Coronal Preflaring
01/07/2016
Massimo Giovarruscio
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
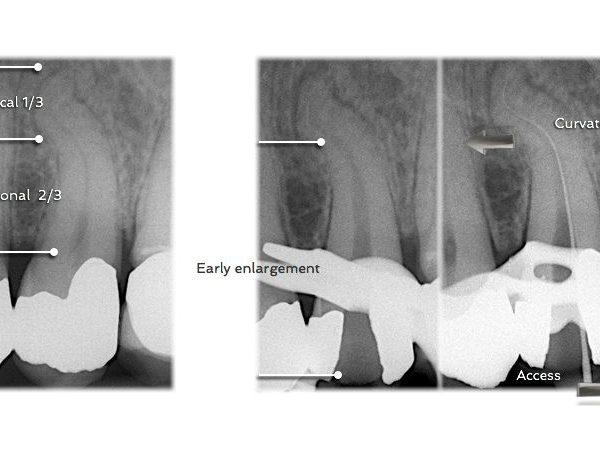
After access cavity, Preflaring, Canal Scouting and Glyde Path are the first phases of canal instrumentation and it has also been noted that, during these phases, the clinician might more frequently encounter procedural difficulties. These problems include instrument fracture, ledge formation, canal zipping or canal straightening, strip perforation, apical perforation, elbow formation and apical blockage. All of these errors can lead to incomplete debridement of the root canal system and contribute to decreased success rates of endodontic therapy.
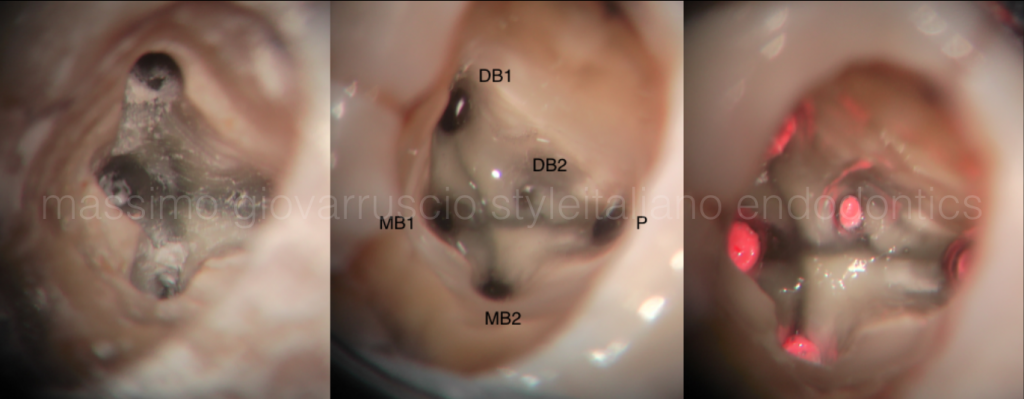
Fig. 1
Much has been written in the field of endodontics about the importance of coronal access. Coronal access needs to be large enough to allow entry into all canals, while preserving tooth structure for future restoration. The access cavity should be as small as practical.

Fig. 2
The principle of straight-line access into the pulp chamber is generally accepted, straight-line access into the chamber will not ensure straight line access into canals as a triangle of dentin will be present at the orifice, which continues for a few millimeters below the pulpal floor. This dentine triangle needs to be removed and this step of ensuring straight line access into the canal should be accomplished for every tooth even if the pre-operative anatomy seems straightforward.
