Management of Maxillary Central Incisor with Extreme Calcific Metamorphosis
20/09/2021
José Conde Pais
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Pulp canal calcification is characterized by the deposition of calcified tissue along the canal walls. As a result, the root canal space can become partially or completely obliterated. It is considered a normal physiological process occurring with ageing, and a defensive response to normal wear. This response, however, can be accelerated considerably in the case of dental trauma, autotransplantation, and orthodontic therapy and in these instances quickly leads to partial or total pulp canal obliteration. These teeth provide an endodontic treatment challenge; the critical management decision being whether to treat these teeth endodontically immediately upon detection of the pulpal obliteration or to wait until symptoms or signs of pulp and or periapical disease occur. This article describes endodontic management of a traumatized maxillary incisor with calcific metamorphosis.

Fig. 1
A 25-year-old female patient presented in our private endodontic office for evaluation of tooth 11, which had a dental trauma 7 years before.
Her medical history was unremarkable and radiographic examination revealed a calcified canal and previously initiated root canal treatment.
Clinical examination :
- Negative vitality
- Positive percussion
- Positive palpation
The diagnosis was apical periodontitis, after discussing treatment options, we decided on an endodontic treatment. The patient was informed of the pros and cons of the treatment and informed consent was obtained.
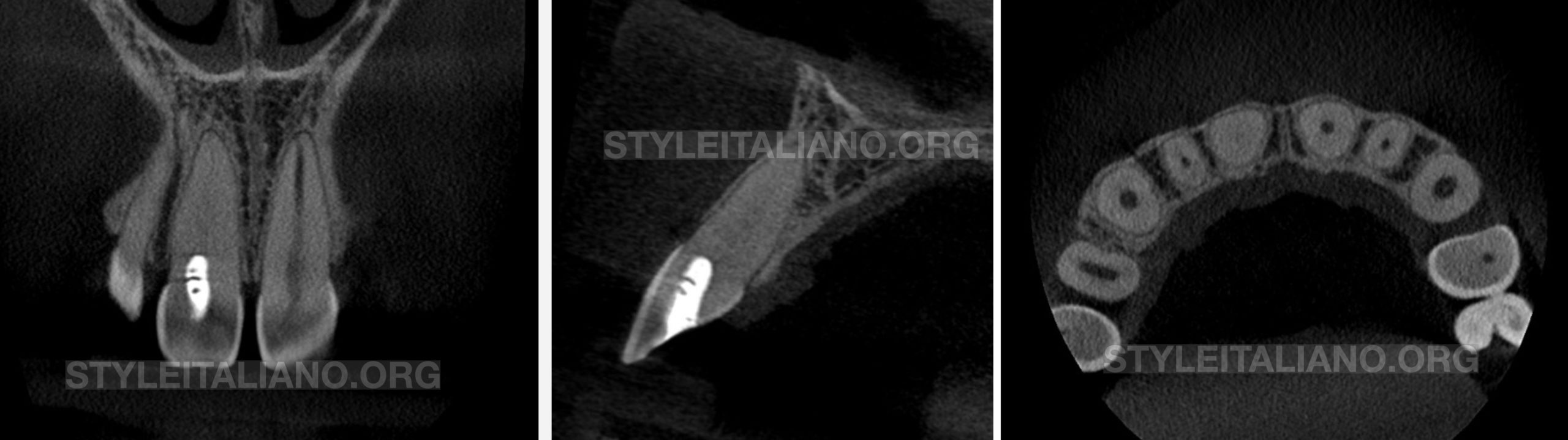
Fig. 2
CBCT Slides

Fig. 3
We made the access cavity with an EndoAcces bur and redefined it with ultrasonic tips
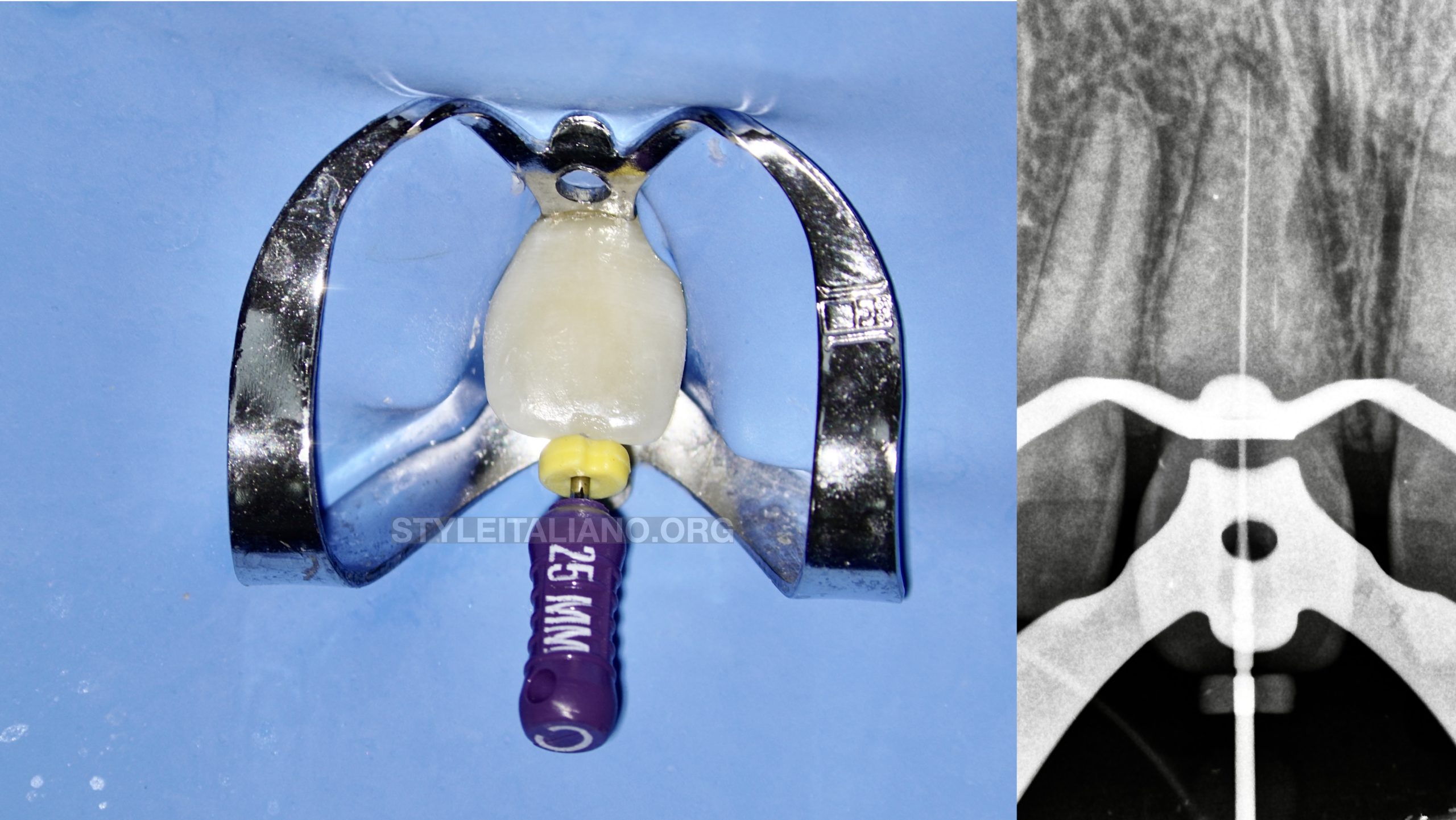
Fig. 4
Glide Path with manual files C + 06 # 08 # 10 #
Scouting Video
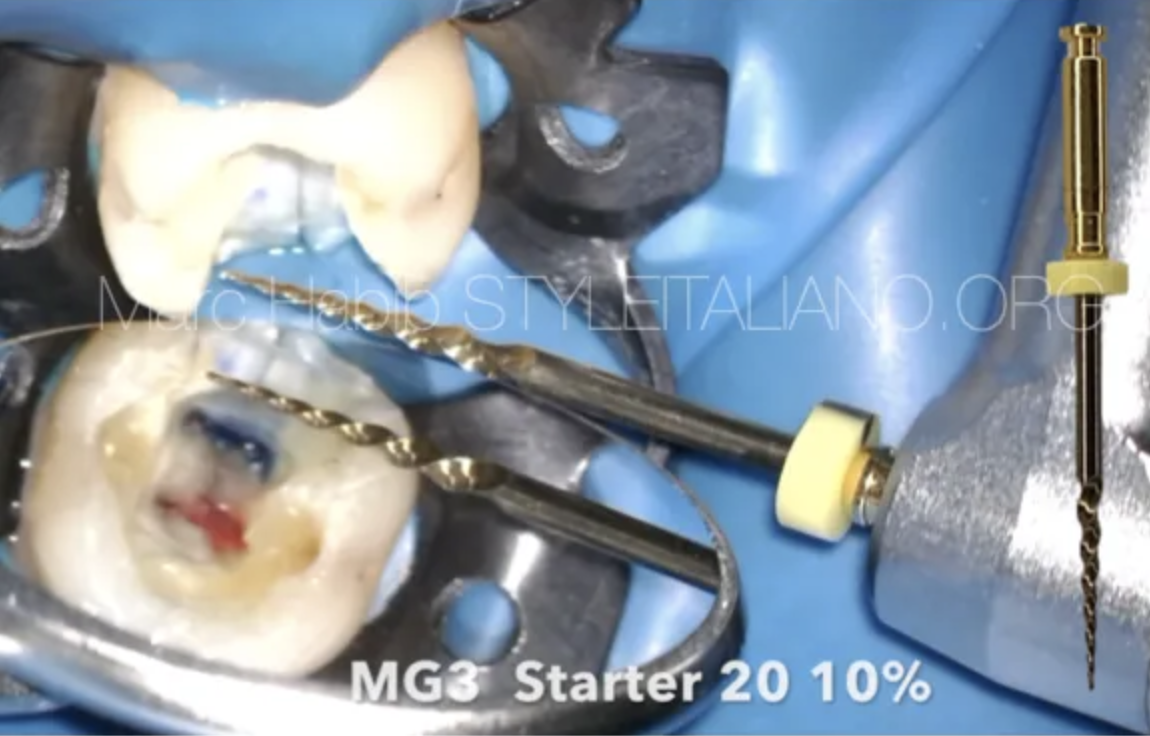
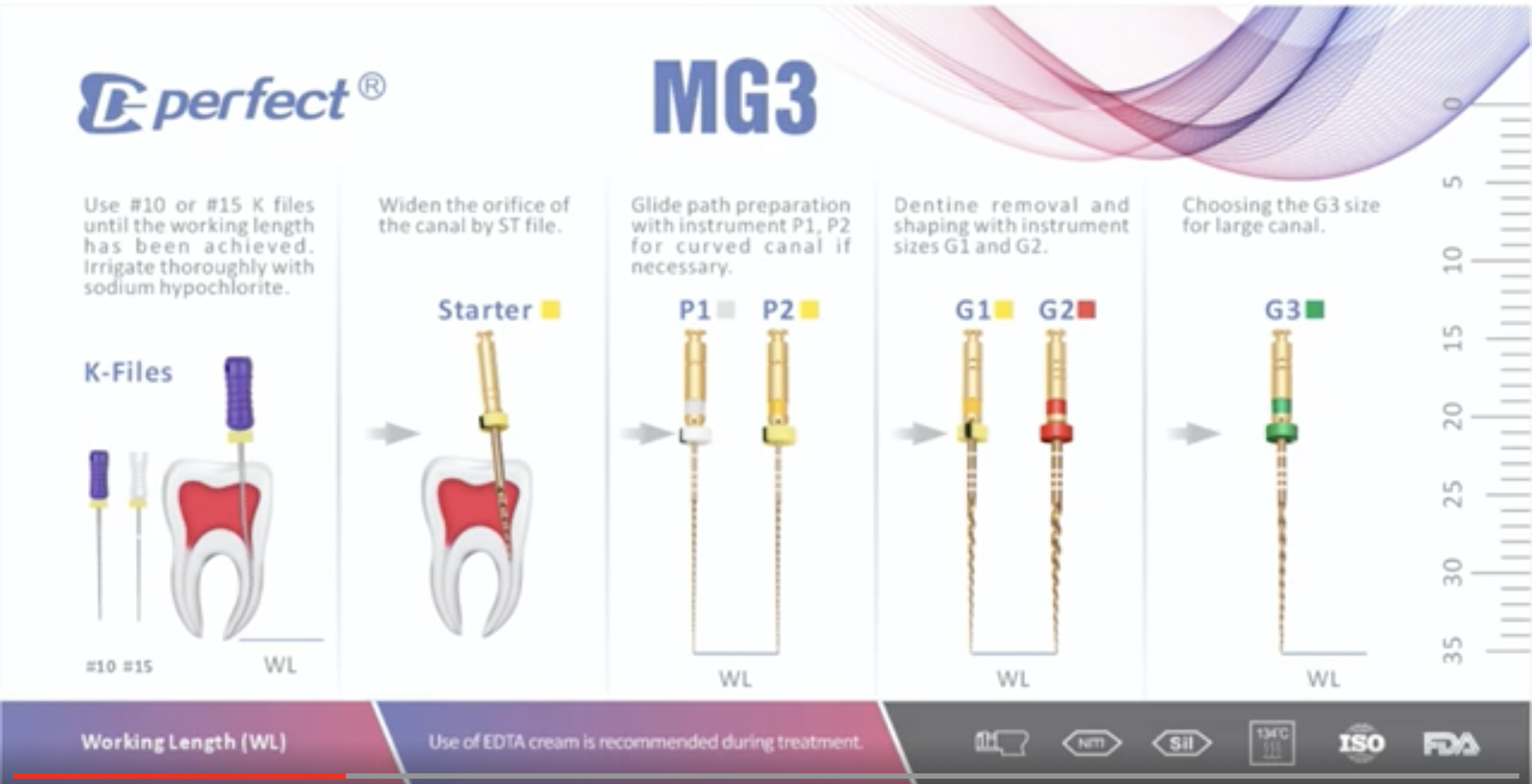
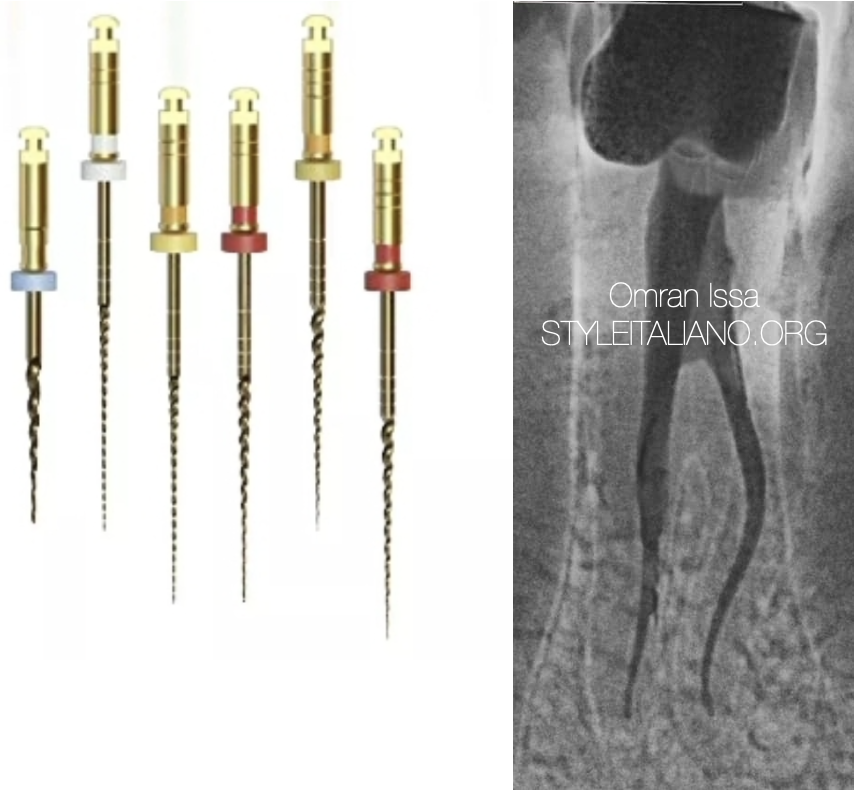
