An external cervical resorption managed with MTA: 5 years follow up
20/08/2020
Riccardo Tonini
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
In this article it will be explained how to manage an external cervical resorption with MTA. A five years follow up will demonstrate that MTA was the right choice in terms of biocompatibility and sealing performance.
External resorption originates in the PDL and is identified thanks to an irregular radiolucent area overlying the root canal.
External cervical resorption (ECR) typically starts at the cervical root third, apically to the junctional epithelium .
The ECR lesion extends horizontally toward the root canal space and vertically (apically, coronally, or both). During this complex process, the pulp typically remains vital, except for the latest stage of progression when the resorption may penetrate the root canal space and make the pulp necrotic.
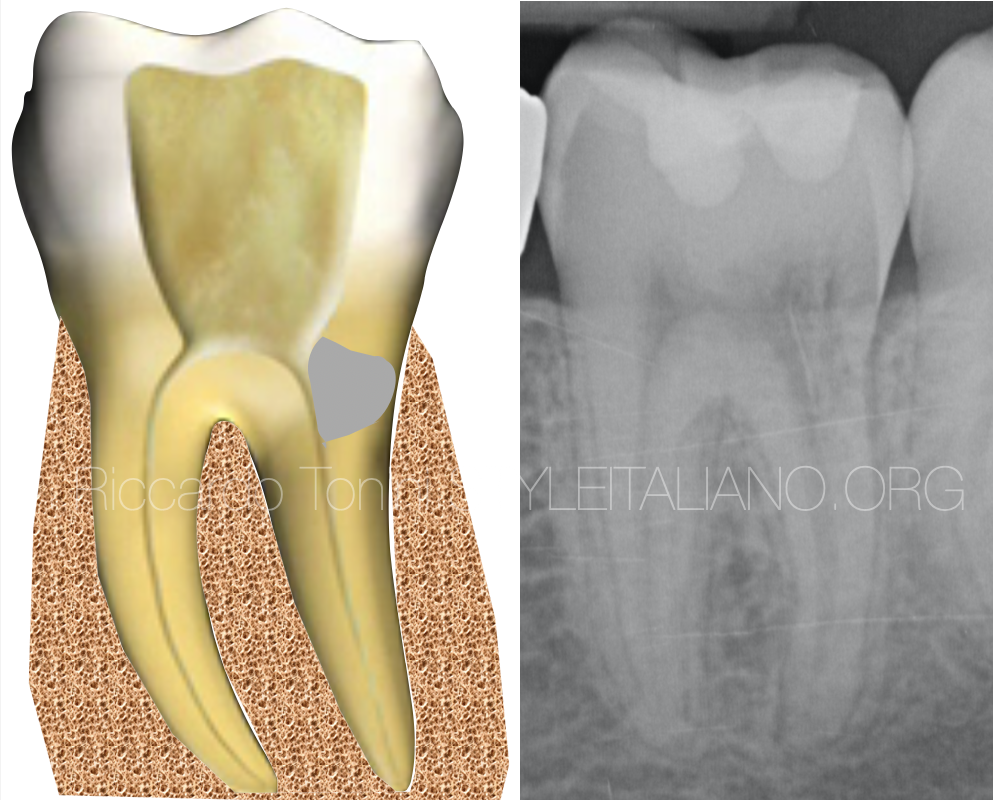
Fig. 1
This distal ECR was completely asymptomatic and the diagnosis occurred only because the 17 years old patient made a panoramic xray. Typically the defect appears in first stages as a light translucency and the root looks more with the bone trabecular aspect.
