The importance of the tube shift technique of radiography, during root canal treatment of mandibular anterior teeth.
05/05/2022
Garima Poddar
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
One of the leading reasons for an unsuccessful root canal treatment of mandibular anterior, is missing out the presence of a second canal, thus leaving it untreated. (4). In endodontics, parallax technique is preferable for mandibular anterior teeth, to avoid superimposition of canals over each other (1).
This article explores the importance of a tube shift technique while doing endodontic management of a mandibular anterior, in order to decrease the chances of missing a canal.
A root canal treatment with desirable prognosis, is dependent on multiple factors. A significant ground for a failed endodontic treatment of mandibular anterior, could be a missed canal. Mandibular incisors and canines have often showed presence of a second canal, which when left untreated, could lead to an unfavorable outcome. (4) The incidence of two canals in mandibular incisors has been described as 12-35% by numerous researchers after studying the root canal system and its canal configurations. (5). Lack of knowledge of making proper radiographs, could be one of the reasons for such a failure. The paralleling technique provides radiographs with less distortion of image, and in endodontics, this technique has a big advantage, as distortion of details is unwelcomed on a radiograph while performing a RCT. (2). However, both bisecting angle technique as well as paralleling technique could be used. Additionally, the preference of one of these two techniques varies between countries.
But, in teeth with multiple roots and/or multiple canals, a parallax method, which employs use of x-ray tube shift slightly, is preferable in order to avoid superimposition of canals over each other. (1). Powered with the knowledge of presence of two canals, it becomes easier for a clinician to prepare a well-designed access preparation and extend it appropriately bucco-lingually in order to locate a buccal and a lingual canal. (6).
Another advanced radiographic technique, which could be used is cone-beam computed tomography (CBCT) for 3-dimensional volume imaging. However, since the dose of exposure should be as low as reasonably achievable (ALARA principle), along with considering the socio-economic factors, for routine cases of mandibular anterior teeth, a tube shift technique suffice the purpose well.
In addition, tools like magnification and good illumination, help in doing access preparation with more precision.
This article traverses the significance of a tube shift technique while doing endodontic management of a mandibular anterior, in order to decrease the chances of missing a canal.
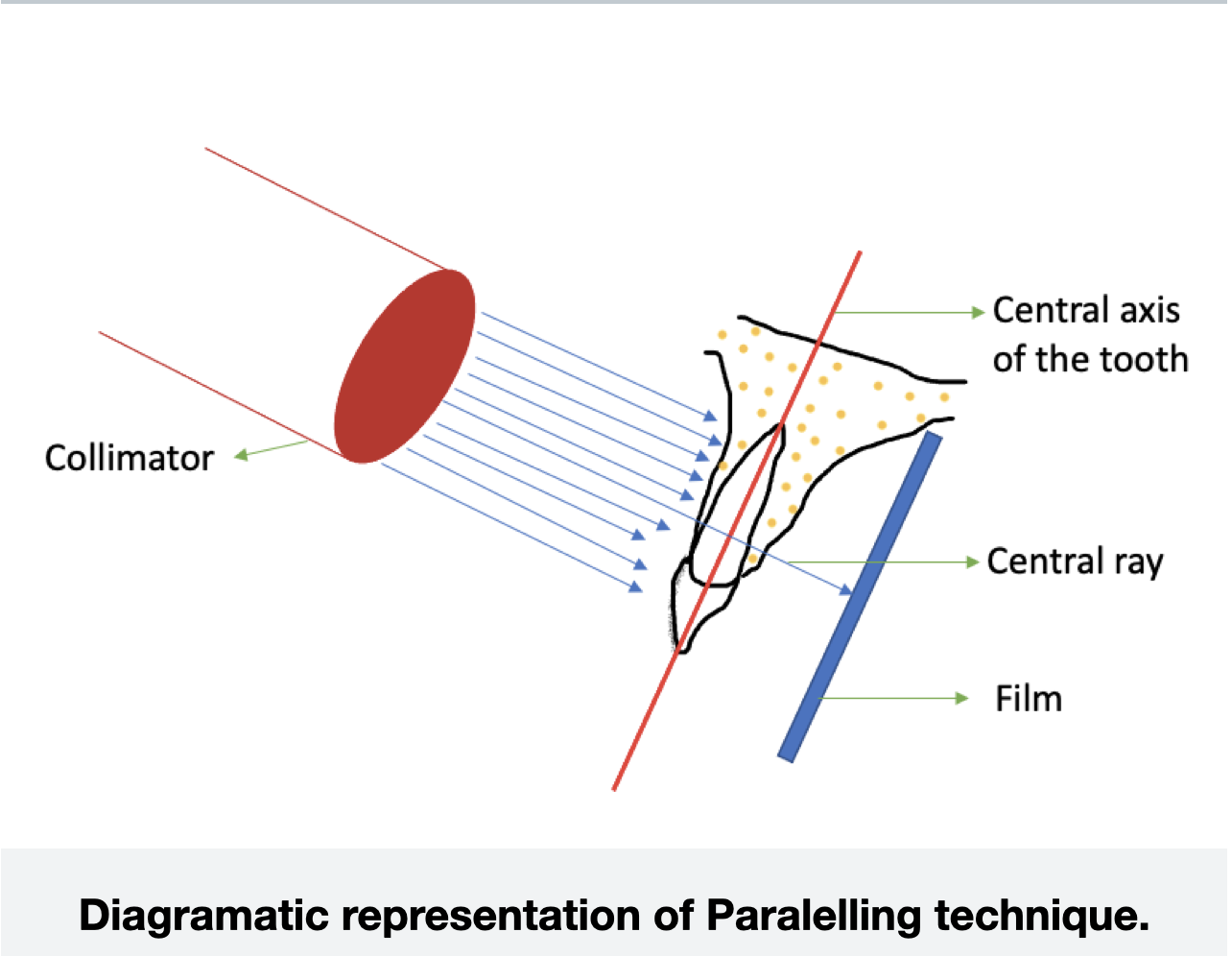
Fig. 1
The paralleling technique for intra-oral radiography.
This technique acquires its name according to the film placement, which is parallel to the long axis of the tooth. This method, has shown minimum distortion of image. (7)
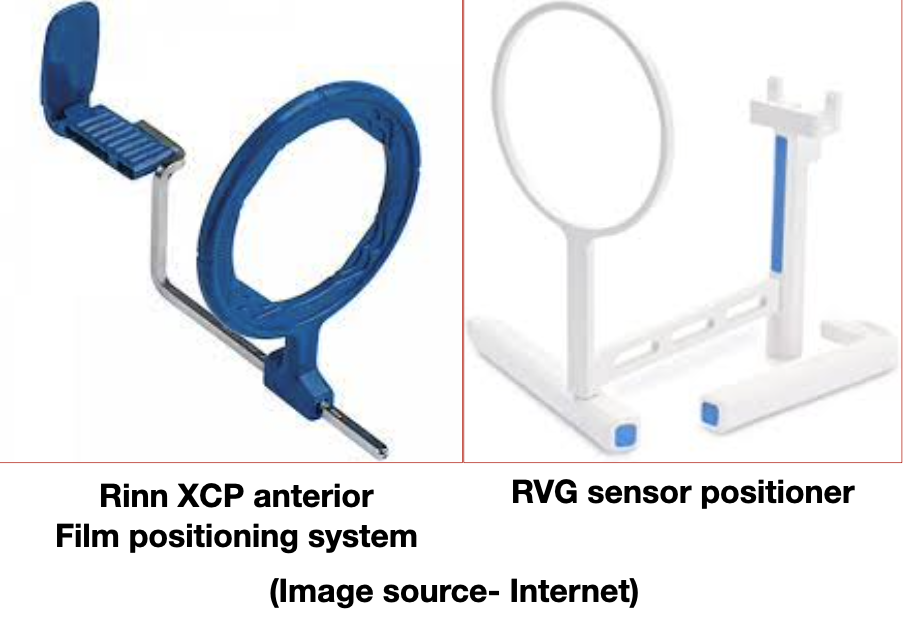
Fig. 2
The paralleling technique for intra-oral radiography.
