Management of the apical inflammatory root resorption
04/12/2021
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Apical inflammatory root resorption (AIRR) is one of the challenges that can happen during root canal treatment. Mostly it is associated with apical periodontis, but can occur after traumas, orthodontic treatment, autotransplantation or can be associated with idiopatic factors. One of the most common factors that is present in teeth with AIRR is intracanal infection. This kind of complication can occur in teeth there were previously not treated or during the retreatment procedures. From the clinical point of view we can meet two kind of problems. First of all in some cases of AIRR there is no apical constriction so the working length determination can be challenging. Therefor a proper diagnosis before the treatment should be collected. In this case digital x-ray and cone beam computed tomography should be used. Also in the final stage of the endodontic treatment achieving proper sealing can be very uncertain if the guttapercha will be used.
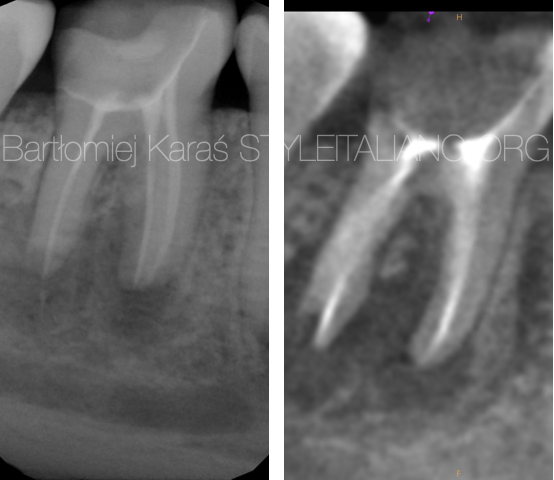
Fig. 1
The diagnosis:
Proper diagnosis of AIRR is mandatory for further management. Most common and important factor for AIRR is intracanal infection which means that either we will have necrotic or previously treated tooth. Second very common factor is periapical lesion which should be present on the x-ray.
The shape of the apex is usually irregular or partially radiolucent.

Fig. 2
Root length determination and preparation.
Usually when the AIRR is present the working lenght determination can be uncertain because apical constriction is violated. In this situation clinican should find the „over apex” or „error” indication on the apex locator and perform the apical stop one millimeter shorter from that indication. Performing control Xray with the files can be useful.
In this kind of situations usually shaping of the apical area sholud be performed up to size 50.04 or even bigger. Often instrumentation with the hand files needs to be performed.
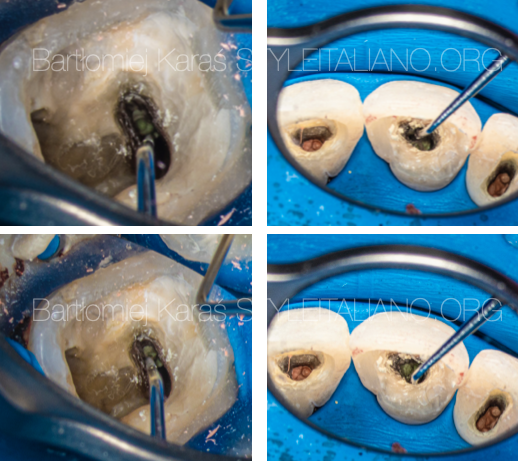
Fig. 3
Obturation
After performing the apical stop procedure and irrigation protocol the apex sholud be sealed with the three calcium silicate based matherial (MTA or Biodentine). We can use Ni-Ti or steel pluggers or biomaterial cariers.
