Endodontic management of a maxillary molar with confluencing canals using MG3 files
25/08/2022
Viresh Chopra
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
A thorough knowledge of the root canal anatomy is a basic prerequisite for successful completion of the endodontic treatment. Awareness and understanding of the presence of unusual external and internal root canal morphology contributes to the successful outcome of the root canal treatment. Maxillary molars are known to have an additional canal (MB2) in the mesio buccal root. The occurrence of second mesiobuccal canal is a common variation. Weine (2004) stated that frequent failure of endodontic treatment in maxillary first permanent molar teeth was likely due to the failure to locate and fill the second mesiobuccal canal. Wolcott et al, have shown that failure to find and treat existing MB2 canal will decrease the long-term prognosis.

Fig. 1
Description of the case
Patient information
- ïAge:26-year old
- ïGender: Female
- ïMedical history: non-contributory
- ïIdentification: Left maxillary first molar (Tooth 26)
- ïDental history :
Chief complaint: I am having severe pain and sensitivity to hot and cold. Pain only relieves for some time with medicines.
- Clinical examination findings: The tooth 26 is severely tender to percussion and had a mesio-occlusal deep carious lesion.
Preoperative radiological assessment:
The periapical radiograph revealed deep mesio-occlusal carious lesion irt 26.
The pulp chamber shows signs of calcifications. (Fig 1).
- Diagnosis (pulpal and periapical):
- Irreversible Pulpitis with Symptomatic apical periodontitis.

Fig. 2
Root canal treatment protocol followed:
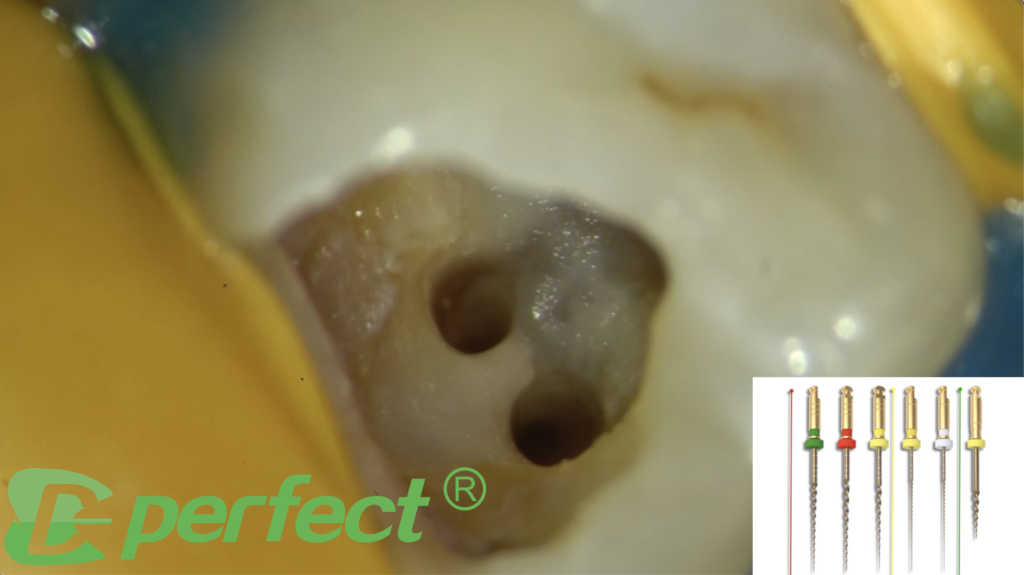
Buccal infiltration anesthesia was administered, the tooth was isolated with rubber dam isolation and the tooth was seen under the microscope preoperatively. Carious excavation was performed followed by endodontic access cavity preparation with Endo access burs. Four orifices were located using Endodontic explorer. The orifices were widened using orifice opener which is 20/.10 file in the MG3 kit (Fig 2).