For this technique, use of film holders/ rvg sensor holders are really helpful in order to support the film/sensor in the patient’s mouth properly.
However when this technique is employed for multirooted teeth or teeth with multiple canals, there could be superimposition of the canals over each other.
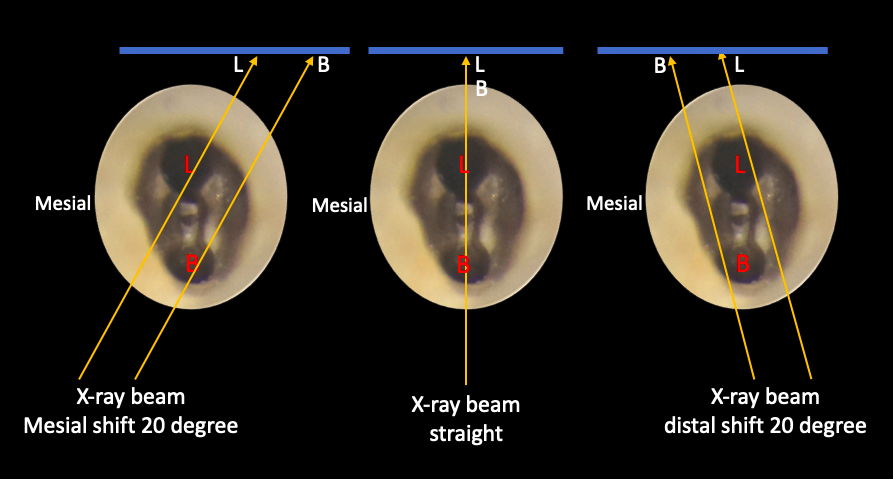
Fig. 3
Tube shift technique.
One of the technique frequently used to obtain three dimensional information about the root canal system is the tube shift technique. Alternative names for this method are- Clark’s rule ( described by Clark in 1910) and the buccal object rule.
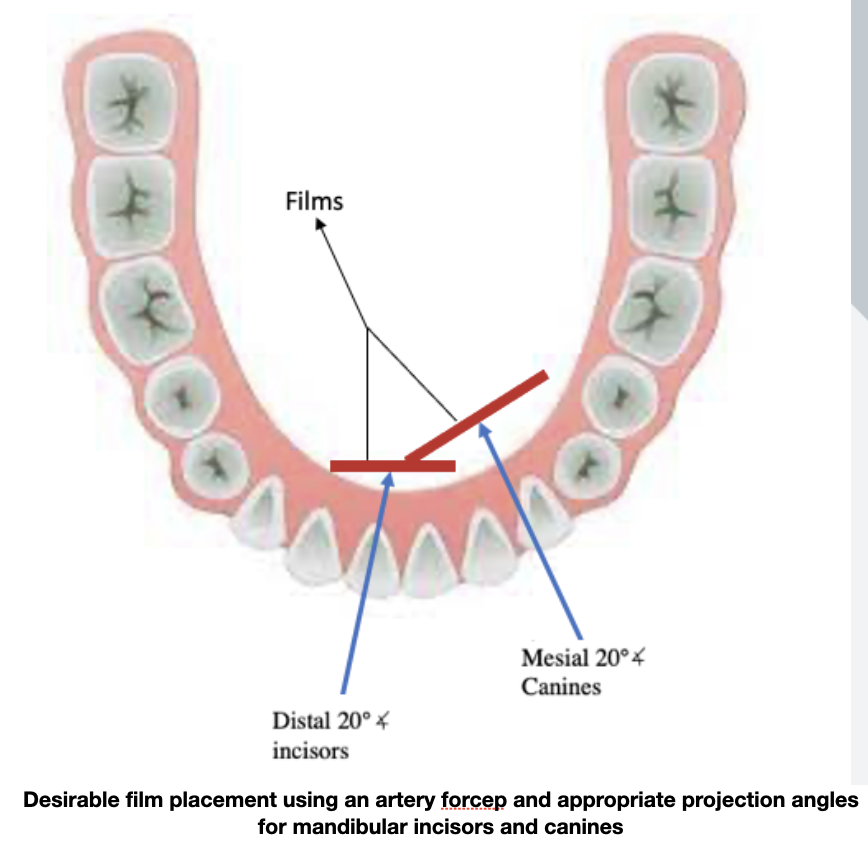
Fig. 4
It is also sometimes referred to as parallax technique. During this procedure, the x-ray tube/collimator is shifted to some degree, horizontally or vertically for the second radiograph.(1) This method also points out the spatial position of an object.
