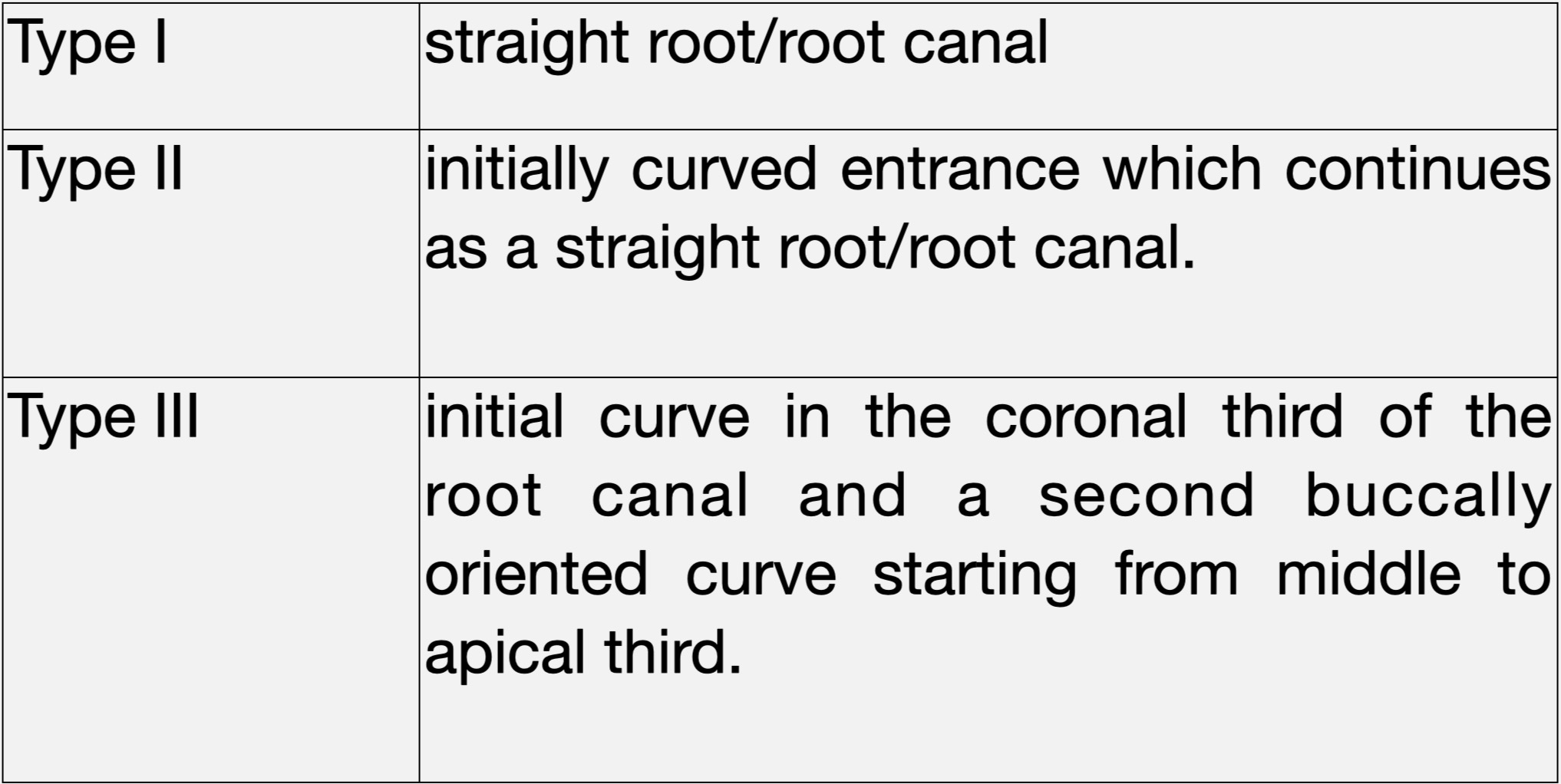
Fig. 3
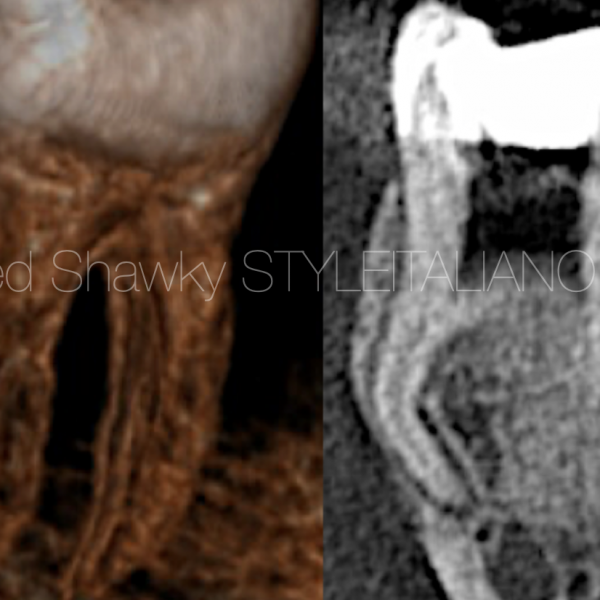
De Moor et al. classification based on the curvature in buccolingual orientation. (5)
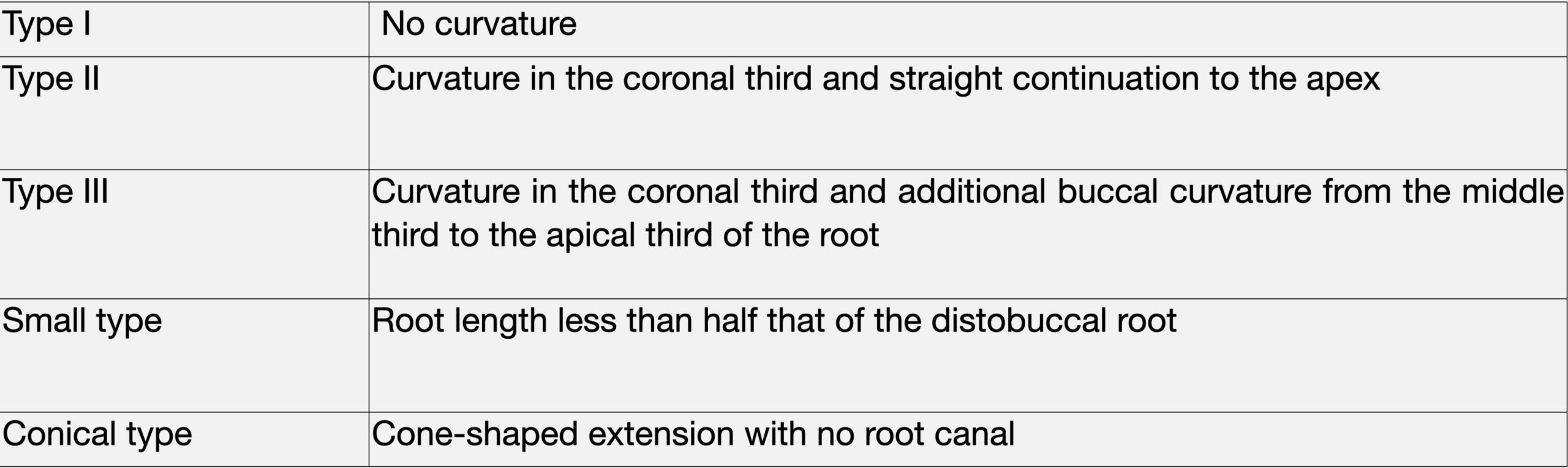