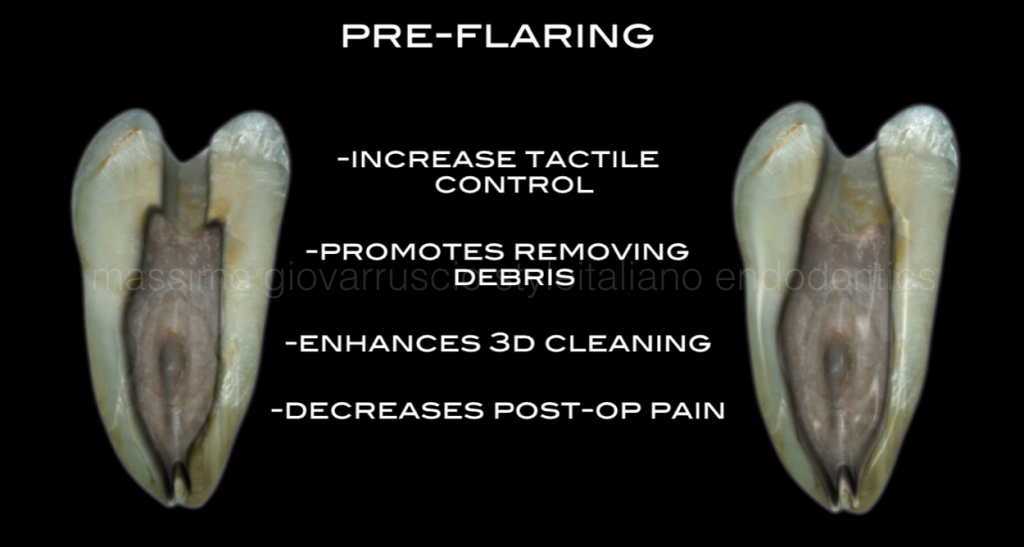
Fig. 3
The principle of straight-line access into the pulp chamber is generally accepted, straight-line access into the chamber will not ensure straight line access into canals as a triangle of dentin will be present at the orifice, which continues for a few millimeters below the pulpal floor. This dentine triangle needs to be removed and this step of ensuring straight line access into the canal should be accomplished for every tooth even if the pre-operative anatomy seems straightforward.
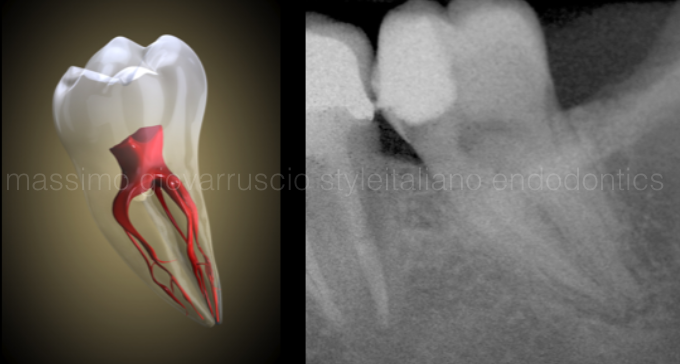
Fig. 4
Pre-flaring gives the clinician better tactile control when directing small precurved negotiating files into the delicate apical one-third microanatomy. Early coronal two- thirds enlargement removes restrictive dentin and reduces significant pressure from the more coronal cutting flutes of any file type.
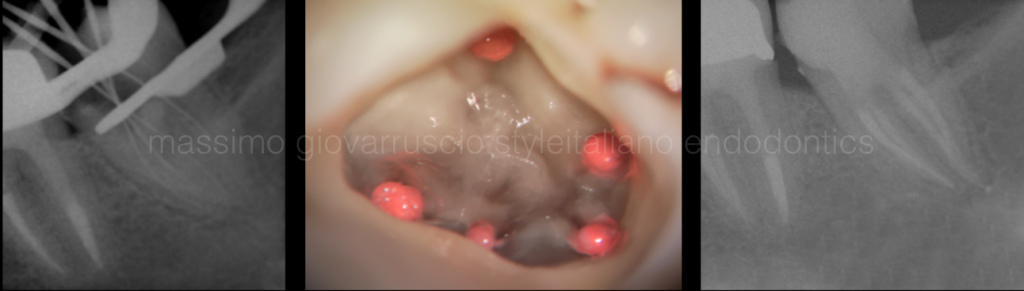
Fig. 5
Scouting and shaping step become more easy and predictable when the pre enlargement has been performed properly also in the complex root canal system like this second lower molar.