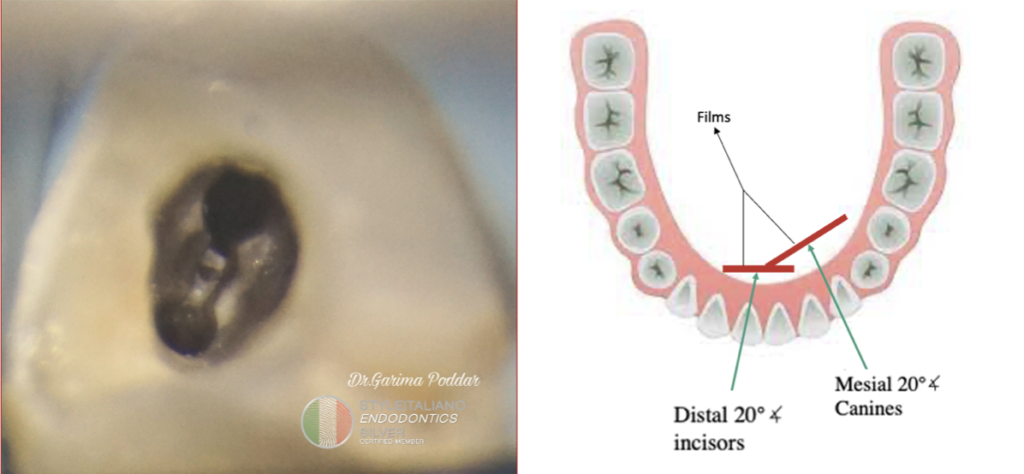
Sometimes, due to limitations like- less lingual sulcus depth, or stiff tongue, it might be difficult to use a film positioner. In such a scenario, usage of artery forceps or haemostat for holding the film in place serves to be helpful.
The diagram, shows the precise film positions and angulation of central x-rays while using a haemostat. The distal projection is useful in case of mandibular incisors, while mesial projection is indicated for mandibular canines.
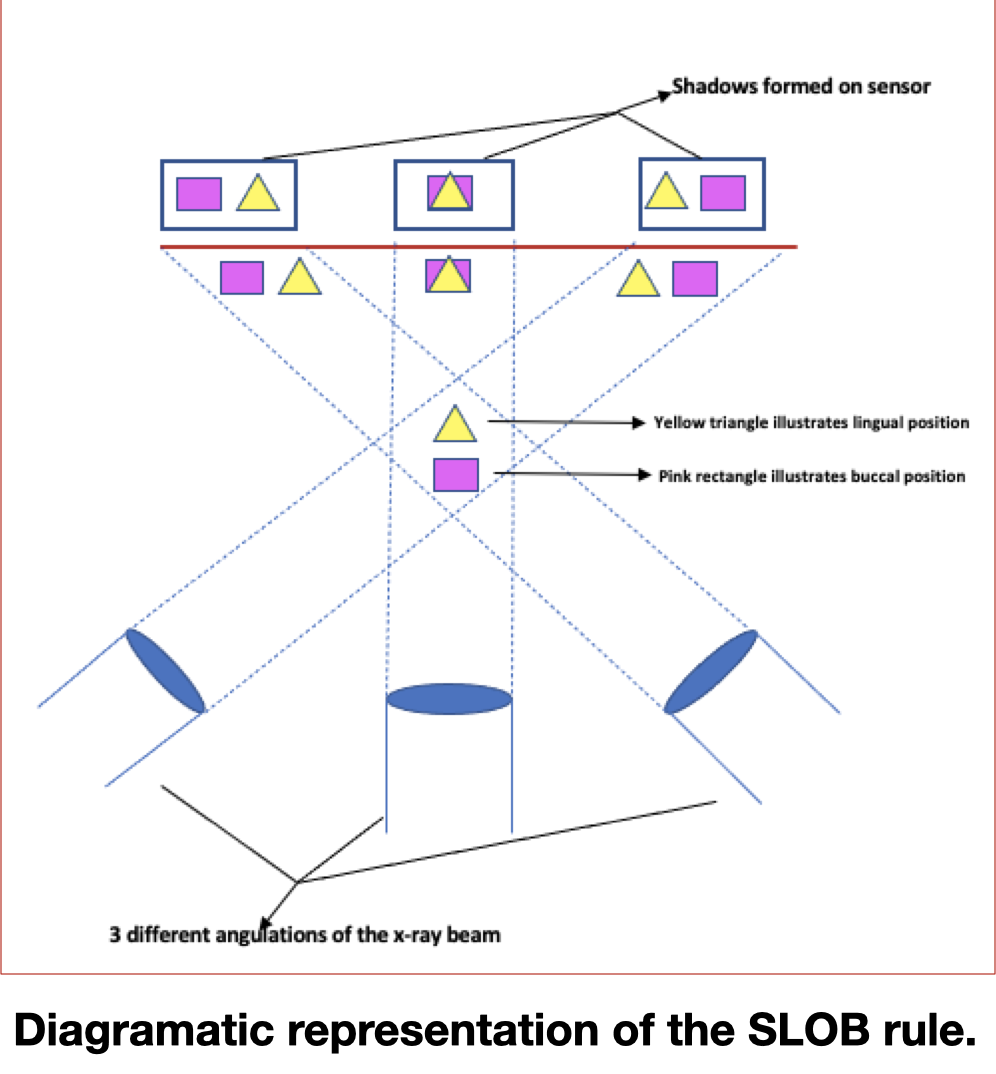
Fig. 5
The reasoning for this method is as follows.
The comparable positions of x-ray images of two individual objects change, when the angle of projection at which the images were made change.