Fig. 4
Song et al. 2010 classification based on morphologic features in general Korean population. (6)
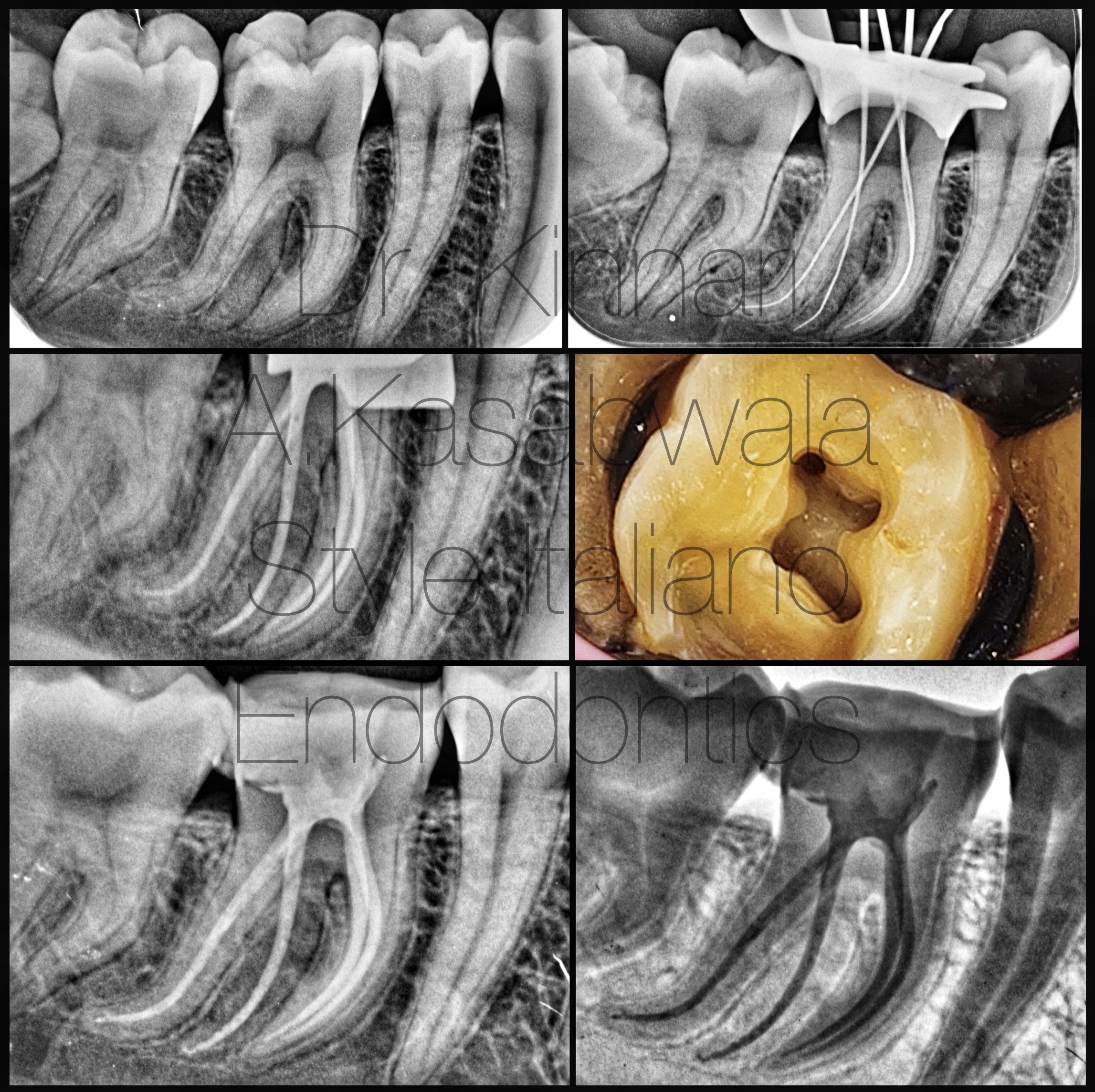
Fig. 5
23 year old female patient reported with complain of spontaneous, nocturnal pain and pain on biting in tooth 46.
Diagnosis (after pulp sensibility testing): symptomatic irreversible pulpitis with symptomatic apical periodontitis.