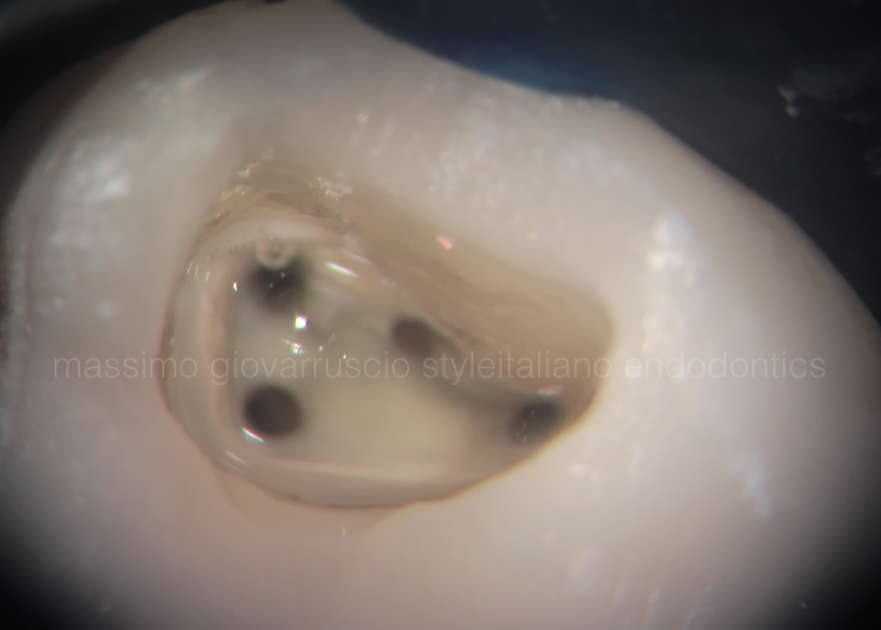
Fig. 6
Preflaring canals hold a greater and more effective volume of irrigant which serves to enhance cleaning. Narrow, more restrictive preparations are dangerous as files work in virtually dry canals. A preflared canal exhibits shape and holds a greater volume of warm irrigant which accelerates the apical and lateral digestion of pulp.
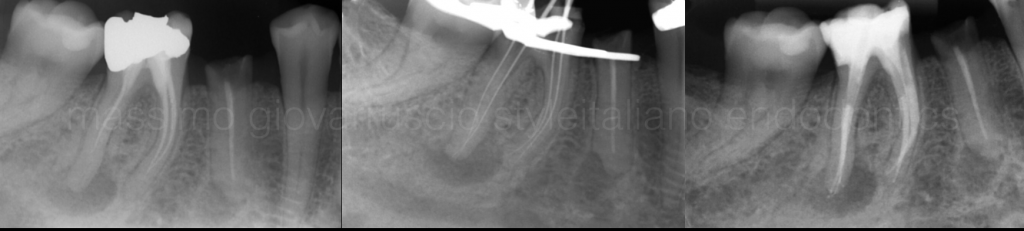
Fig. 7
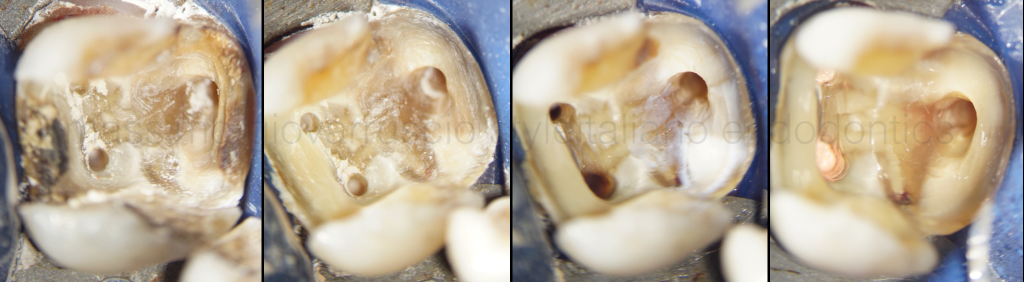
Fig. 8
Preflaring procedures decrease post-treatment problems as the bulk of the pulp and, if present, bacteria and related irritants have been removed. Passing files through a cleaned pre-enlarged preparation equates to less debris inadvertently inoculated periapically. Passing files through underprepared canals coronally pushes more irritants periapically and generates more post-operative exacerbations.

Fig. 9
Other options for removal of the dentin triangle would include Gates Glidden drills, orifice openers or a series of larger hand files. Gates Glidden drills have the potential to cut to the furcation side of the canal. Over enlargement may result in the thinning of the root wall or a root perforation.
