Mid-Root Perforation Repair : A Case Report
26/05/2020
Marc Habib
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Endodontic perforation is an iatrogenic procedural error defined as a communication between the root canal system and the periodontal attachment apparatus through the root canal walls.
This defect may occur on any given tooth at any stage of root canal therapy, from access cavity to post space preparation.
Same day Emergency appointment of a 45 year old patient with Acute Apical Abscess on tooth #23. The Patient was referred to another colleague since I was unable to receive him on so short notice. The fellow dentist initiated the retreatment… Unfortunately it was very difficult to locate the canal through crown & fiber post. The second day he was referred back to me with mid root perforation and still very much in Pain!!
The clinical situation showed no sinus tracts, no mobility but huge swelling under the nose with extreme pain and tenderness.
Radio-graphical examination showed large canal space above the deep canal space with a medium size lesions surrounding the apex.
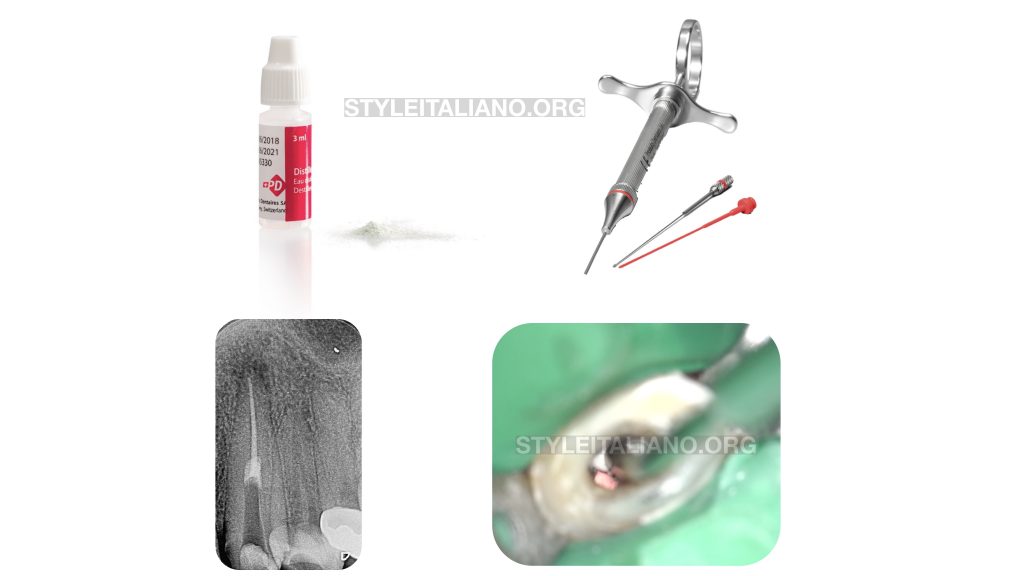
After a pre Op Xray I tried locating the canal under Microscope and with ultrasonics but in vain….

Fig. 1
I adjusted his medication and ordered a CBCT to be able to locate the position of the canal and try to find it clinically the following day…
CBCT study showowing the extent of the perforation:being on the Buccal and Mesial aspect of the root.
After access cavity modification, ultrasonic was used under microscope and indirect vision guided by 2 black reference points made on the distal and palatal occlusal aspect of the access cavity since CBCT examination showed perforation to be Buccal and Mesial!