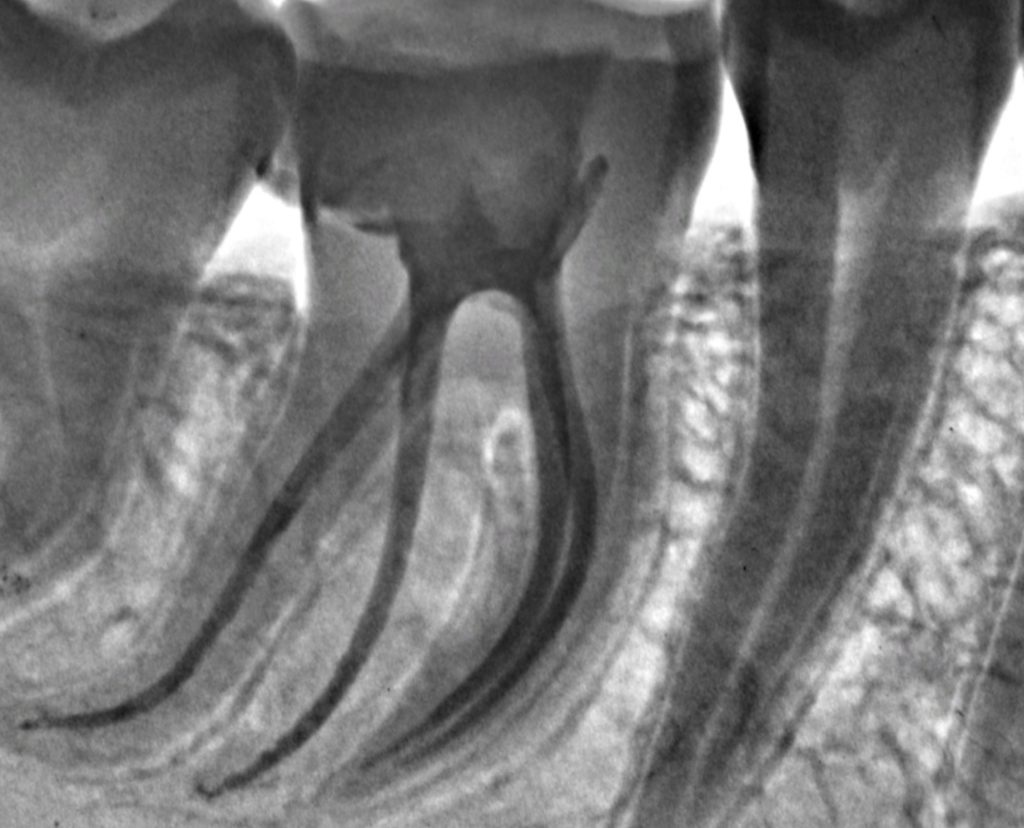
Angled pre-operative radiograph revealed RE.
Access opening was extended disto-lingually to reveal the orifice of RE.
4 canals present – MB, ML, DB, DL/RE.
Initial canal negotiation was done with no. 6 K file (Mani) till resistance, with gentle watch winding motion, followed by filing till working length with No.6,8, 10 K files.
Glide path was established by Path files (Dentsply Mallifer) and One G file (Micro Mega).
Canals were shaped with 4% Hero Gold files (Micro Mega). Restricted shaping with less tapered files was considered given the acute curvature of the canals.
Irrigation was done with 5.25% NaOCl intermittently and as final rinse alternated with 17% EDTA.
Obturation was done using single cone technique with 4% GP cones and AH plus sealer.
Case was done using Labomed Prima microscope.
