Scouting The Root Canal
08/07/2016
Massimo Giovarruscio
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
As discussed on the previous article, the manual preflaring creates a glide path for safer use of hand files and NiTi rotary instrumentation. Canal scouting is the first phase of canal instrumentation, during which procedural difficulties or errors might more frequently occur.
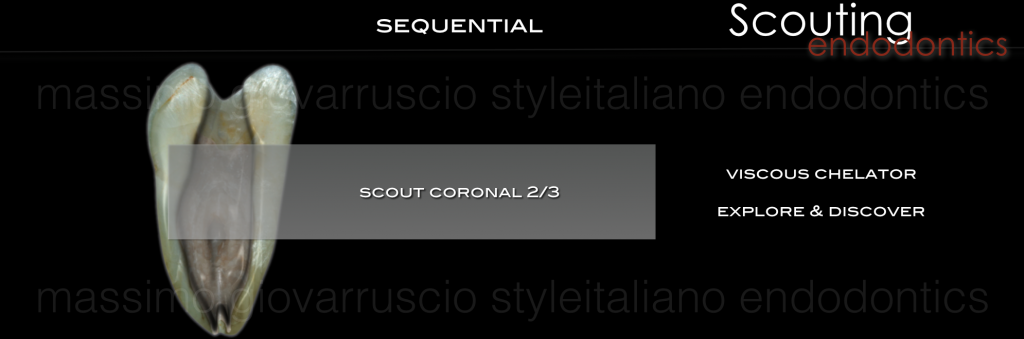
Fig. 1
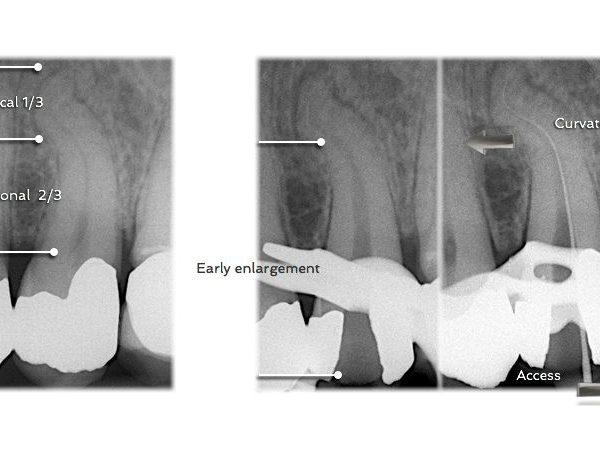
Scouting Coronal 2/3 provide information regarding root canal system anatomy and give important feedback regarding the canals degree of curvature, recurvature, or if there is a dilaceration Clinicians need to appreciate the five commonly encountered anatomical forms which include canals that merge, curve, recurve, dilacerate or divide.
When straightline access has been completed and all the orifices have been identified, attention is directed towards preparing the root canal. If the pulp is vital and bleeding, the chamber is filled brimful with a viscous chelator. In the instance where the pulp is necrotic, the chamber is irrigated and completely filled with a 5,25% solution of warm NaOCL. With the SCOUTING the smaller stainless steel files are measured on the preo-op radiograph and prebend to conform to the anticipated full length and curvature of the root canal. Stainless steel 0,02 tapered 10K hand files is utilized to explore or scout the coronal 2/3 of the root canal.
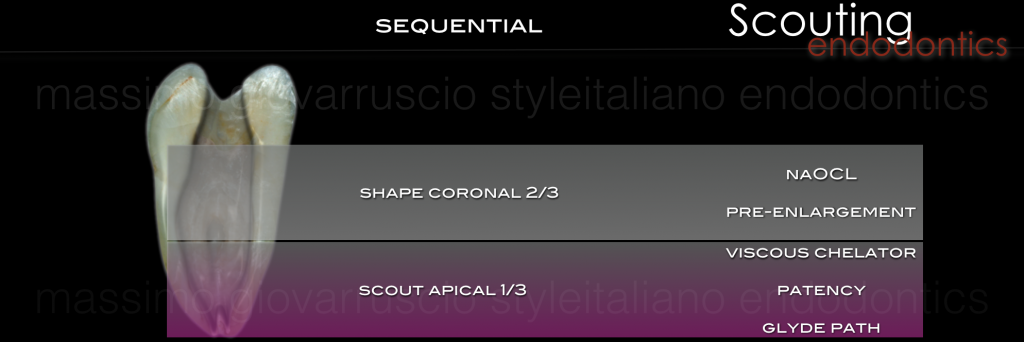
Fig. 2
After negotiation the coronal 2/3, the canal is flushed with NaOCL and may be pre-enlarged using hand instruments, gates gladden drills utilized like a brushes, or rotary NiTi shaping files.
With the coronal 2/3 optimally prepared and filled with irrigant, the apical 1/3 is then scouted and reconnaissance information gathered. Small hand files are used (08K or 10K file) to negotiate the rest of the canal, confirm a smooth glide path to the terminus and establish patency.