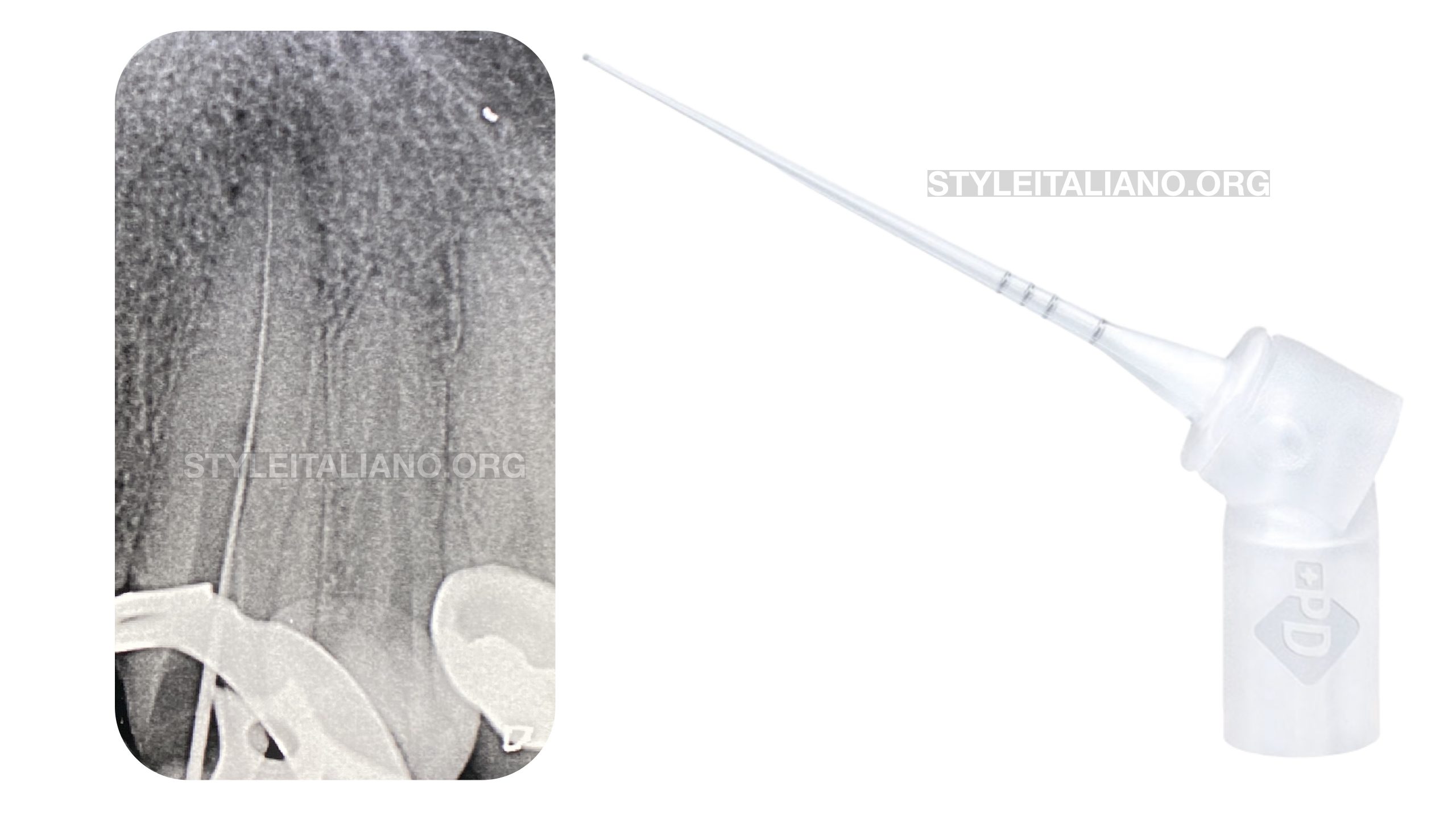
Fig. 2
Then using C+ file number 15 (Dentsply Sirona, Ballaigues, Switzerland) the canal was found and shaped with PTG F1 25mm(Dentsply Sirona, Ballaigues, Switzerland).
