Smart decisons for your retreatments w/ MisurEndo, ExtEndo, Multiplo & Prexo M
05/10/2021
João Meirinhos
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Apical periodontitis is a local inflammatory response which due to the presence of microorganisms within an infected root canal system1. One of the main goals in endodontics is to be able to prevent this infectious disease or, in cases it already happened with consequences in the periapical tissues, create conditions to a good periapical healing2. Several authors3 have reported that apical periodontitis is more prevalent in root canal treated teeth. In these cases, the treatment outcome might be influenced by the obturation characteristics such as poor condensation, short fills, or extrusion of material into the the periapical tissues4.

Fig. 1
A 25-year-old male patient was referred by general practitioner with an inadequate previous root canal treatment on tooth 21 who was diagnosed with a symptomatic apical periodontitis.
After evaluation and recognition the cause of treatment failure, a nonsurgical approach was proposed.
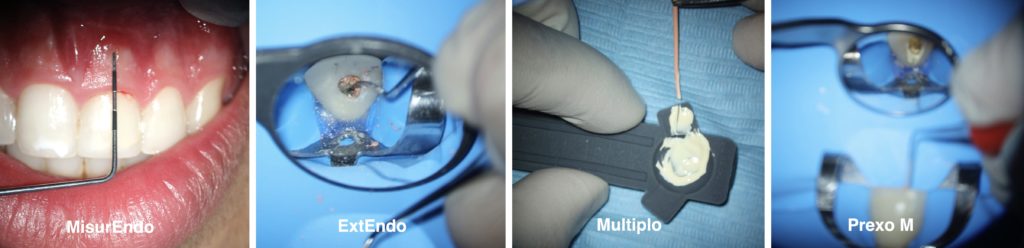
Probing was done with MisurEndo (designed also for conventional diagnostic probing) and was within normal depths in all surfaces with a fistula associated to the maxillary left central incisor.
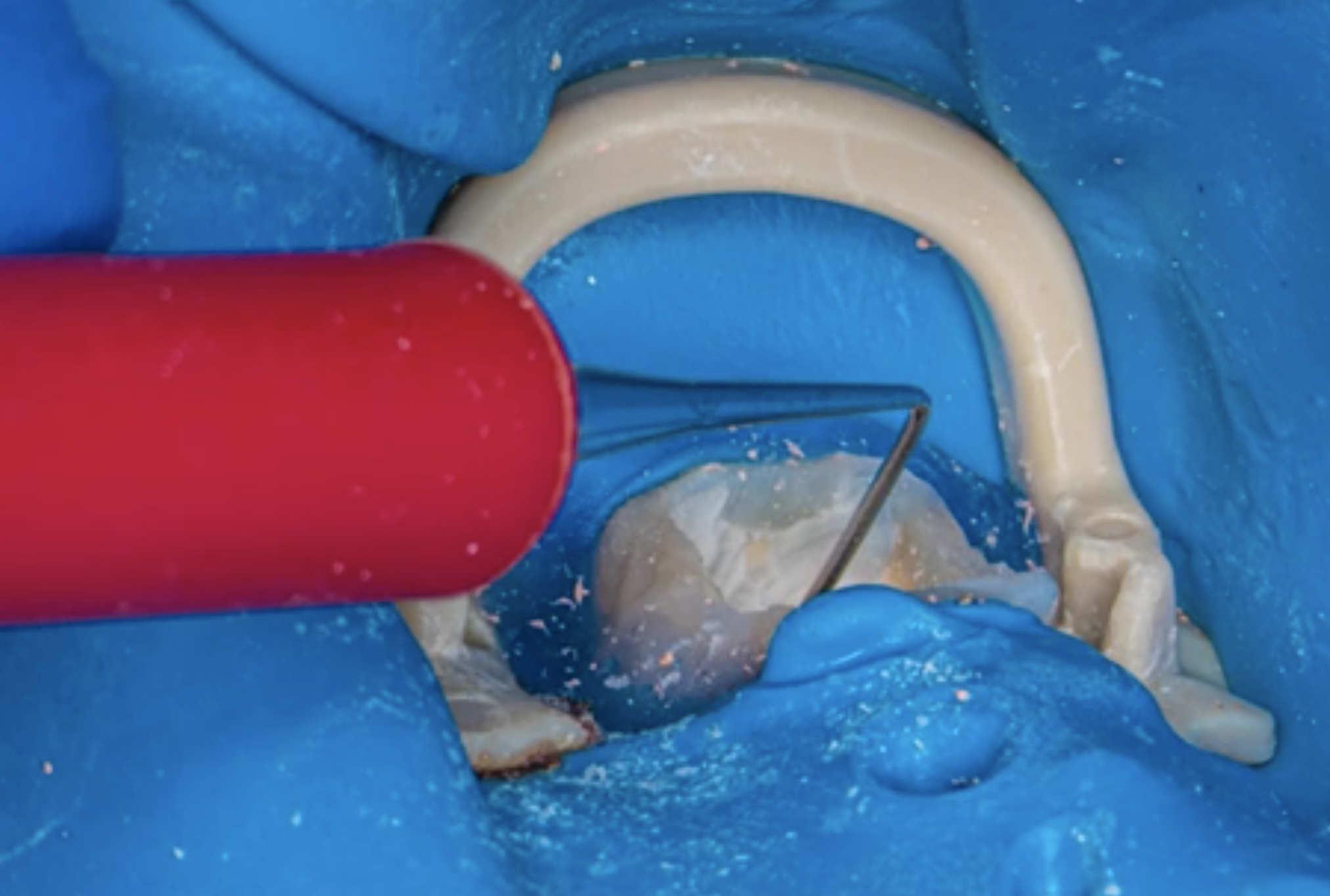
After removing old restoration, the root canal was identified and retreated with the help of ExtEndo (useful for removing gutta-percha along the root canal walls).