Fig. 3
In complex anatomies with small, long and potentially multiplanar canals, it is not possible to immediately pass a 10 K-file initially to the root end. Subsequently, the clinician with the SCOUTING may try to use smaller files to the apex. However, 06K file and 08K file are typically not needed to enlarge the glide path to the apex unless it is an extraordinarily difficult case.

Fig. 4
The apical foramen will always be larger than a 10K file; therefore any resistance met prior to the apex is likely due to curvature or irregularity in the canal. As a result, opening up the canal with a 10K file in small increments can be an efficient way to follow a reproducible glide path, while minimizing the likelihood of creating a ledge or blockage in the canal.
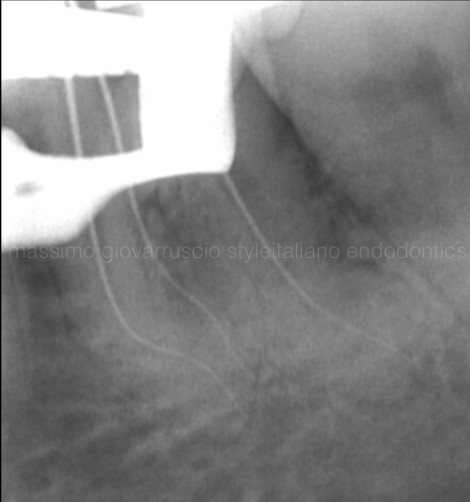
Fig. 5
The TIP of the SCOUTING is that the file should never be forced apically because the risk of creating a ledge is greatly increased. If the tip of the file never binds into the canal wall, it is impossible to make a ledge.

Fig. 6
The Post-Op radiograph shows how the original anatomy has been preserved after root canal instrumentation. Preflaring and Scouting guarantee a well respected of the entire root anatomy.