This relationship is usually termed as SLOB rule. The acronym SLOB stands for: same lingual, opposite buccal.
White and Pharoah have described further in their book, that when the x-ray tube is shifted from a more mesial angle and the object under consideration, also moves mesially with respect to the object of reference, the object lies lingual to the reference object. Alternatively, if the tube is shifted mesially and the object appears to move distally, it lies on the buccal aspect of the reference object.
In case of a mandibular incisor or canine, this method of tube shift would allow viewing of all the canals and also would help in opening up narrow canals on the radiograph.
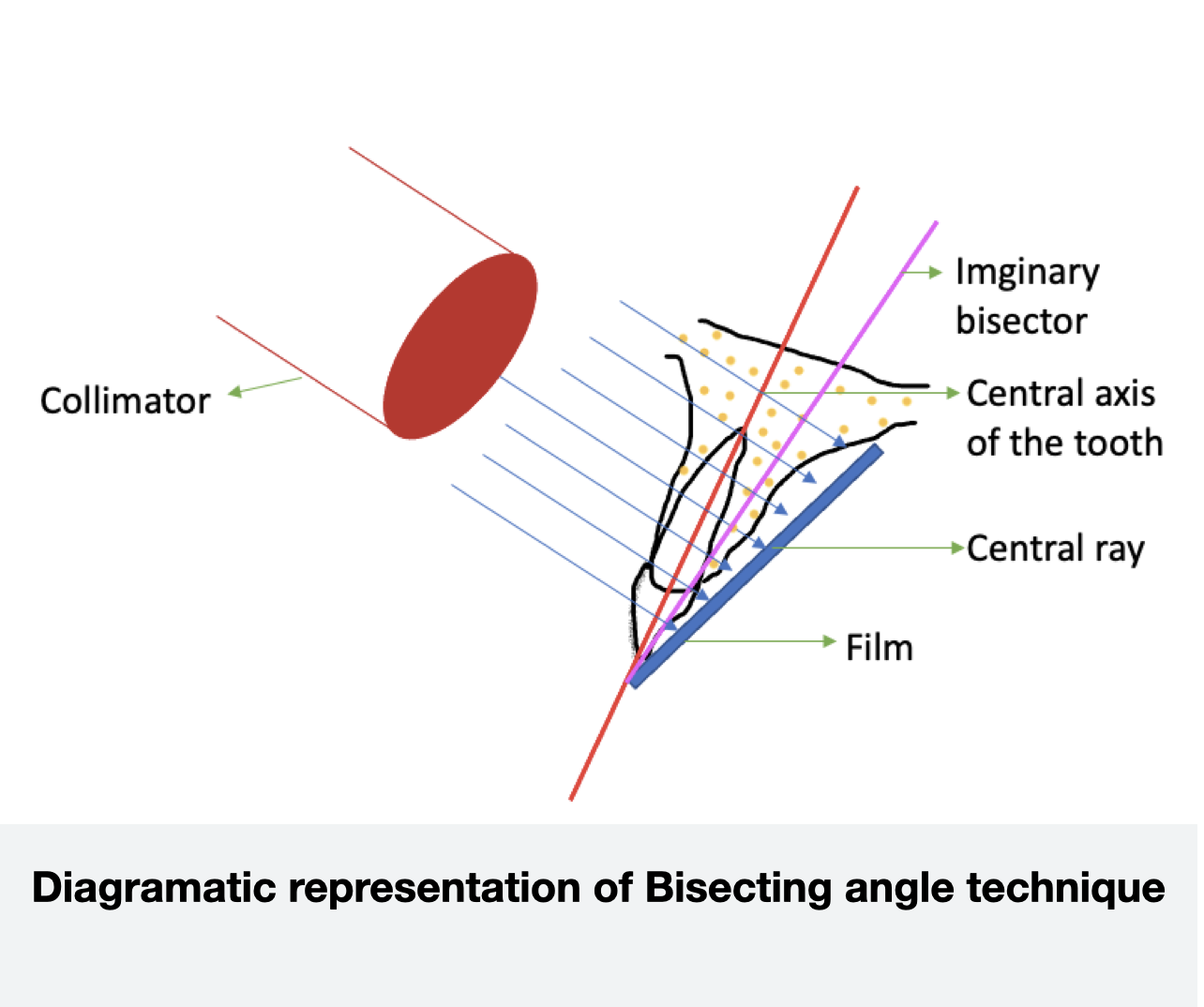
