

Cervical margin relocation of endodontically treated teeth
24/02/2022
Federico Ceroni
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Adhesive dentistry changed the way we approach the rehabilitation of endodontically treated teeth. Adhesives and composites have permitted more conservative protocols for repairing severely damaged teeth by reducing the invasiveness that was historically involved with the ‘’classic’’ prosthetic approach.
The limit of the adhesive approach lies in our ability to be able to isolate the cavity margin. The use of the rubberdam, the impression for a indirect restoration, the cementation of an overlay become complicated when the cavity margin is subgingival. so how can we manage the most complex cases?
Cervical margin relocation (CMR) was first described by dietschi et al, he suggested to elevate a proximal, slightly sub gingival cervical cavity to a more supra gingival level through the use of an adequate layer of composite.
This method allows us to solve the problems listed above: difficulties during the impression, isolation with rubberdam of the margin of the preparation and the management of the cementation of an indirect restoration. After Dietschi several other articles have been published with the aim of supporting or better describing this restorative approach.
CMR is a minimally invasive alternative to the crown lengthening in some cases, especially useful when we are rehabilitating aesthetic areas that could be altered if lengthening is performed.
But there are two problems with this approach, the adhesion protocol for deep cavities, and the violation of the biological with due to the depth of the carious lesion, these two factors must be carefully analyzed every time we face a cervical margin relocation case.

Fig. 1
A 25 yrs old man came to our office complaining discomfort related to the second upper right premolar.
You can see from the pictures a gingival inflammation affecting the distal papilla of 15, inflammation which also led to the loss of the most coronal portion of the papilla.
The cause is a large cavity that leads to the accumulation of plaque in that area.
Biologically, a distance of 3mm is recommended between the restorative margins and the alveolar crest in order to avoid detrimental effects on neighboring soft and hard periodontal tissue and fortunately in this case the distance was respect so a cervical margin relocation was chosen to restore the tooth.
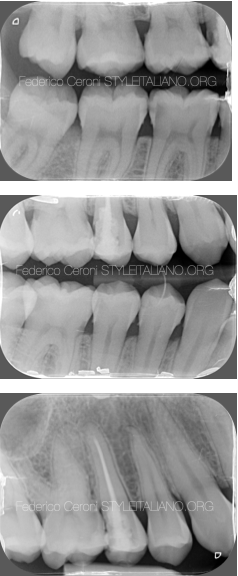
Fig. 2
After the execution of the x-rays we can see the size of the cavity and its subgingival position, in addition there is also an incorrect restoration that has to be replaced and an old endodontic treatment that needs to be redone.
The restoration of endodontically treated premolar teeth presents in general different mechanical and esthetic challenges. Several aspects have to be considered, such as:
Remaining Tooth structure ( Presence of enamel, number of remaining walls, quality of dentin )
Patient age
Functional loads
Esthetic demands
Direct or indirect restorations with or without post placement should be chosen considering all these aspects.
In this particular case I decide to restore the tooth with an indirect restoration without any post, this because the remaining structure was enough to resist at the functional loads.

Fig. 3
After the rubberdam placement the old composite restoration was carefully removed using a cylindrical medium-grain bur and the margins were clean and smoothened using a silicon bur.
Deep cervical margins often leaves only dentin and cementum as the main substrates for adhesion. Adhesive bonding to etched enamel has proven to be efficient and stable . Adhesion to dentin, on other hand, depends on numerous factors related to the substrate morphology(4), the type of adhesive used, and the sensitivity of the application technique.
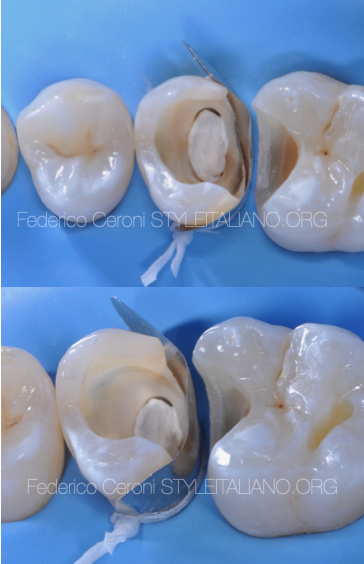
Fig. 4
Another problem that is encountered during the relocation procedure of a cervical margin is the positioning of a wedge which often deforms the matrix. a useful alternative is to use a dental floss to block the matrix without risking deforming it

Fig. 5
A total etch adhesive procedures was performed,
Etching for 30 sec the enamel and 15 sec the dentin.
Then a three step etch and rinse adhesive system was placed
lightcuring for at least 30 sec.
Then i layered the proximal wall with a nano ibrid composite.

Fig. 6
After an endodontic retreatment was performed, the working length was checked radiographically and the subsequent irrigation protocol consisted in 5,25% NaOCL and 17% EDTA. The canal was dried and the filling was performed with warm vertical condensation. Then a composite build up was performed and the tooth was prepared for a veneerlay.

Fig. 7
The preparation for a veneer lay was necessary for esthetic reason.
During another appointment the veneerlay was cemented. The tooth surface was treated with air abrasion and a 3 step etch and rinse adhesive system, the lithium disilicate surface was treated with hydrofluoric acid, orthophosphoric acid, silane and bonding. Then the veneerlay was cemented with a nano filled composite.

Fig. 8
This is result 1 year later. As you can see the infiammation of the papilla disappeared and the coronal part of the papilla regrow. Meaning that a cervical margin relocation, if done correctly it is a valid type of treatment.

Fig. 9
fundamental is the control of the closing margin both between tooth and composite and between composite and inlay, for this reason it is always important to perform intraoral and bitewing xrays.
Conclusions
Our goal must be to restore correct aesthetics and function while preserving the dental structures as much as possible. A minimally invasive approach is essential for a correct resolution of problems involving damage teeth, especially in young patients.
Cervical margin relocation can easily solve apparently complex clinical cases like this one in conservative way.
Bibliography
1 Dietschi D. Spreafico R. Current clinical concepts for adhesive cementation of tooth-colored posteriors restorations. Pract Periodontics aesthet Dent 1998;10:47-54
2 Veneziani M. Adhesive restorations in the posterior area with sub gingival cervical margins: new classification and differentiated treatment approach. Our J Esthet Dent 2010;5:50-56
3 Magne P,Spreafico R. Deep margin elevation: a paradigm shift. Am J Esthet Dent 2012;2:86-96
4 Juloski J,KoKen S,Ferrari M.Cervical margin relocation in indirect adhesive restorations. A literature review.J Prosthodont Res 2018;62:273-280
5 Perdigao J. Dentin bonding as a function of dentin structure . Dent Clin North Am 2002;46:277-301





