

External cervical resorption and new bioactive materials
18/06/2020
Massimo Giovarruscio
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Effective management of external cervical resorption (ECR) depends on the accurate assessment of the true nature and accessibility of ECR.
The aim of this article is, based on the available evidence, to describe a strategy for the management of ECR with a new bioactive material.
In cases where ECR is supracrestal, superficial and with limited circumferential spread, a surgical repair without root canal treatment is the preferred approach. Bioactive materials that mimic the physical and chemical properties of teeth, and that are moisture-friendly and easy to use, are an attractive alternative to traditional materials. They stimulate apatite formation at the material-tooth interface that knits the restoration and tooth together, guards against secondary caries and seals against microleakage and failure.

Fig. 1
It is well established that ECR is a complex and dynamic process consisting of three main stages: resorptive (initiation), resorptive (propagation) and reparative (remodelling). Unfortunately the aetiology of ECR is still poorly understood.
The presenting features of ECR are highly variable and dependent on several factors, including location and degree of progression. ECR commonly presents as an incidental finding on clinical and radiographic examination, though there may be clinical signs of localized gingival inflammation and bleeding, pulpal involvement, or in more advanced cases apical periodontitis.
The objectives of treatment for ECR are excavation of the resorptive tissue, sealing of the hard tissue defect with an aesthetic biocompatible material and prevention of recurrence of ECR. An indirect or direct pulp cap using a Bioceramic material such as Biodentine or MTA may be indicated if the pulp is close to being affected. These materials have excellent sealing ability, antibacterial properties and biocompatibility. They also promote reparative dentine formation, cementum formation and osteoblast differentiation. The remaining cavity may then be restored with a direct plastic adhesive restoration at the same visit.
During the last decade, a considerable amount of attention has been directed towards the development of so-called bioactive materials. For instance, any fluoride-releasing material, calcium silicate and calcium aluminate-based cements.
These novel products are the dental resins with a bioactive ionic resin matrix. Bioactive materials are a viable treatment options because they are able to release calcium and phosphate ions and to promote the formation of apatite and osteoblasts.
A 55 years old patient came to the clinic 44 with an external resorption below the gum level. Clinically the large cavity is not visibile. With the periodontal probe is possible to test the size and the involvement of buccal periodontal tissue.
The tooth is asymptomatic, patient referred hot and cold only.