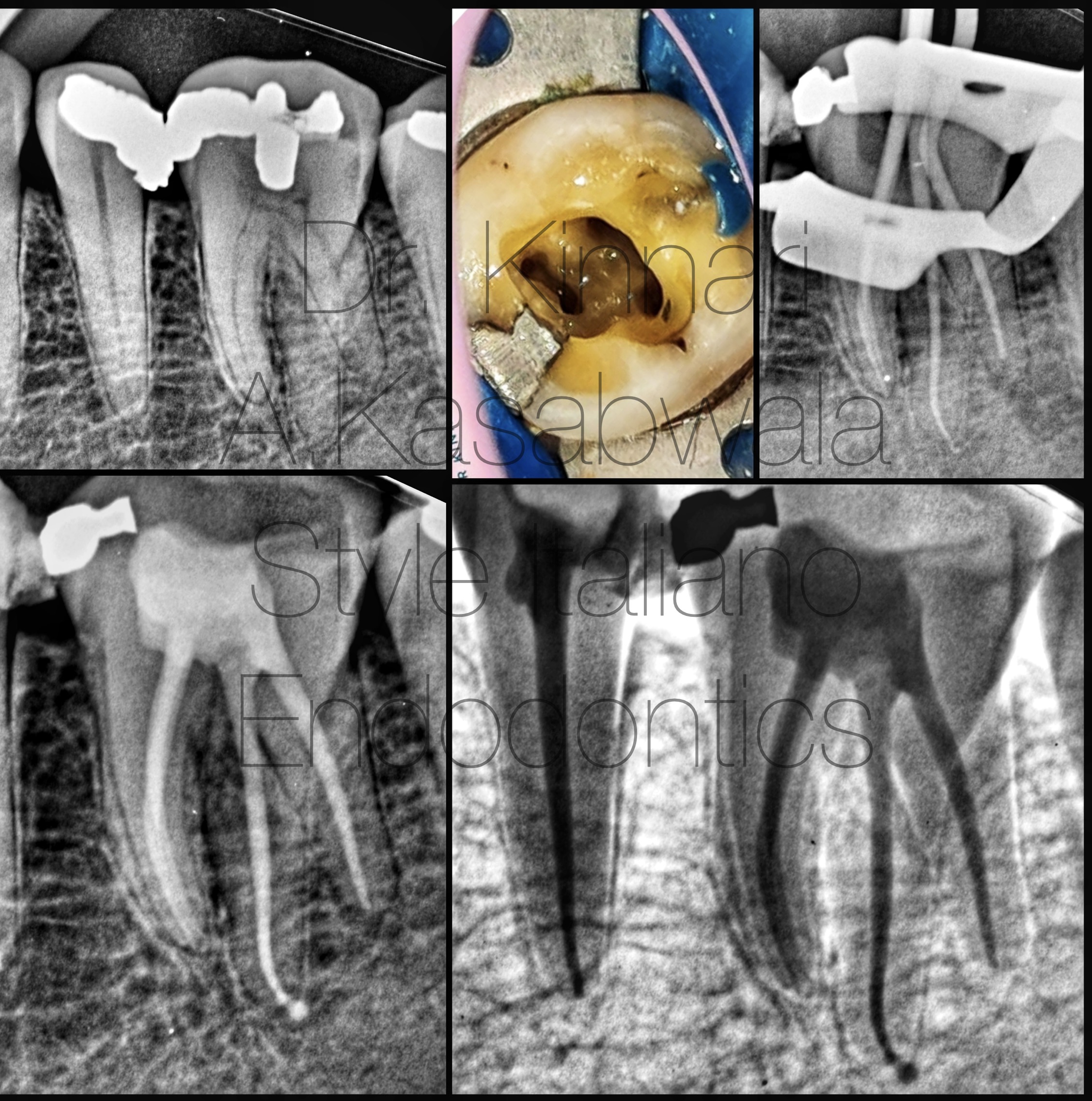
Fig. 6
54 year old female patient reported with throbbing pain and pain on percussion under deep amalgam restorations in teeth 35, 36.
Diagnosis (after pulp sensibility testing): pulp necrosis in 35, 36.
Angled pre-operative radiograph revealed RE in 36.
Access opening was extended in disto-lingual direction to reveal RE.
4 canals present – MB, ML, DB, DL/RE.
Pulp stone was removed with ultrasonic tips and calcified mesial canals were initially negotiated with 6,8,10 K files progressively till WL.
Glide path was established using One G file (Micro Mega).
Canals were shaped with 4% Hero Gold files (Micro Mega). Irrigation was done with 5.25% NaOCl intermittently and as final rinse alternated with 17% EDTA.
Obturation was done with single cone technique using 4% GP cones and Ceraseal bioceramic sealer (Meta Biomed).
Case was done using Labomed Prima microscope.