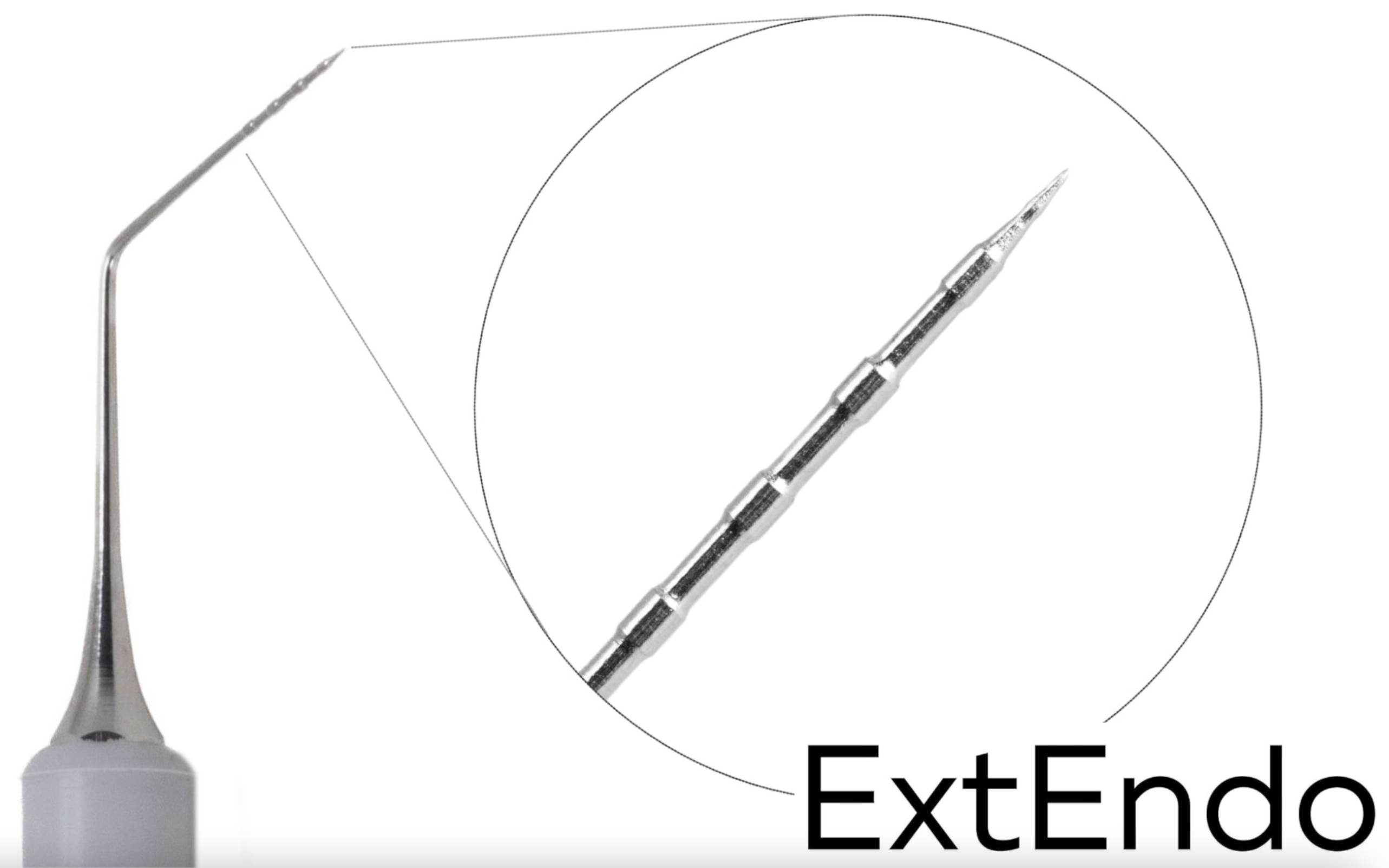
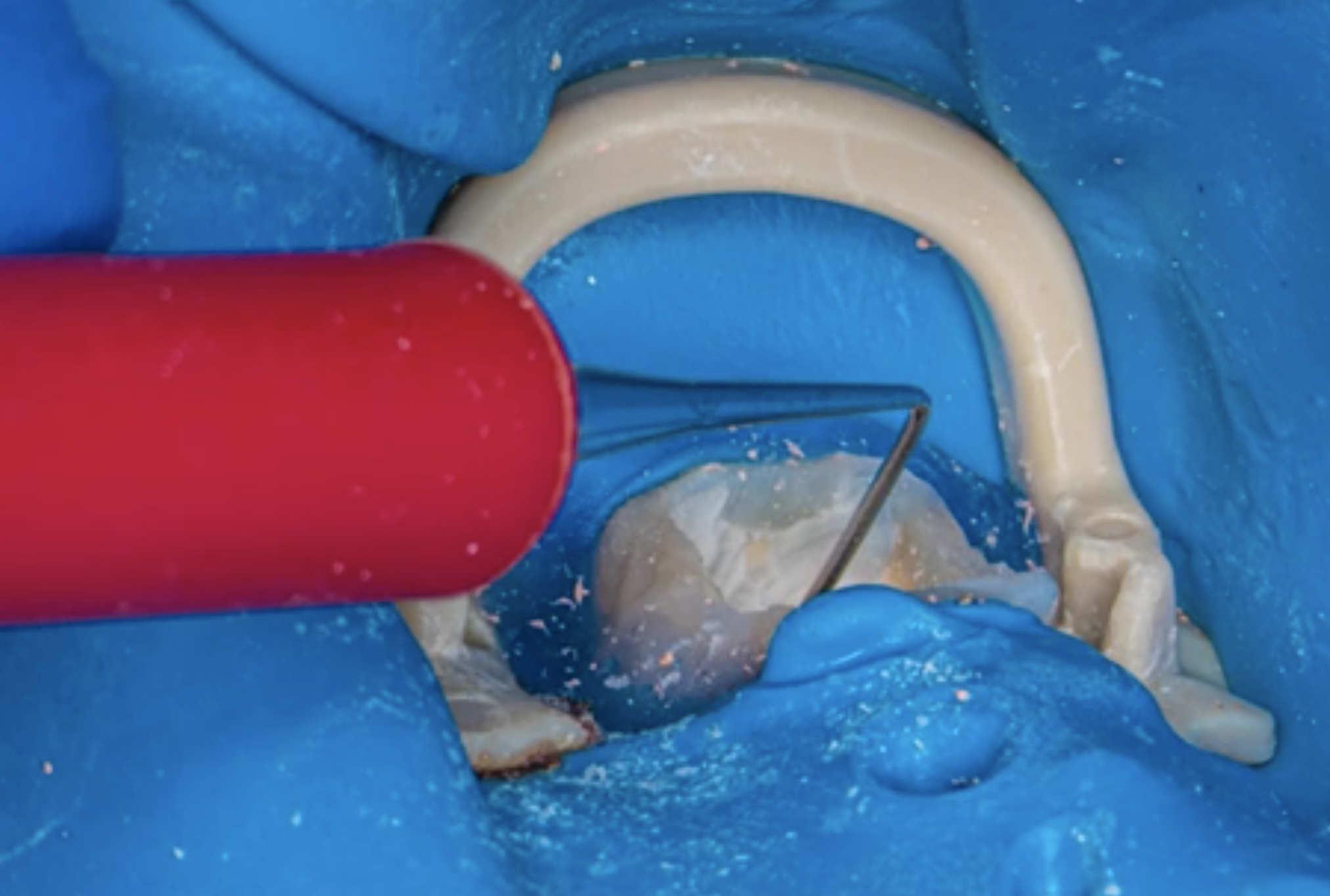
While using the hand plugger it is important to perform proper pressure and also the good visibility is important.
On the images you can see that the visibility of the apical part of the canal while using Prexo-M is very good. Therefore we can see the adaptation of the patherial no matter if it is MTA or Biodentine and adjust the pressure of the condensation.