Fig. 7
Canals just present with anatomic impediments such as straight canal with apical irregularity, curved canal with irregularity and abruptly bent canal.
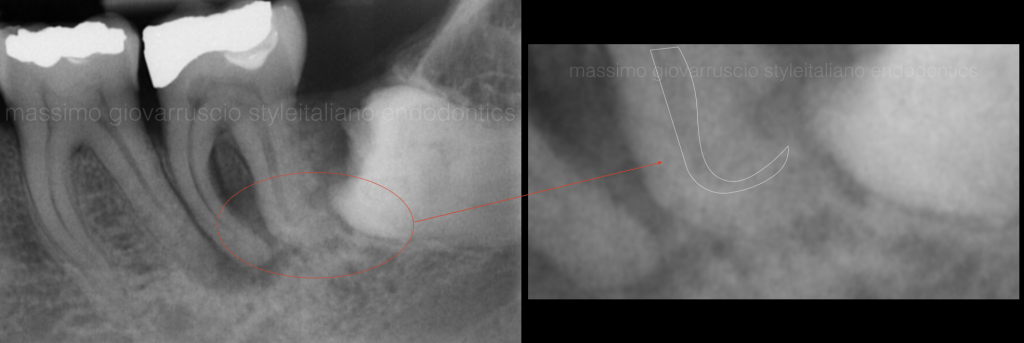
Fig. 8
This canals require cleverness and persistence to traverse. Impediments are identified by the tactile sense (felt through the file handle) of loose resistance to apical file placement. This occurs because the tip of the file is hanging up in a irregularity, rather then grinding to length and beyond.
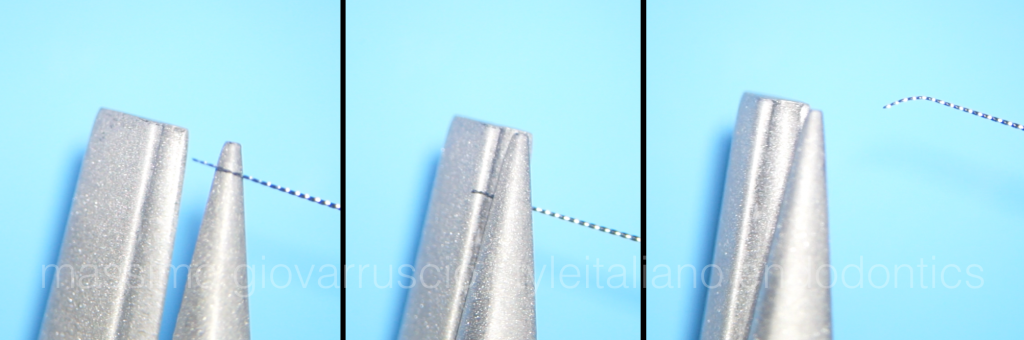
Fig. 9
When an impediment to apical progress is met, remove the file, smoothly bend the very last 2mms with file bending plier (EndoBender), align the directional mark on the silicon stop toward the file bend, and you are able for a path around the impediment.
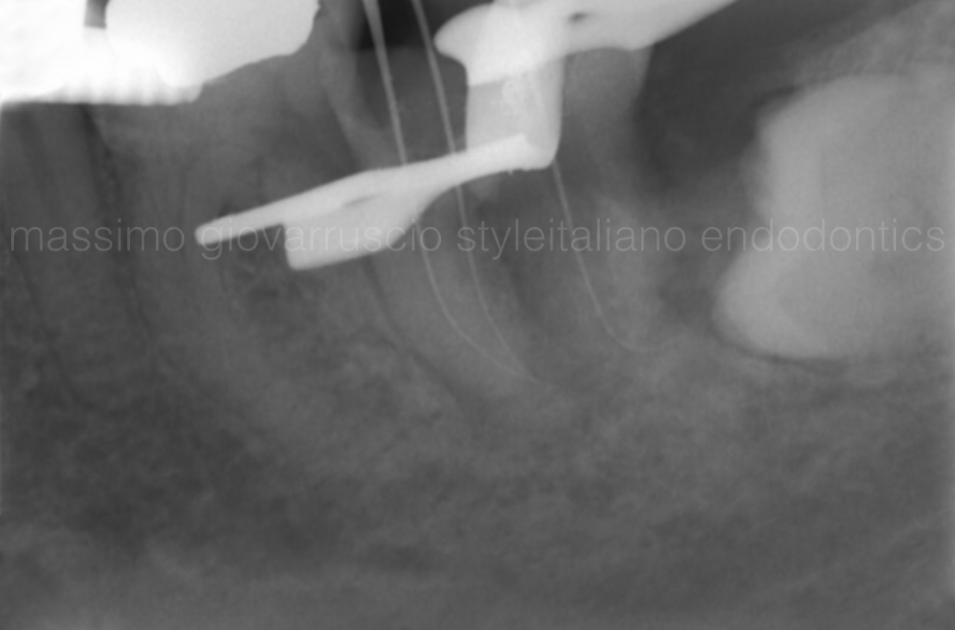
Fig. 10
When scouting a careful watch-winding motion is used to advance the file trough the impediment. When the impediment is met, pull back a mm, turn the file tip in a new direction, move it apically with a wiggle and see if it advances. If not, pull back, redirect the bent file tip and see if it drops. Repeat, if apical progress is seen, until patent. An apex locator and a radiograph control is essential to check whether the terminus has been reached after an impediment is successfully traversed.

Fig. 11
Post operative radiographs shows a complete tridimensional root canal filling and the respect of the complex anatomy.