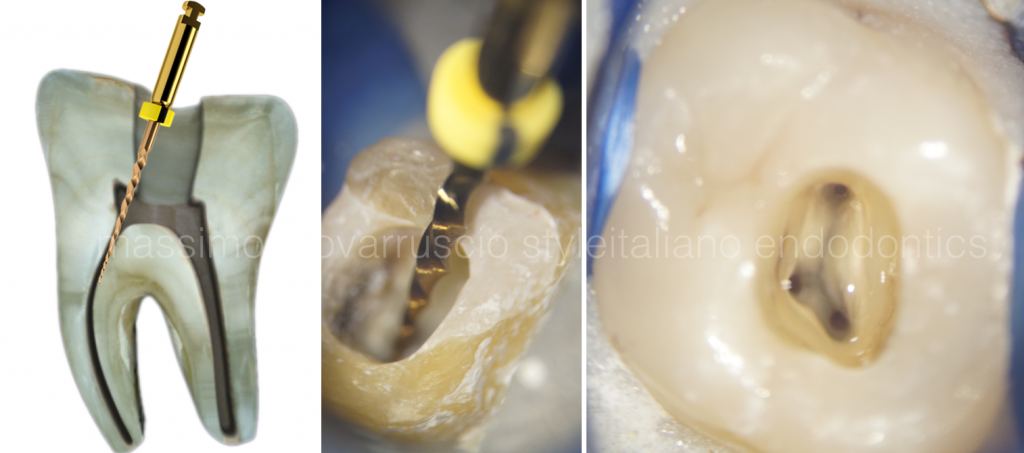
Fig. 10
Hand files will require more time and are stiff, thereby increasing the risk of altering the natural canal anatomy, but hand instruments can be effective at this level of the canal. Nowadays a Ni-Ti rotary files can be used safely and efficiently.

Fig. 11
Preflaring procedures generally improve diagnostics. A pre-enlarged canal passively accepts a larger file into the apical one-third where its terminal extent is easier to visualize radiographically. Electronic apex locators are more accurate when utilized in pre-enlarged canals as instruments are more likely to snug into dentin towards their terminal extents. When the clinician does establish a working length, it will be more accurate as it occurs after a more direct path to the terminus has been established.

Fig. 12
A Triangle of Dentine if not removed properly can increase the torsional stress on hands files during working length measurement.

Fig. 13
The Green Area could be considered a safety area where any rotary instrument is able to work with less torsional stress due to the straight line access.

Fig. 14
Conclusions
The purpose of this paper was to describe a preflaring technique that is designed to optimize the apical part of root canal preparation. Cervical or early preflaring plays a vital role in reducing the discrepancy between initial apical file diameter and apical canal diameter. It also has frequently been reported that manual or mechanical pre-flaring is very important to reduce the incidence of instrument breakage.
Further article will describe how to create a reproducible Glide Path that is a pathway with smooth canal walls along which the NiTi instruments can easily slip and slide to reach the working length.
Bibliography
- Schilder H. Cleaning and shaping the root canal, Dent Clin North Am 18:2, 269-296, April 1974.
- Ruddle CJ. Ch. 8, Cleaning and shaping root canal systems. In Pathways of the Pulp, 8th ed., Cohen S, Burns RC, eds. St. Louis: Mosby, pp. 231-291, 2002.
- Weine FS: The use of non-ISO tapered instruments for canal flaring, Compend Contin Educ Dent 17:651-663, 1996.
- Machtou P, Ruddle CJ. Advancements in the design of endodontic instruments for root canal preparation. Alpha Omegan. 2004;97:8-15.
- Berutti E, Cantatore G, Castellucci A. Use of nickel-titanium rotary PathFile to create the glide path: comparison with manual preflaring in simulated root canals. J Endod. 2009;35:408-412.
- Glosson CR, Haller RH, Dove SB, del Rio CE. A comparison of root canal preparations using NiTi hand, NiTi-driven, and K-flex endodontic instruments. J Endodon 1995, 21: 146-151.
- Berutti E, Negro AR, Lendini M, Pasqualini D. Influence of Manual Preflaring and Torque on Failure Rate of ProTaper Rotary Instruments. J Endod 2004; 30 (4): 228-230.