External resorption
14/10/2021
Fitim Shabani
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Tooth resorptions can be classified as: (1) trauma induced; (2) infection induced; or (3) hyperplastic invasive. Some transient trauma induced resorptions require no treatment but must be carefully monitored to check that there are no complicating issues such as infection. In cases of trauma induced replacement resorption, a multidisciplinary approach is usually necessary to ensure an optimal long-term solution. (GS Heithersay Management of tooth resorption ).
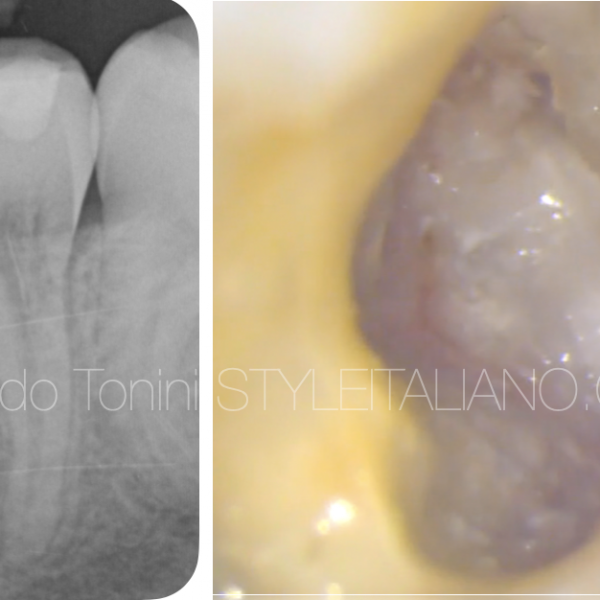
External resorptions present a difficult clinical situation: many times, lesions are misdiagnosed and confused with caries and internal resorptions. In this case we see clearly that the resorption is located in the distal/cervical part of the tooth.
In this case we first performed the DME (deep margin elevation), which was inevitable, to proceed further with the endodontic treatment and finally covered the tooth with an Overlay.

Fig. 1
Clinical case
Clinical data
In routine control the patient presents some slight complaints on the upper jaw right.
Xray shows an external resorbtion on the distal/cervical surface.
Vitality negative.
Treatment plan :
- DME / Deep Margin Elevation
- Endodontic treatment
- Prosthetic treatment

Fig. 2
Initial situation of the case.

Fig. 3
Deep margin elevation ( DME ) or coronal margin relocation, is performed.

Fig. 4
X-ray after DME deep marginal elevation
Mandatory step to continue with endodontic treatment.

Fig. 5
Determining the working length and at the same time controlling confluences in canals MB1 and MB2.

Fig. 6
Determining the working length and at the same time controlling confluences between MB1 and MB2.

Fig. 7
Endodontic treatment is performed.

Fig. 8
X-ray after obturation.

Fig. 9
Preparation for an Overlay.

Fig. 10
Occlusal view after cementation.

Fig. 11
Buccal view.

Fig. 12
Palatal view.

Fig. 13
Final X-ray.
Conclusions
Tooth resorption is a pathologic condition that still remains a mystery in many aspects. It may go unnoticed over many years as most cases of resorption are asymptomatic in nature. Early detection of resorption is essential for successful management.
The plan before treatment is of special importance, and almost in all cases a multi-disciplinary approach is needed.
Bibliography
Dr. Marina Fernandes, Ida de Ataide and Rahul Wagle,Tooth resorption part I - pathogenesis and case series of internal resorption, Case series Jan-Feb 2013.
Dr. Marina Fernandes, Ida de Ataide and Rahul Wagle,
Tooth resorbtion part II – external resorption : Case series, Mar-Apr 2013.
L.Bergmans, J. Van Cleynenbreugel, E. Verbeken, M. Wevers, B. Van Meerbeek, P. Lambrechts
Cervical external root resorption in vital teeth, 25 September 2002.
A. Maini, P. Durning and N. Drage, Resorption: within or without? The benefit of Cone-Beam Computed Tomography when diagnosing a case of an internal/external resorption defect, 2008
GS Heithersay, Management of tooth resorption, 12 March 2008.