Fig. 2
To determine the working length, the electronic apex locator Root ZX (Morita Corp. Tokyo. Japan) was also used. All the canal was shaped with Reciproc files (r25, r40, r50) (VDW, Germany) according to the manufacturer’s instructions.

Fig. 3
Copious irrigation with 5mL syringe and a 27G notched needle with 5,25% sodium hypochlorite was done all throughout the endodontic treatment.
The canal was dried with paper points (Zipperer, VDW, Munich, Germany).
To work with microscope, it is necessary to have the maximum amount of light to illuminate the depths of the root canal system and no distortion. Standard mirrors result in double images and a loss of definition. On the other hand, rhodium mirrors reflect 75% of the light. Mirror and Multiplo can be attached and work as a combined tool (mirror, working length measurement and a place to mix and collect the endodontic sealer)
The canals were filled with gutta-percha and resin sealer (AH plus, Dentsply Tulsa Dental, USA) with a continuous wave of obturation technique with the B&L system (Biotech, USA). The material was condensed with PrexoM, a simplified plugger with an innovative design.

Fig. 4
Intracoronal sealing was done with a flowable composite resin and the crown was subsequently temporarily restored .
Conclusions
Endodontic treatment failure appears not to be associated with only to one factor5. Several studies from different research groups are unanimous highlighting the high prevalence of periapical periodontitis due to the poor quality of root canal treatments. Extra care should be taken to have a proper apical and coronal seal of all the root canal system and teeth with root fillings should be regularly monitored.
Bibliography
- Abbott, P. V. (2004). Classification, diagnosis and clinical manifestations of apical periodontitis. Endodontic Topics, 8(1), 36–54.
- Al-Omari, M. A., Hazaa, A., & Haddad, F. (2011). Frequency and distribution of root filled teeth and apical periodontitis in a Jordanian subpopulation. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 111(1), e59–e65.
- De Moor, R. J. G., Hommez, G. M. G., De Boever, J. G., Delme, K. I. M., & Martens, G. E. I. (2000). Periapical health related to the quality of root canal treatment in a Belgian population. International Endodontic Journal, 33(2), 113–120.
- Ray, H. A., & Trope, M. (1995). Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. International Endodontic Journal, 28(1), 12–18.
- Meirinhos, J., Martins, J. N. R., Pereira, B., Baruwa, A., Gouveia, J., Quaresma, S. A., … Ginjeira, A. (2019). Prevalence of apical periodontitis and its association with previous root canal treatment, root canal filling length and type of coronal restoration – a cross‐sectional study. International Endodontic Journal.