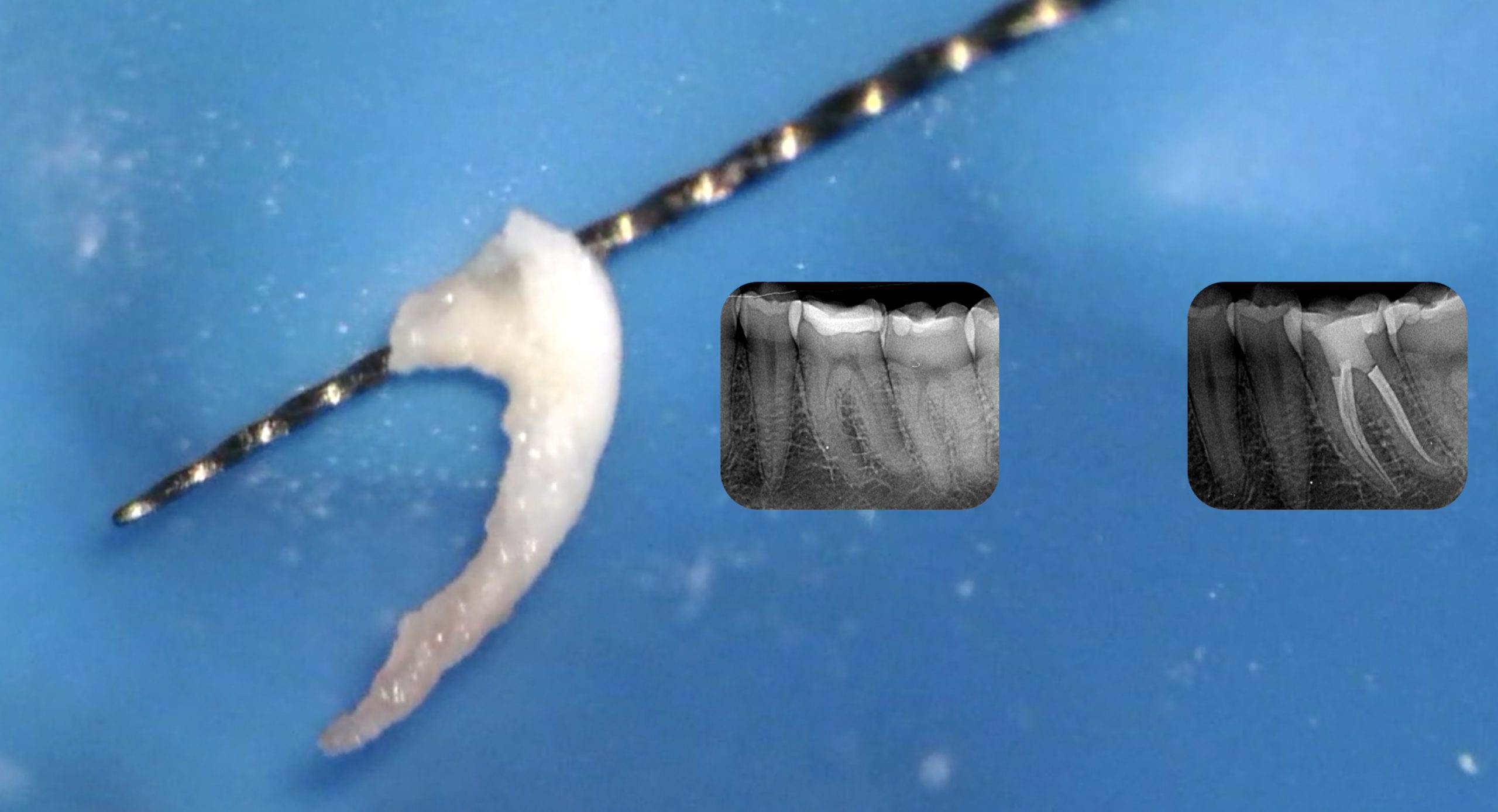
The mesiobuccal canals (MB1 and MB2) were confluencing which can be clearly seen during master cone trial in (video - -). The canals were then cleaned and shaped with using the MG3 files in the following sequence
· Initial glide path using P1 and P2 files(video 1).
· Final shaping using G1 and G2 files (video 2).
Profuse irrigation was performed in between every instrument using 3% sodium hypochlorite for adequate disinfection. The canals were finally shaped using G2 file as the master apical file (video 2). Master cone fit was checked clinically as well as radiographically and the canals were prepared for obturation .
The mesiobuccal canals (MB1 and MB2) were confluencing which can be clearly seen during master cone trial in (video 3).