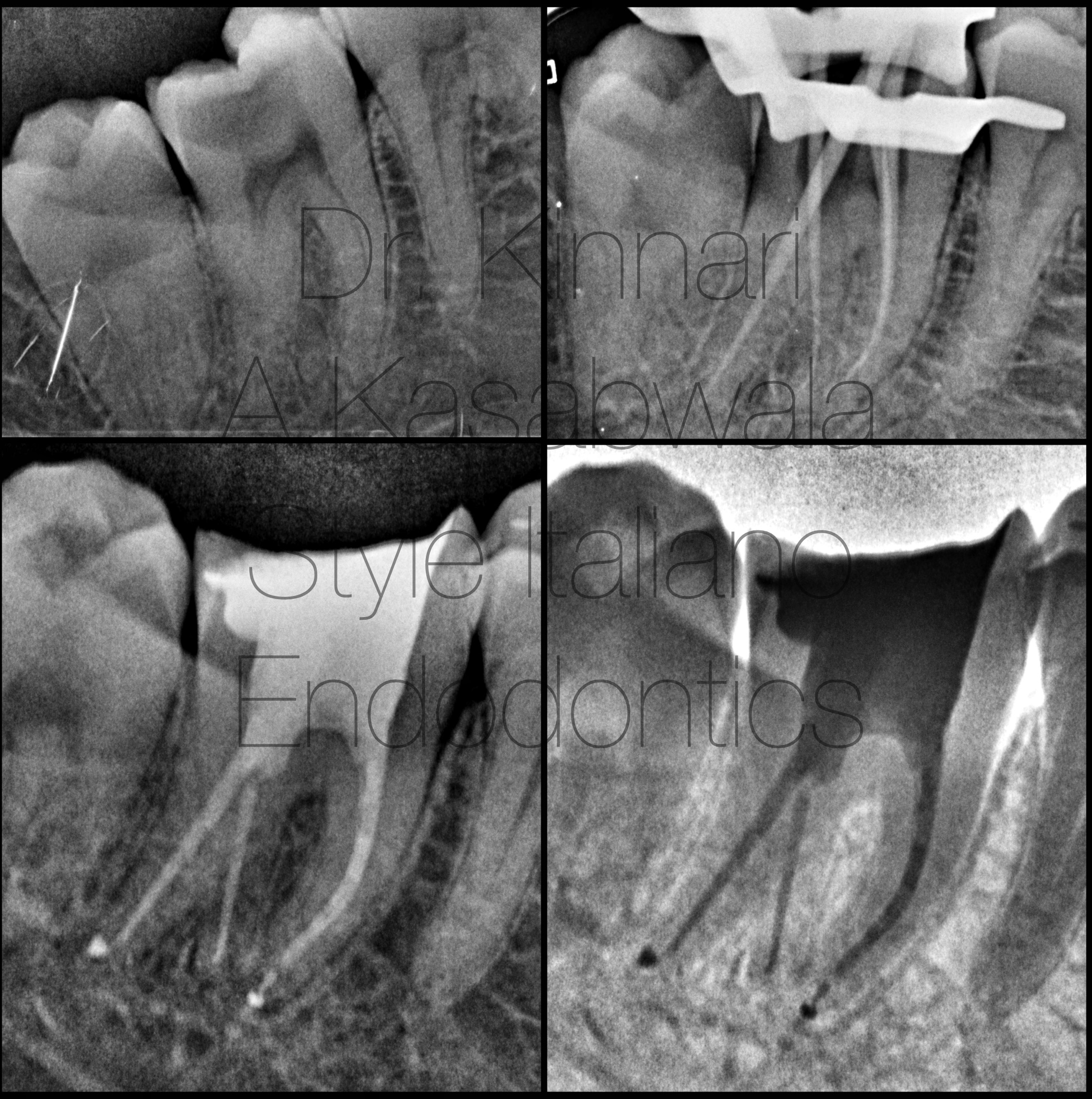
Fig. 7
28 year old female patient reported with spontaneous, nocturnal pain and pain on biting in tooth 47.
Diagnosis (after pulp sensibility testing): symptomatic irreversible pulpitis.
Angled pre-operative radiograph revealed RE.
4 canals present – MB, ML, DB, DL/RE.