Fig. 2
Radiographic evaluation confirmed the presence of a large resorption, with no periapical radiolucency. The x-ray revealed the non-restored osseous compartment and an infiltrative channel present mesially around the canal, in the coronal one third of the root.
The management of ECR is dependent on the accessibility and the restorability of the lesion.
CBCT Scan has an important role in the diagnosis and assessment of the external resorption but the patient preferred to avoid additional X-Ray exposure. Mavridou et al. (2016) described the common characteristics of ECR in teeth with vital pulps. They invariably found the presence of one or more portals of entry with three-dimensional spread of the resorption defect. Supraosseous portals of entry will usually result in crater-like lesions containing predominantly fibrovascular tissue. These are usually managed by an external approach.
A full thickness labial mucoperiosteal flap was reflected following local infiltration anesthesia. Granulomatous tissue was seen involving the buccal surface and part of the distoproximal surface.The area of osseous ingrowth was removed using a sharp scalpel and the defect was refreshed with a round bur. No exposure of the pulp was evident at that stage. The resorptive defect extended from the cervical one third of the crown to the cervical one third of the root, involving the distoproximal line angle, with the defect becoming shallow toward the root.
Rubber dam is mandatory to obtain a full and sterile operative field. It is essential that treatment is carried out with the aid of a dental operating microscope or loupes. Granulomatous tissue has been removed with a sharp Micro-Excavator respecting the pulp tissue. To protect the nerve, an air abrasion with BioGlass powder has been used. A novel Resin-based Bioactive Restorative material has been applied on the pulp. A dual composite has been placed as a final restoration (Sandwich Technique)
6.0 sutures have been removed after 7 days.
21 days later: great healing of the surrounding tissues, no probing, no bleeding no clinical symptoms.
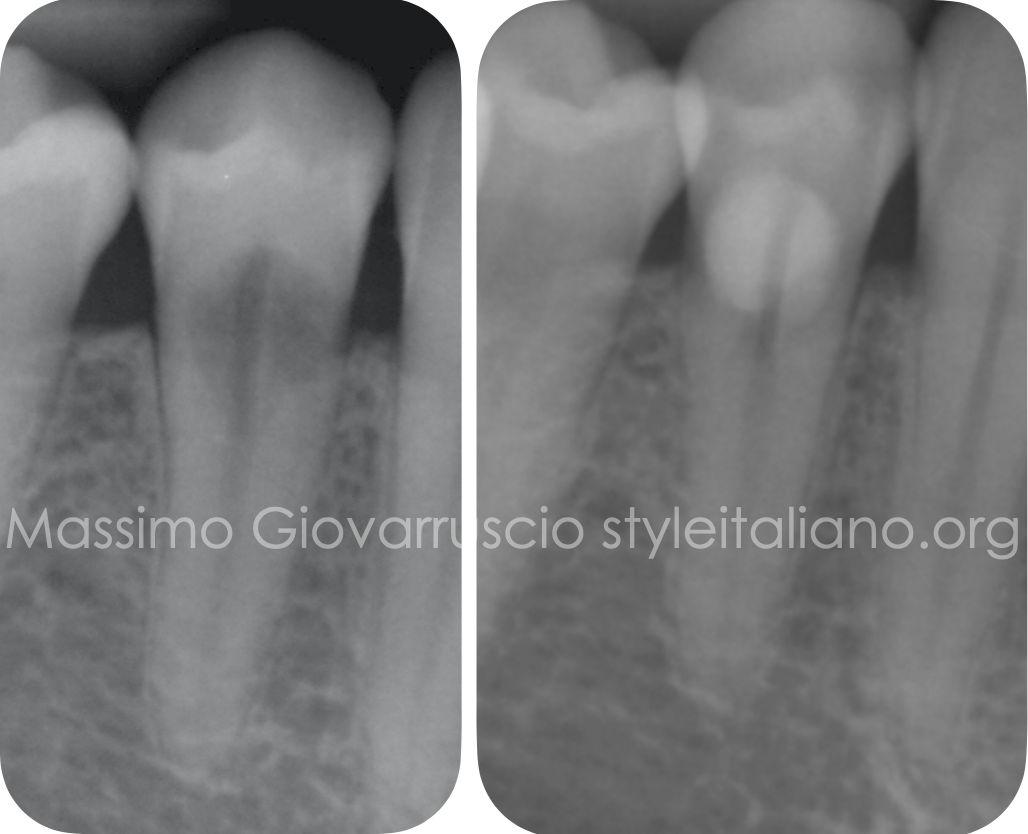
Fig. 3
Post-operative. At a 6 month recall, the patient was asymptomatic and the probing depth was normal with no gingival recession.
The tooth responded positively to vital tests.
Conclusions
Effective and predictable management of ECR depends on the accurate assessment of the true nature of the lesion. The presenting features of ECR are highly variable and dependent on several factors including location and degree of progression. Therefore the clinical and radiographic presentation of ECR is highly variable with no classic presentation.
The objectives of treatment are excavation of the resorptive tissue, sealing of the resultant defect and portal of entry and prevention of recurrence. Treatment options for ECR depend on the extent, nature and accessibility of the resorptive process; in some cases it may be necessary to raise a mucoperiosteal flap. External Cervical Resorption lesions that are accessible and therefore amenable to conservative treatment have a good prognosis. Bioceramic materials are indicated if vital pulp is exposed.
Bioactive materials that mimic the physical and chemical properties of teeth, and that are moisture-friendly and easy to use, are an attractive and novel alternative to traditional materials. They stimulate apatite formation at the interface and seals against micro leakage and failure with the advantage of aesthetics, strength and durability.
Bibliography
-Patel S, Lambrechts P, Shemesh H, Mavridou A. “European society of endodontology position statement: External Cervical Resorption”. Int Endod J 2018 Dec(12):1323-1326
-Mavridou AM, Hauben E, Wevers M, Schepers E, Bergmans L, Lambrechts P.”Understanding external cervical resorption in vital teeth”. Journal of Endodontics 2016 42, 1737– 51
-Patel S, Mavridou AM, Lambrechts P, Saberi N. “External cervical resorption: part 1 - histopathology, distribution and presentation”. Int Endod J 2018 Nov 51(11):1205-1223
-Patel S, Foschi F, Condon R, Pimentel T, Bhuva B. “External cervical resorption: part 2 - management: External Cervical Resorption”. Int Endod J 2018 Dec(12):1224-1238
-Patel S, Foschi F, Mannocci M, Patel K. “External Cervical Resorption: a three dimensional classification”. Int Endod J 2018 Feb:51(2):206-214