Fig. 6
Bisecting angle technique.
For this technique, the operator requires to place the film/sensor as close to the teeth as possible. Care should be taken to prevent deformation of the film. Over here, the x-rays are directed perpendicular to an imaginary plane bisecting the angle between the teeth and the film/rvg sensor.
A tube shift technique can easily be utilized with bisecting angle technique also and a comparative x-ray image could provide valuable details about the root canal morphology of that case.
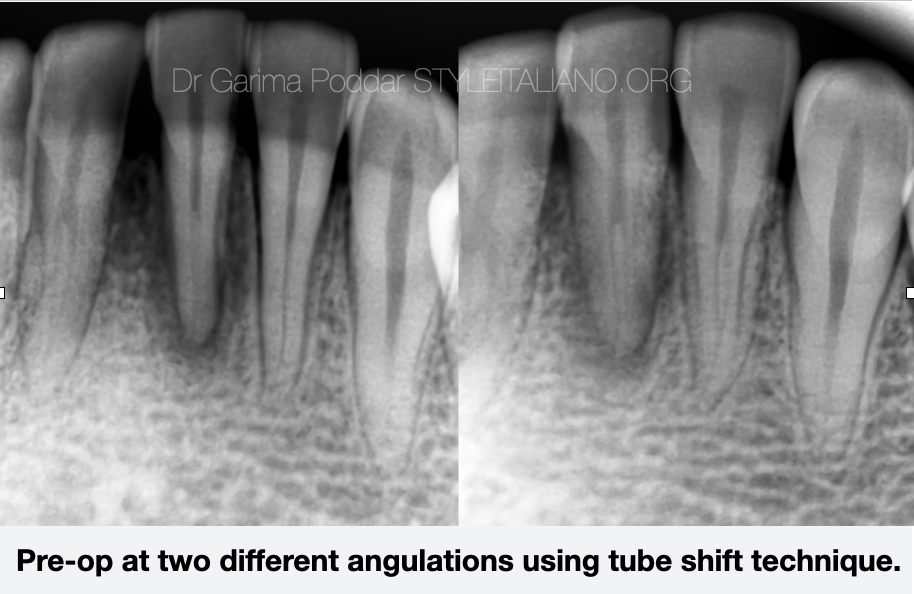
Fig. 7
This article further shares two cases – case-1 for a mandibular central incisor and case 2 of mandibular canine, to illustrate and correlate the concepts clinically.