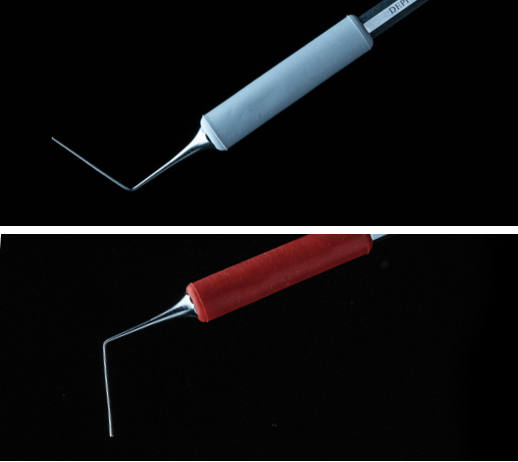
Fig. 4
Prexo-M
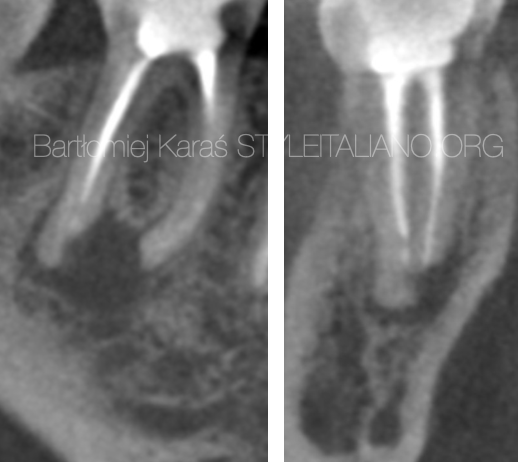
Fig. 5
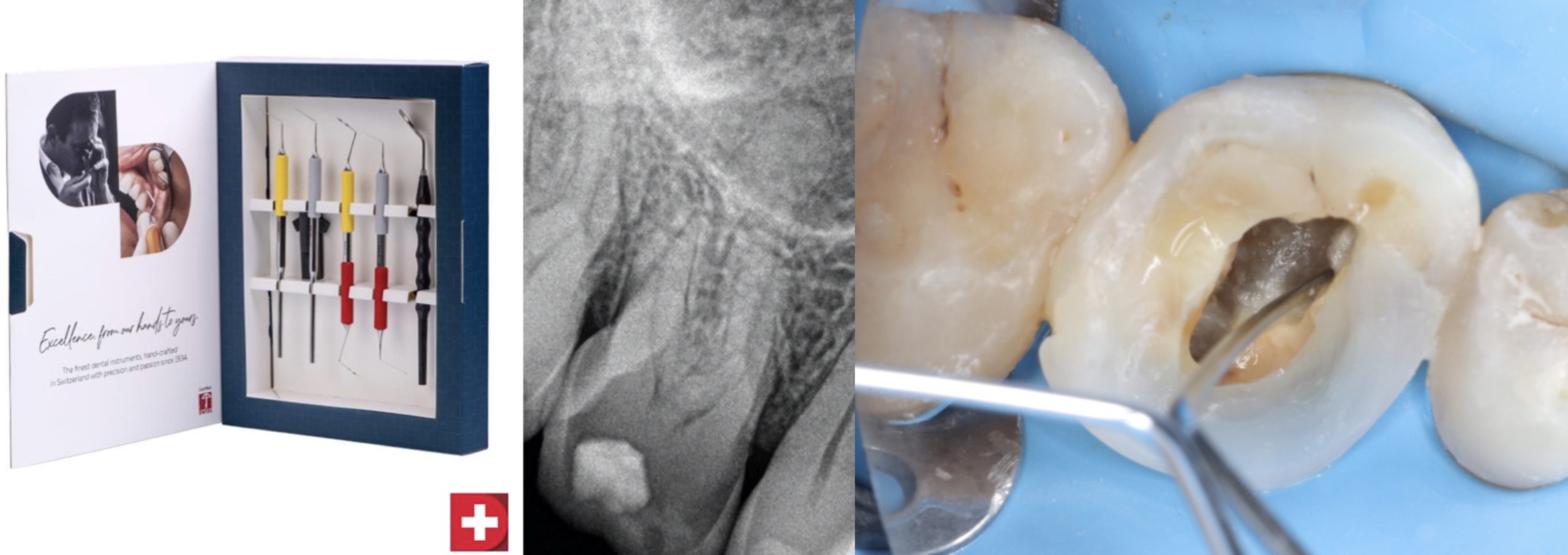
Case:
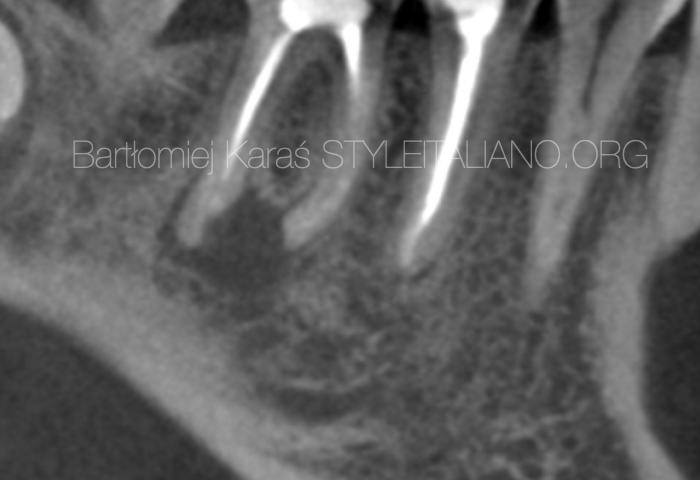
Treatment of the symptomatic, previously treated first mandibular moalar. Cbct examination revealed periapical lesion and AIIR in the distal root.