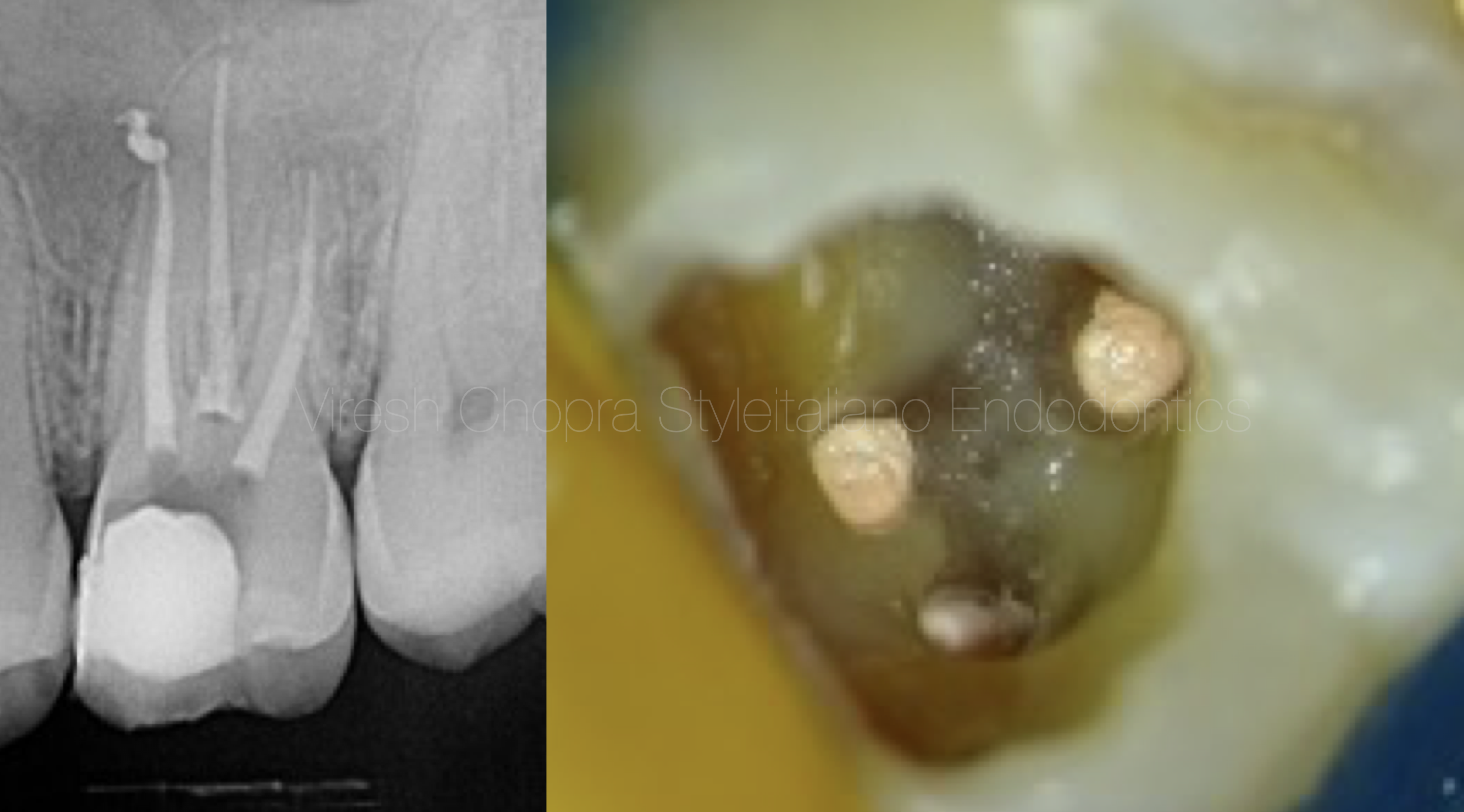
Fig. 3
Master cone fit was checked clinically as well as radiographically and the canals were prepared for obturation. Obturation was performed using Calcium silicate sealer along with the Gutta percha cones (Fig 3) (video 4). The obturation was verified radiographically (Fig 4)
Obturation video
Conclusions
In order to achieve success in endodontic treatment, root canal system needs to be thoroughly cleaned, shaped, disinfected and a 3-dimensional obturation of the root canal system should be achieved.
Inability to locate all the canals will lead to inadequate cleaning and shaping leaving residual microorganisms leading to failure of the initial root canal treatment. Significance of confluencing canals should be understood in order to clean and disinfect the canals appropriately.
- Learning Objectives: The reader should be able to understand:
- The importance of magnification in Endodontics.
- The significance of proper interpretation of the preoperative radiograph.
- The significance of a selection of correct rotary file system..
- The importance to use of efficient tools to make endodontic treatment easier and less messy.
- The importance of copious irrigation in endodontics.
- The need to plan/modify the treatment steps as per the clinical findings during the procedure (like in this case: the obturation was done by cutting gp at orifice and not WVC since BC sealer was used).
- How to decide clinically, which instrument to be used for a particular step during an endodontic treatment.
- The concepts of understanding the prognosis of the tooth and giving a try to save the tooth instead of straight away extracting it.
Bibliography
Schryvers A, Govaerts D, Politis C, Lambrechts P. Endodontic management of a maxillary first molar with two palatal roots: A case report. Australian Endodontic Journal. 2019 Dec;45(3):420-5.
Raju RC, Sathe N, Morisetty PK, Veeramachaneni C. Endodontic management of a maxillary first molar with unusual location of second mesio buccal orifice. Journal of conservative dentistry: JCD. 2010 Jul;13(3):162.
Mirdha N, Ponnappa KC. Endodontic Management of Maxillary first molar with 2 palatal and 3 buccal canals and associated with multiple space infection. J Int Oral Health. 2011 Jun 1;3:31-6.