Case 1
While making preoperative x-ray images of tooth number 31, tube shift technique revealed the presence of two canals very clearly, thus helping in more predictable work during access preparation of this tooth.
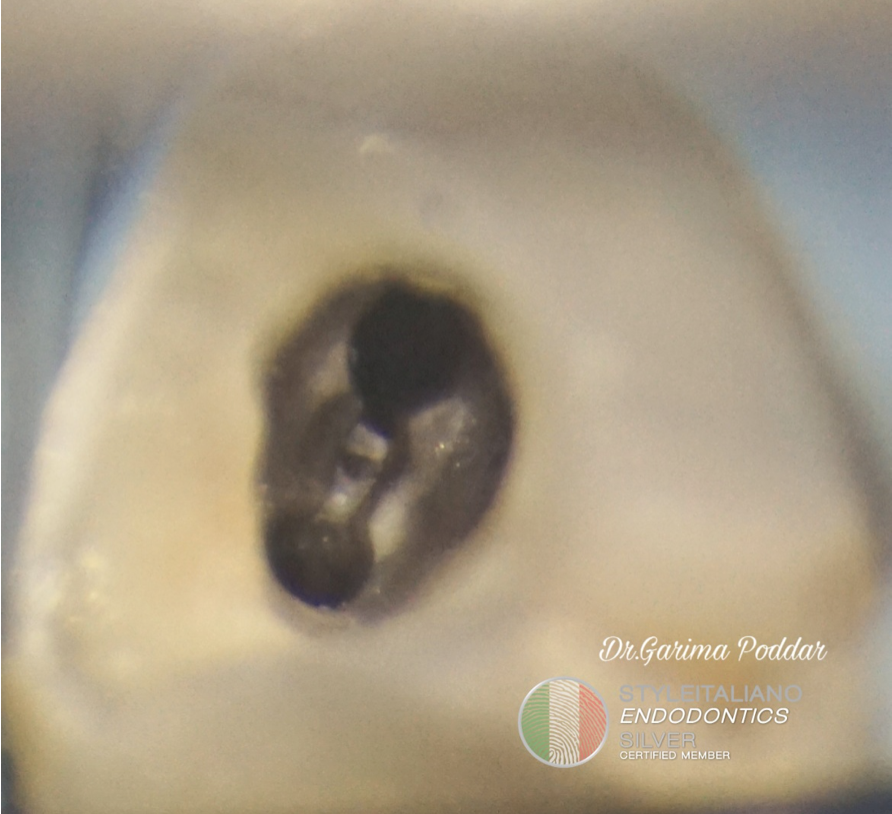
Fig. 8
Case 1
An appropriate and ergonomic access preparation is of high importance for smooth workflow during root canal treatment of such teeth. If the clinician is unable to prepare a good access, it poses added challenges during shaping, cleaning as well as obturation procedures. In case of mandibular incisors, owing to their small size, a good preoperative radiograph, followed by use of magnification, illumination and smaller sized instruments aids in conservative yet accurate access design. If not properly diagnosed, lingual canal in such cases might be missed more often than the buccal canal. So, the clinician should extend the access prep buccolingually properly in such a situation. (4)
In this case of tooth number 31 also, proper extension of access cavity both buccally as well as lingually, assisted in effortless workflow throughout the rct procedure.