Preflaring was performed using Starter, P1 and P2 (MG3 files kit )(Shenzhen Perfect Medical Instruments Co)
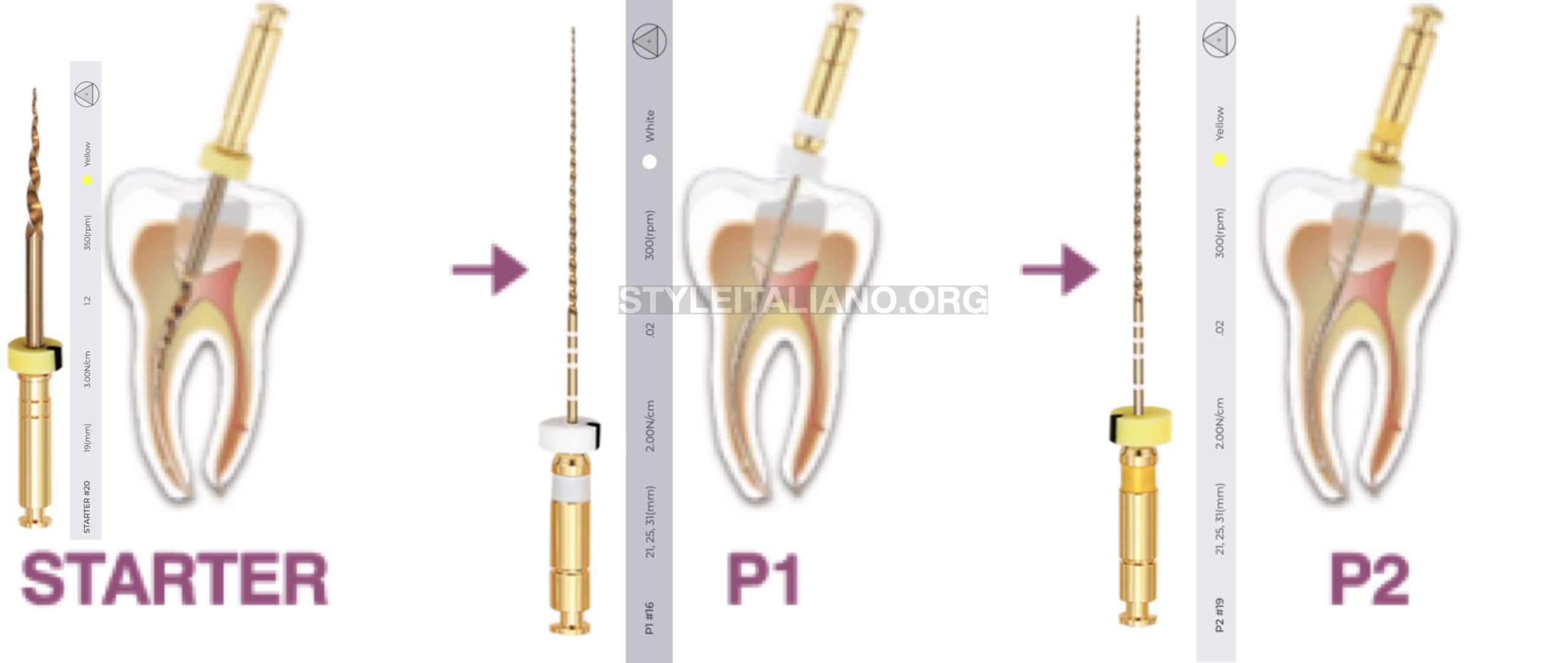
Fig. 5
Preflaring sequence
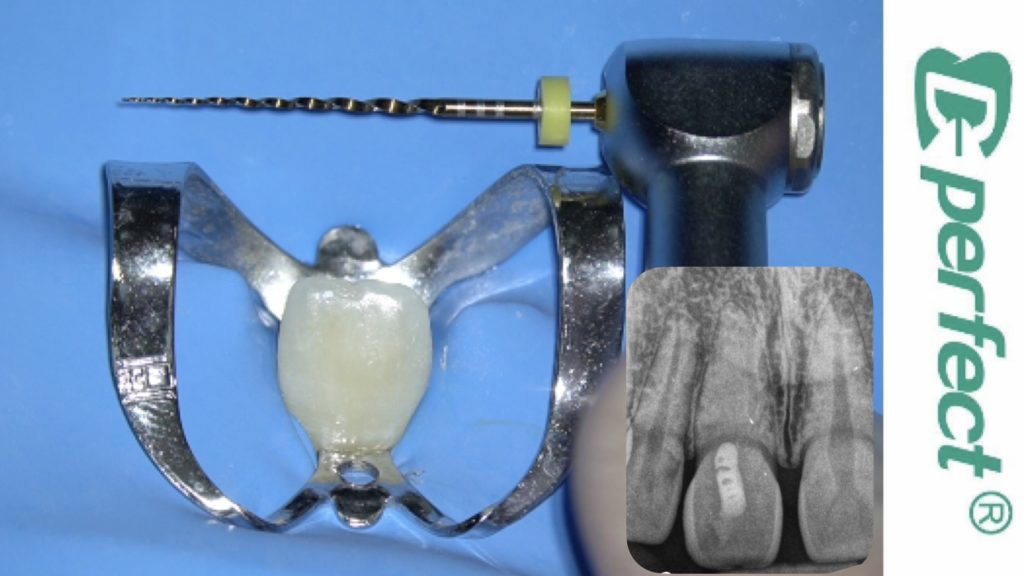
Shaping was performed using G1 and G2 (MG3 files kit )(Shenzhen Perfect Medical Instruments Co)
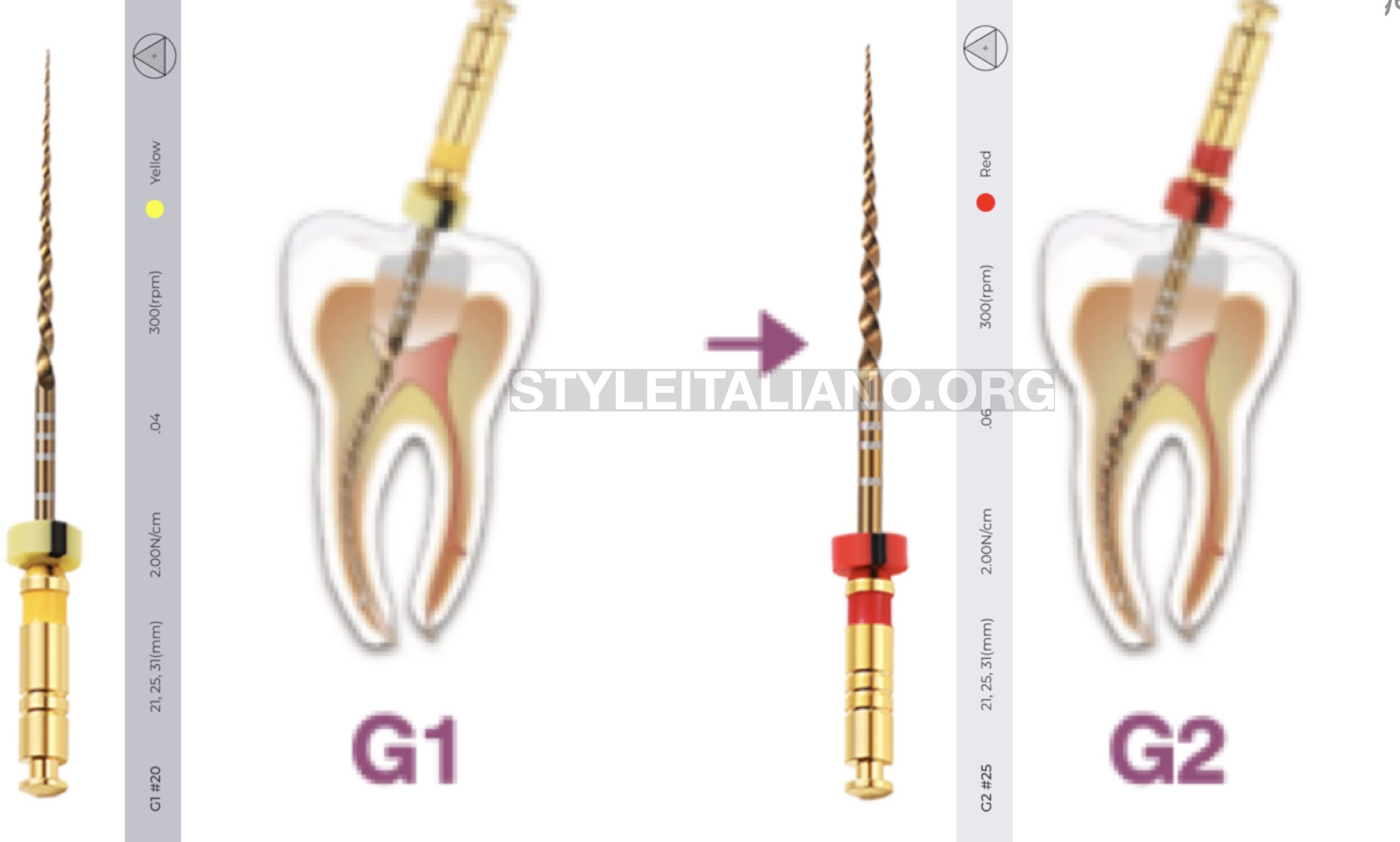
Fig. 6
Shaping Protocol
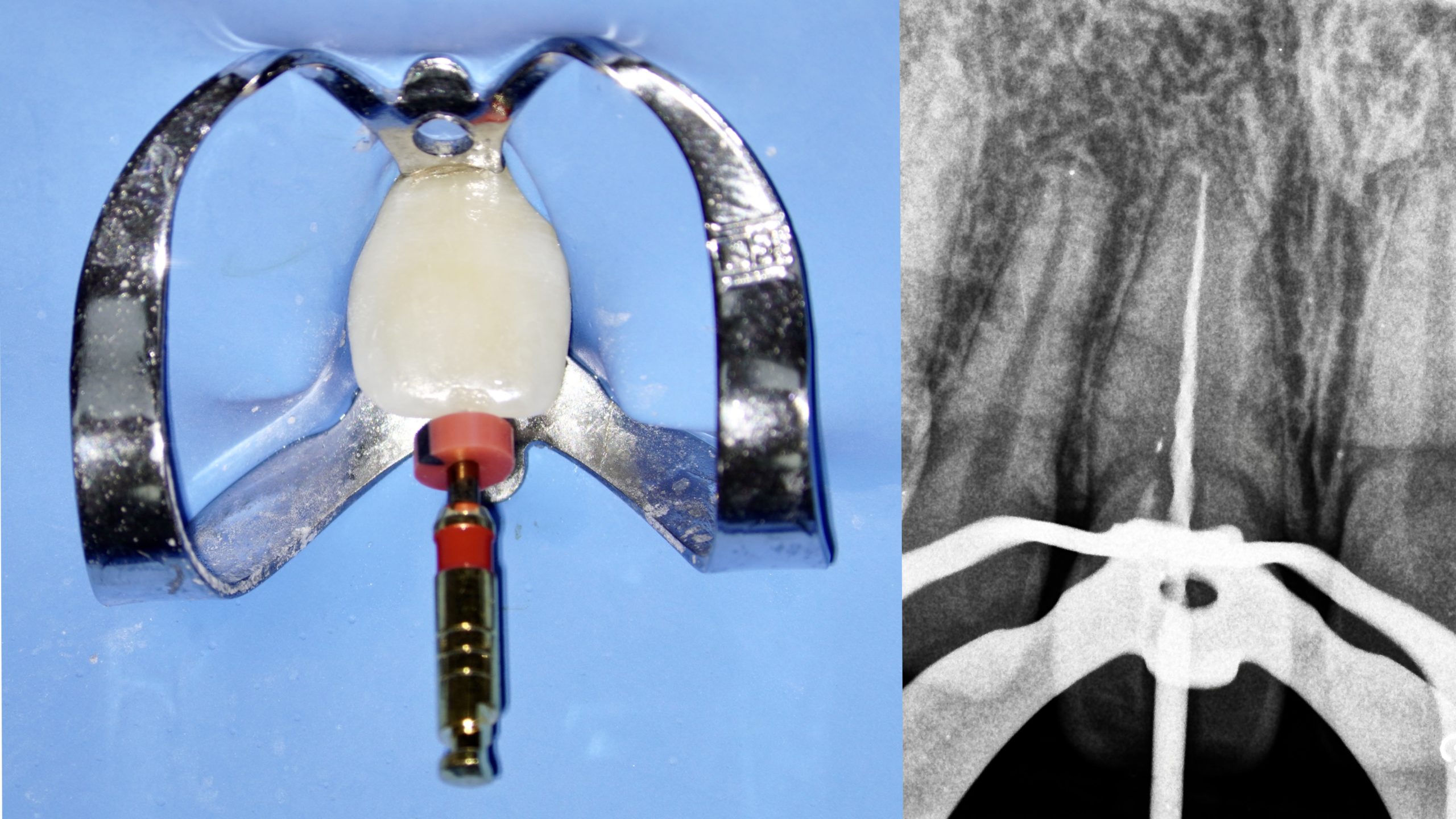
Fig. 7
Master Apical File 25#
Irrigation
Obturation with continuous wave technique

Fig. 8
Apical Seal and Backfill

Fig. 9
Final Rx
Full case video
Conclusions
Managing a calcified tooth is a great challenge for an experienced clinicians. The use of a microscope and files with good cutting capacity are essential to successfully solve these types of cases.
Bibliography
Andreasen FM, Zhijie Y, Thomsen BL, Andersen PK. Occurrence of pulp canal obliteration after luxation injuries in the permanent dentition. Endod Dent Traumatol. 1987 Jun;3(3):103-15. doi: 10.1111/j.1600-9657.1987.tb00611.x. PMID: 3476298.
McCabe PS, Dummer PM. Pulp canal obliteration: an endodontic diagnosis and treatment challenge. Int Endod J. 2012 Feb;45(2):177-97. doi: 10.1111/j.1365-2591.2011.01963.x. Epub 2011 Oct 17. PMID: 21999441.