Canals were negotiated with 8,10 K files progressively till WL. Canals were shaped with 4% Hero Gold files (Micro Mega). Irrigation was done with 5.25% NaOCl intermittently and as final rinse alternated with 17% EDTA.
Obturation was done using single cone technique using 4% GP cones and Ceraseal bioceramic sealer (Meta Biomed).
Case was done using Labomed Prima microscope.
Existence of three rooted mandibular molars is a rarity. According to Manning, only 2% of mandibular second molars showed three roots.(7)
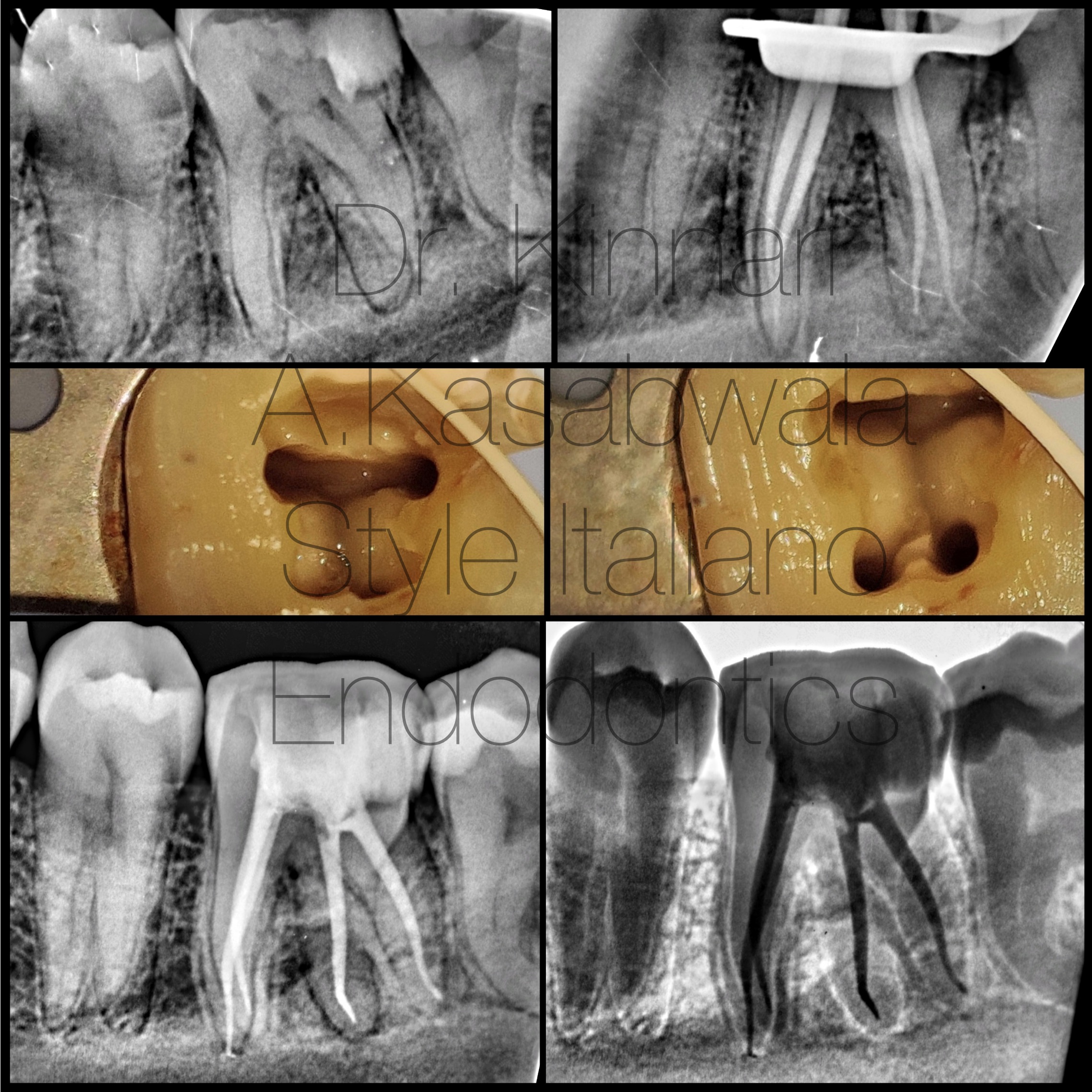
Fig. 8
25 year old female patient reported with intermittent pain due to secondary decay under composite restoration.