The treatment of choice was NSRCRT with the TriCalcium silicate based matherial filling in the distal root.
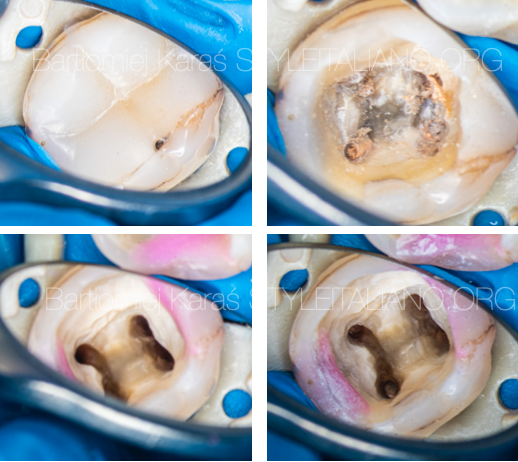
Fig. 6
During the single session appointment all procedures of the retreatment were performed. The old composite restoration was removed, chamber was sealed with flowable color composite. Old filling matherial was removed with rotary files. Irrigation protocol was performed with sodium hypo, citric acid and ultrasonic activation.

Fig. 7
Apex of the distal root was sealed with MTA material. Mesial canals and the medial part of the distal root were obturated with warm guttapercha. After the control xrays fiber post were placed.
Conclusions
Apical Inflammatory Root Resorption can be a challenge for the clinicians. For the proper diagnosis we should use digital x-rays and CBCT if available. During the preparation stage we need to remember about proper working lenght determination and creating the apical stop for proper obturation. During the obturation phase calcium silicate based material should be used. Also using a proper hand plugger that will allow us to perform enough pressure for condensation of the material and let us have a proper vision in the canal will be helpful.
Bibliography
1. Andreasen JO, Andreasen FM. Essentials of traumatic injuries to the teeth. 2nd ed. Copenhagen: Munksgaard, 2001:188.
2. Tronstad L. Root resorption. Etiology, terminology and clinical manifestations. Endod Dent Traumatol 1988;4:241–245.
3. Nance RS, Tyndall D, Levin LG, Trope M. Diagnosis of external root resorption using TACT (tuned-aperture computed tomography). Endod Dent Traumatol 2000;16:24–28.
4. Pierce A. Pathophysiological and therapeutic aspects of dentoalveolar resorption. Aust Dent J 1989;34:437–448.
5. Ne RF, Witherspoon DE, Gutmann JL. Tooth resorption. Quintessence Int 1999:9–25.
6. Gunraj M. Dental root resorption. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1999;88:647–653.
7. Andreasen FM, Sewerin I, Mandel U, Andreasen JO. Radiographic assessment of simulated root resorption cavities. Endod Dent Traumatol 1987;3:21–27
8. Durack C, Patel S, Davies J, Wilson R, Mannocci F. Diagnostic accuracy of small volume cone beam computed tomography and intraoral periapical radiography for the detection of simulated external inflammatory root resorption. Int Endod J. 2011 Feb;44(2):136-47. doi: 10.1111/j.1365-2591.2010.01819.x. Epub 2010 Nov 17. PMID: 21083575.