Fig. 12
In challenging cases, many attempts may be required when scouting the canals. As soon as the file tip moves beyond the impediment, it will drop deeper into the canal.
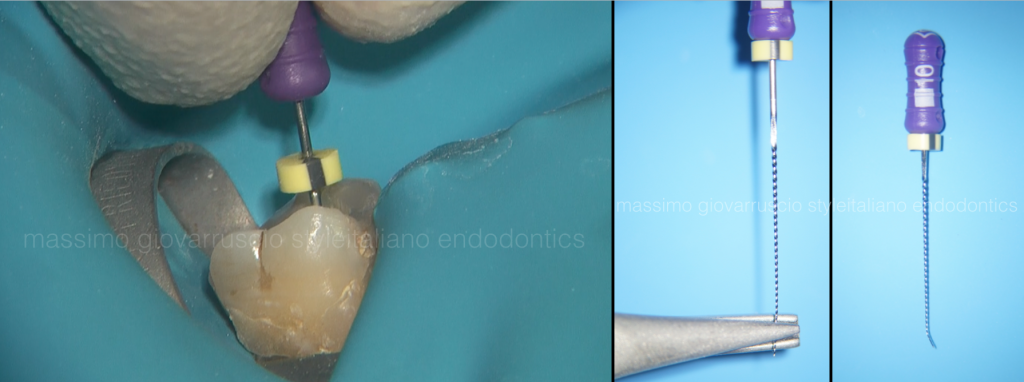
Fig. 13
During this scouting, the directional on the silicone stop informs the clinician about the direction of the bent file tip as it traverses the impediment, in essence, mapping the path. Wiggle the file and move deeper, and work it, checking it with an apex locator lead until length is reached.
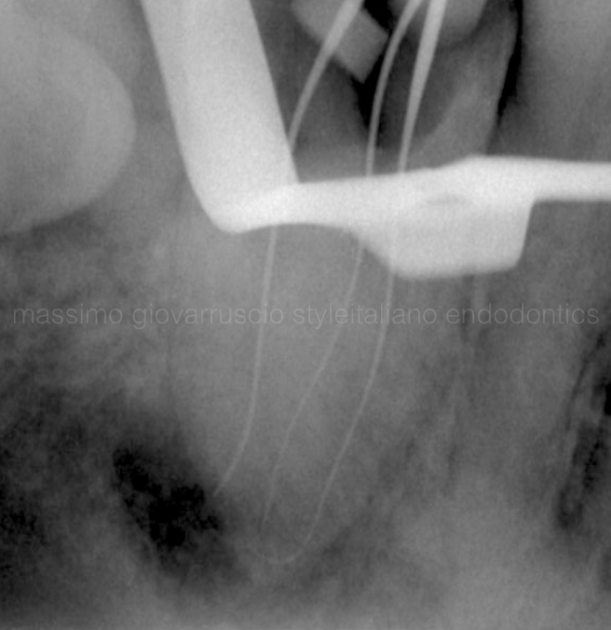
Fig. 14
Once past the impediment, avoid withdrawing the file to the impediment level as the file has inevitably straightened and will no longer traverse it without being withdrawn, rebent, and re-inserted.
In the canal with a double impediment of S-shaped curvature, the present fill will drop when directed around the first bend in the canal but will again meet loose resistance to apical file placement as it encounters the second canal bend. In this case, pull the file back slightly, turn it 180 degrees, give it a wiggle, and see if it catches or just drops to length.

Fig. 15
With bent files and stop indicators, you should be able to mentally map the canal path around the impediments and thereafter easy dance around them and get the job done!
Conclusions
This article has described the rationale for scouting and then pre-enlarging the coronal 2/3 of the canal before scouting and finishing the apical 1/3. Scouting and patency decisively influences the creation of a sufficient and secure Glide Path that will be described in the further article.
Bibliography
- Roane JB, Sabala CL, Duncanson MG Jr. The balanced force concept for instrumentation of curved canals. J Endod. 1985, 11: 203-211.
- Schilder H: Cleaning and shaping the root canal system, Dent Clin North Am 1974, 18:2. 269-296.
- Weine FS, Kelly RF, Lio PJ. The effect of preparation procedures on original canal shape and on apical foramen shape. J Endod. 1975 Aug;1(8):255-62.
- Ruddle CJ. Ch. 8, Cleaning and shaping root canal systems. In Pathways of the Pulp, 8th ed., Cohen S, Burns RC, eds. St. Louis: Mosby, pp. 231-291, 2002.
- Ruddle, CJ. Current concepts for preparing the root canal system. Dentistry Today, Feb 2001.
- Buchanan LS. Negotiating and shaping around anatomic canal impediments tactile clues, bypass technique, shaping procedural flow. Defend course, Santa Barbara 2016.
- Debelian G, Norway &Trope M. Scouting the root canal with dedicated NiTi files. Endodontics International 22 January 2013.
- Mounce RE. Endodontic techniques for scouting the apical thirds of root canals. J Calif Dent Assoc. 2006 Mar;34(3):209-12.
- Buchanan LS. Endodontic Shaping Procedures: The Past, Present, and Near Future. Dent Today. 2015 Sep;34(9):102, 104-7.