Diagnosis (after pulp sensibility testing): symptomatic irreversible pulpitis.
Angled pre-operative radiograph revealed 4 distinct root outlines suggestive of RE and RP.
Clinically access opening needed to be extended distolingually to reveal RE.
4 canals located– MB/RP, ML, DB, DL/RE with independent portals of exit.
Shaping was done with 6% Hero Gold files (Micro Mega).
Irrigation was done with 5.25% NaOCl intermittently and as final rinse alternated with 17% EDTA.
Obturation was done with single cone technique using 6% GP cones and Ceraseal bioceramic sealer (Meta Biomed).
Case was done using Labomed Prima microscope.
The incidence of four-root configuration is only 0.04% in the mandibular first molars. (8)
 : eval()'d code</b> on line <b>11</b><br />
)
Fig. 9
Endodontic failure would be inevitable if extra roots haven’t been accurately diagnosed and treated. Overlapping or unclear root outlines in a straight pre-operative radiograph can hint towards the presence of RM since RE and RP lie in the same bucco-lingual plane as their respective distal and mesial counter-parts, respectively. An angulated radiograph at 30 degrees can separate these overlapping root outlines and can reveal the extra root following buccal object rule or Clark’s rule, the same lingual, opposite buccal (SLOB rule). (9) CBCT aids in visualising 3-dimensional root canal anatomy and thus would provide an exact spatial orientation of the orifice and root canal.
Clinically, complete de-roofing of the pulp chamber, extension of the conventional triangular access to a more rectangular or trapezoidal outline form to gain straight line access and examination of the floor of the pulp chamber to assess the dentinal map are primary requisites in locating RE orifice. The radix roots being short and more curved, their canals should be instrumented with lesser taper files under caution to prevent iatrogenic complications. (3)
Magnification devices such as dental operating microscope and loupes become indispensable in allowing the clinician to operate seamlessly in cases with such abnormal morphology.
Conclusions
Identification of aberrant root canals systems becomes quintessential in clinical practice to avoid endodontic treatment failure.
Awareness and understanding of the anatomy, precisely angled pre-operative x-rays, magnification devices and additional investigations like CBCT can contribute to successful outcome of root canal treatment.
Negotiation of RE canals should be restricted to minimum tapers given their acute curvature and small size, in an attempt to avoid procedural errors.
Bibliography
- Carabelli G (1844) SystematischesHandbuch der Zahnheilkunde (2 edn). Braumuller und Seidel, Vienna, Italy. P114
- Gu Y, Zhou P, Ding Y, Wang P, Ni I (2011) Root canal morphology of permanent three-root mandibular first molars: Part III- An odontometric analysis. J Endod 37: 485-490.
- Calberson FL, De Moor RJ, Deroose CA. The radix entomolaris and paramolaris: clinical approach in endodontics. J Endod 2007; 33(1):58-63.
- Carlsen, O., & Alexandersen, V. (1990). Radix entomolaris: identification and morphology. Scandinavian journal of dental research, 98(5), 363–373.
- De Moor RJ, Deroose CA, Calberson FL. The radix entomolaris in mandibular first molars: an endodontic challenge. Int Endod J 2004
- Song JS, Choi HJ, Jung IY, Jung HS, Kim SO (2010) The prevalence and morphologic classification of distolingual roots in the mandibular molars in a Korean population. Journal of Endodontics 36, 653-7
- Manning SA. Root canal anatomy of mandibular second molars. Part I. Int Endod J. 1990
- Morita M. (1990). Shika gakuho. Dental science reports, 90(6), 837–854.
- Ingle JI, Heithersay GS, Hartwell GR et al. (2002) Endodontic diagnostic procedures. In: Ingle JI,Bakland LF, eds. Endodontics, 5th edn. Hamilton, London, UK: BC Decker Inc., 203–58.