Once canal was shaped Pus was observed flushing from the canal. Copious irrigation was made using sodium hypochlorite 5.25% with IrriFlex (Produits Dentaires SA, 1800 Vevey, Switzerland)
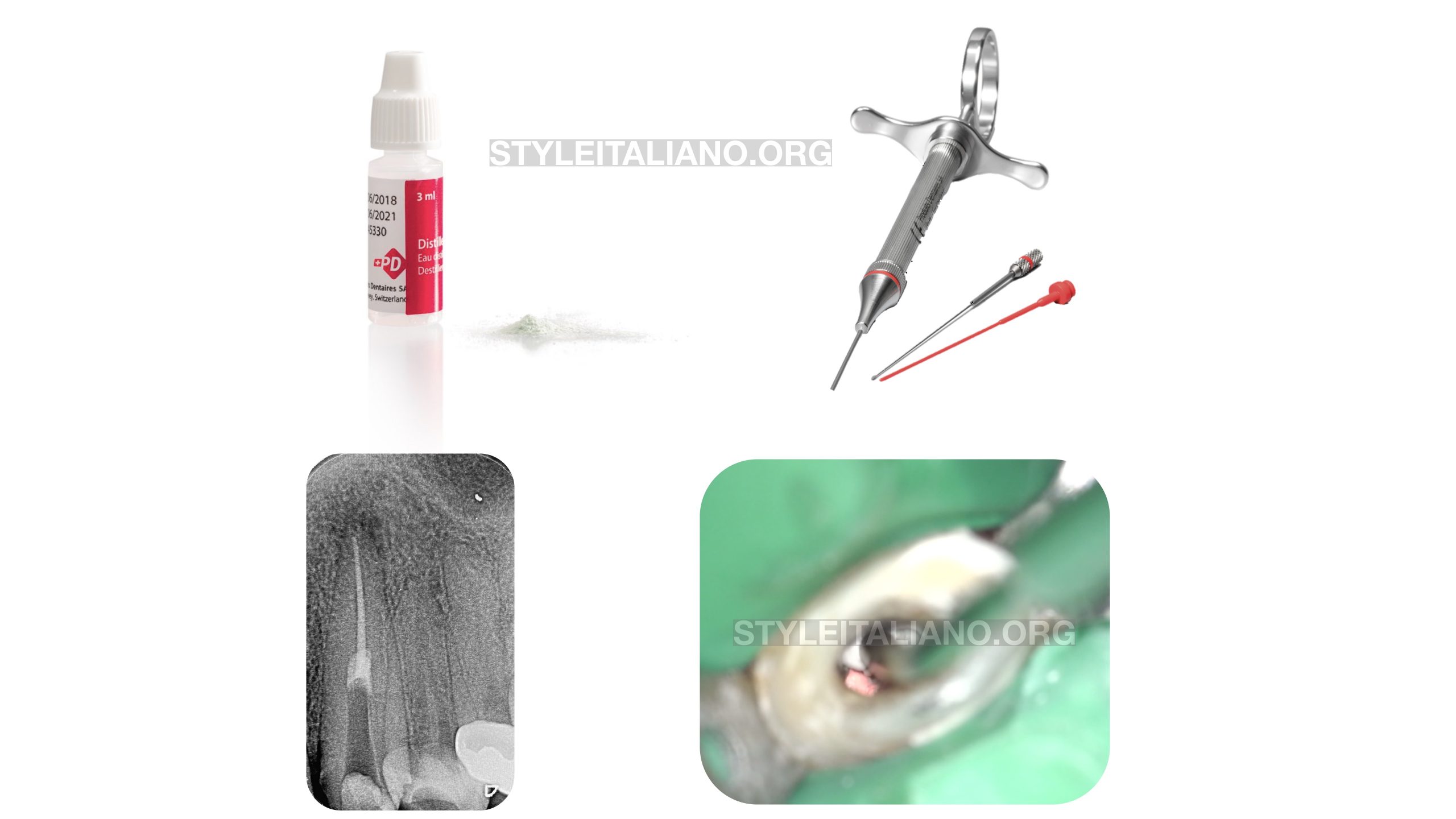
Fig. 3
Canal space was blocked with a gutta percha cone at the level of entrance and then the perforation was repaired with MTA White using MAP ONE gun both from Produits Dentaires SA (1800 Vevey, Switzerland)
After a wet cotton pellet was introduced in contact with the repair material for MTA setting for 72h.