Fig. 9
Case1
For the same case, post-operative radiographs at two different angulation using the tube shift technique, shows that the details of both the canals can we well appreciated with an angulated x-ray image.
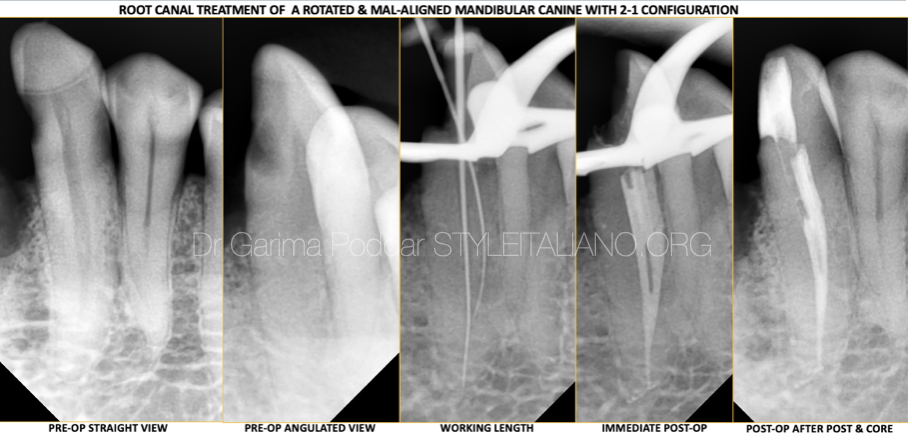
Fig. 10
Case 2
In a case of endodontic treatment of tooth number 33 which was malaligned and rotated, it was an added challenge to make proper radiographs with good diagnostic value. In that condition, a comparitive x-ray image using tube shift tehnique was indeed a fruitful decision.
The radiographs were compared and read well, which helped all throughout the rct procedure. The canals had a 2-1 configuration. Even during working length determination, radiograph made with an approximate angulation of 20 degree tube shift revealed proper details of extent of insertion of the files inside the canals.
Case 2
This case video shows the step of injection of bioceramic sealer- ceraseal in the 2-1 canal anatomy during the obturation procedure.
Conclusions
A meticulous evaluation of pre-operative radiographs made at different angulations following tube shift method, is a crucial step before commencement of endodontic procedure.
During access preparation, care should be taken to do proper extension of the cavity design buccolingually ,as well as a gingival extension below the cingulum could prove to be helpful in searching for second canal in mandibular anterior teeth. When established protocol and steps are involved during a root canal treatment, changes of errors like missing a canal could largely be avoided in day to day practice.
Bibliography
- Yusof, Zamros & P, Nambiar. (2007). Radiographic Considerations in Endodontics. Malaysian Dental Journal.
- Bridgman JB, Campbell DJ. Radiography in endodontics. N Z Dent J. 1995 Jun;91(404):62-4. PMID: 7675349.
- V. Hegde, S. Kokate, and Y. Shahu, “An unusual presentation of all the 4 mandibular incisors having 2 root canals in a single patient—a case report,” Endodontology, vol. 22, no. 2, pp. 70–74, 2010.
- Vandana B. Kokane, Swapnil N. Patil, Mohit K. Gunwal, Rajesh Kubde, Swaraj Atre,"Treatment of Two Canals in All Mandibular Incisor Teeth in the Same Patient", Case Reports in Dentistry, vol. 2014, Article ID 893980, 4 pages, 2014.https://doi.org/10.1155/2014/893980
- K. S. Al Fouzan, A. Almanee, J. Jan, and M. Al-Rejaje, “Incidence of two canals in extracted mandibular incisor teeth of Saudi Arabian samples,” Saudi-Endodontic Journal, vol. 2, no. 2, pp. 65–69, 2012.
- S. Cohen and K. Hargreaves, Pathways of the Pulp, Elsevier Mosby, 12th edition, 2020
- S.C. White and M.J. Pharoah, Oral radiology principles and interpretation, 6th edition, 2009.