

External cervical resorption
15/09/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
External cervical resorption (ECR) is an aggressive form of root resorption (RR), which initiates from the external cervical area of the tooth. Its aetiology is mostly unclear. As in this case, the lesion often progresses asymptomatically, until it is discovered incidentally.

Fig. 1
In 1999, Heithersay devised a classification of such lesions.
The prognosis of class 1 and 2 is good, whereas class 3 and 4 present with poor prognosis, often requiring extraction. This case depicts the management of a class 4 lesion.

Fig. 2
Patient, female, in her 40’s, presented with mild discomfort from her UR1. Clinical examination revealed that the UR1 was nonresponsive to cold and mildly tender to percussion.
Radiographic examination revealed that the UR1 suffers from ECR grade 4 Heithersay.
The guarded prognosis of the tooth was explained to the patient, who was keen to save the tooth, at all costs.
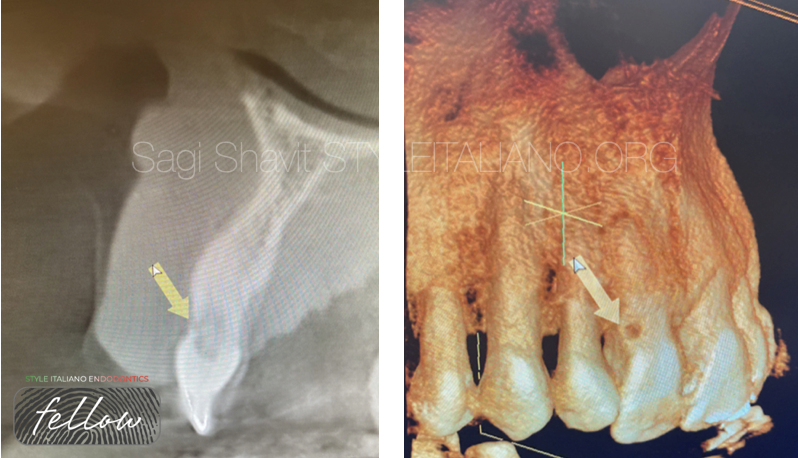
Fig. 3
A CBCT scan was acquired, which shows the favourable position of the initial lesion (disto buccal aspect of the tooth).
The treatment plan was to provide surgical repair of the lesion, followed by non-surgical endodontic treatment.

Fig. 4
After adequate anaesthesia (2% lidocaine with 1:80,000 adrenaline) a minimal flap was raised. The resorptive lesion was located and cleaned using high speed diamond bur, under copious irrigation.

Fig. 5
Rubber dam was placed in order to achieve good isolation.

Fig. 6
The lesion was sealed using composite, after which the flap was sutured using 4-0 non resorbable sutures.

Fig. 7
Non-surgical endodontic treatment was then performed, using copious sodium hypochlorite 5.25% in order to dissolve the granunation tissue,coupled with passive sonic activation (Eddy).
The rubber dam was secured with Wedgets, to prevent further trauma to the marginal gingivae.
Following the chemo-mechanical debridement, the endodontic space was obturated with Bioceramic putty, using the Shavit-Zemurg pellet former, and the access cavity was sealed with composite.
The patient returned 1 week later to remove her sutures, and she was asymptomatic.

Fig. 8
About the author:
Sagi Shavit
Visiting lecturer in Endodontics at Tipton Training. Endodontics module leader at City of London Dental School. Dentist with special interest in Endodontics at a Private Dental Practice, accepting referrals for complex endodontic treatments, including apicectomies.
Associate Dentist, accepting referrals for endodontic and implant treatments.
Clinical Skills:
I use dental operating microscope in 100% of my endodontic cases and magnifying loupes in restorative cases.
I use top of the range endodontic equipment such as apex locators, NiTi rotary files and system B obturation.
I perform micro surgical endodontic treatments with dental operating microscope.
I place and restore implants.
I am trained at delivering short term orthodontic treatment.
Conclusions
The management of ECR can be complex and may be unpredictable.
Correct diagnosis and treatment planning are essential for long term prognosis of such cases.
Bibliography
- Heithersay GS. Treatment of invasive cervical resorption: an analysis of results using topical application of trichloracetic acid, curettage, and restoration. Quintessence Int. 1999 Feb;30(2):96-110. PMID: 10356561.
- Sholeh Ghabraei, Behnam Bolhari, Nasim Hashemi, Hamidreza Gharehchahi, Conservative management of an advanced external cervical resorption with internal approach using bio‐ceramic materials: A case report, Clinical Case Reports, 10.1002/ccr3.8378, 12, 1, (2023).