Cleaning Of MAP One Gun immediately after use to prevent blockage
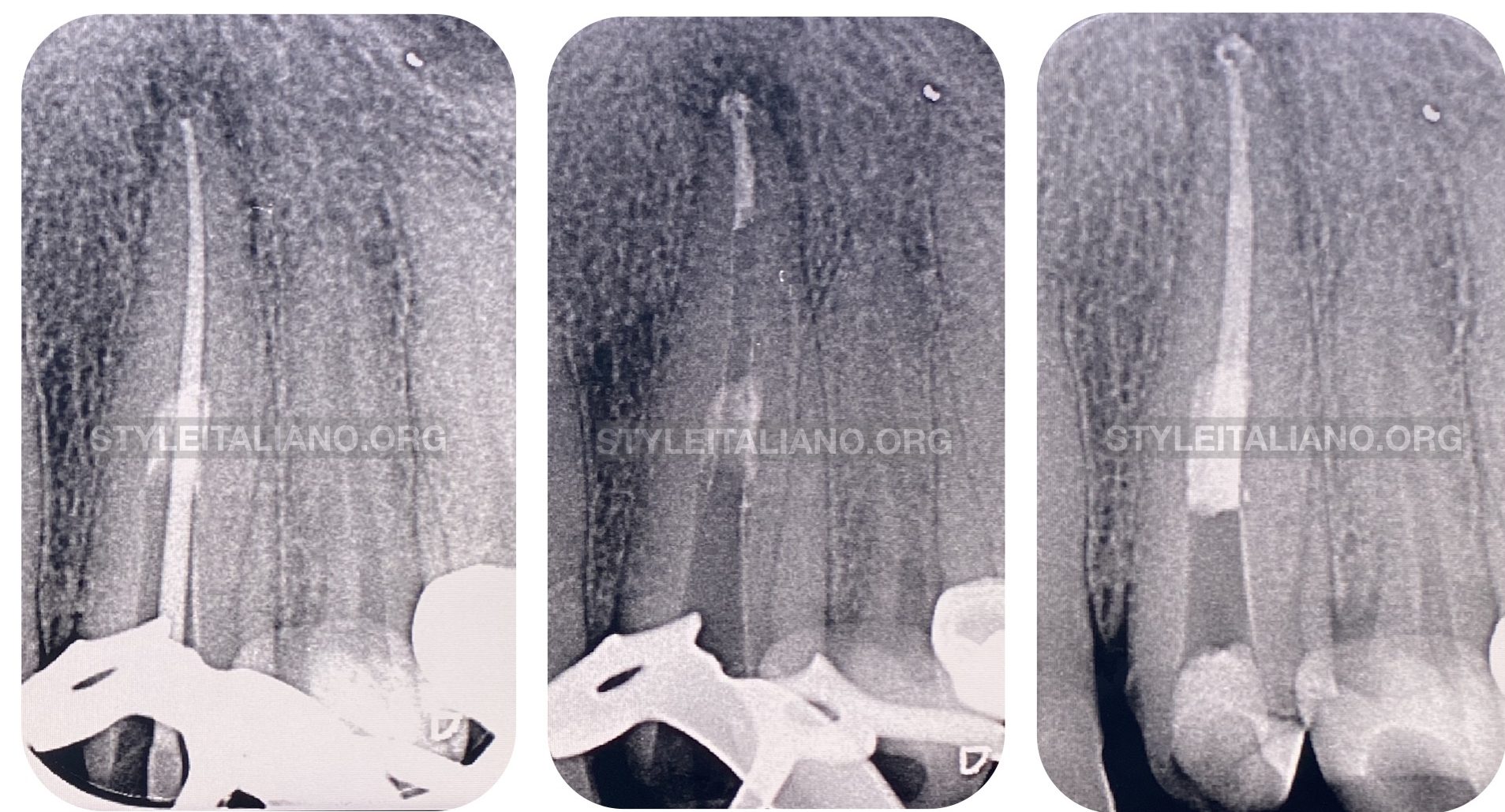
Fig. 4
On the third appointment the patient was without symptoms the final obturation was performed successfully after checking the MTA setting and regaining access to the canal through the repair material.
See the whole case
Conclusions
Proper tools such as Magnification, Ultrasonics and CBCT imaging should always be used while retreating difficult access in single rooted teeth.
Root canal Perforation are sometimes very deep far from the bone crest. In this case report, the site of the perforation was 10 millimeters below the crest; the small area of communication between the external surface of the root and the alveolar bone made the prognosis positive.
The ability of the clinician to visualize clean and seal such perforation is mandatory for achieving long term succes.
Bibliography
Fuss Z, Trope M (1996). Root perforations: classification and treatment choices based on prognostic factors. Endodontic Dental Traumatology Journal 12, 255-64.
Krupp C, Bargholz C, Brüsehaber M, Hülsmann M (2013). Treatment Outcome after Repair of Root Perforations with Mineral Trioxide Aggregate: A Retrospective Evaluation of 90 Teeth.. Journal of Endodontics 39, 1364-8
Stephane Kerner and François Bronnec(2015). Conservative Treatment of a Large Facial Midroot Perforation. Case Reports in Dentistry, 2015, 1–8. Fuss Z, Trope M (1996). Root perforations: classification and treatment choices based on prognostic factors. Endodontic Dental Traumatology Journal 12, 255-64.