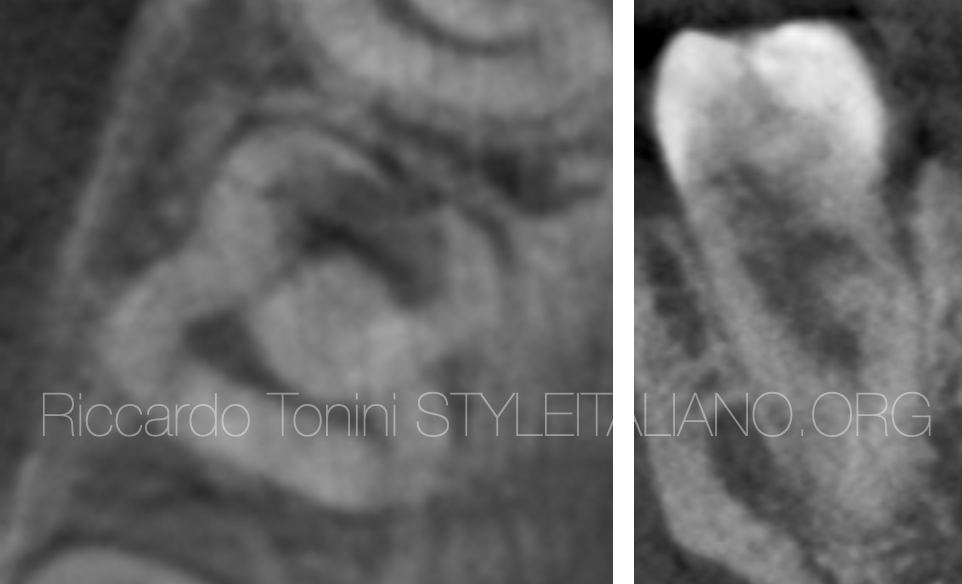
Fig. 2
A CBCT is always recommended in order to identify the location and the extension of the defect. From the images it is evident that the defect is invasive and involves the coronal part of the distal root. It was also suggested to the patient to remove first the 3.8, but he refused.
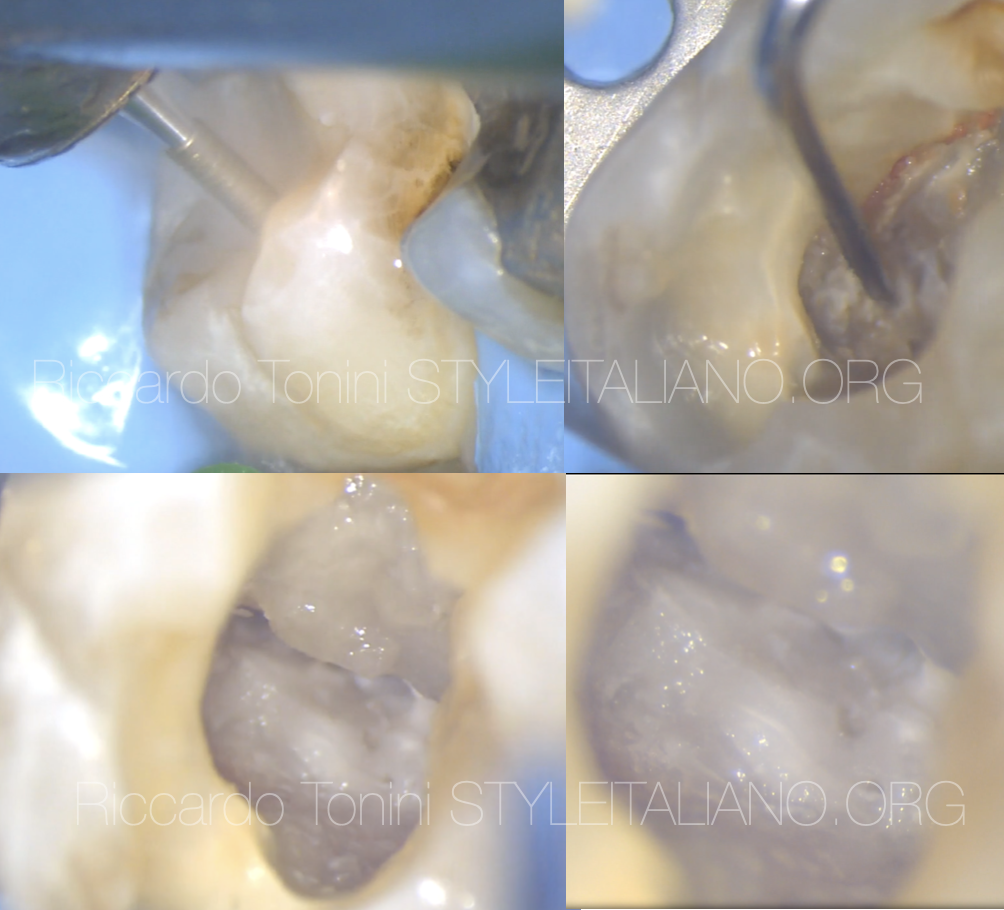
Fig. 3
A RCT has been planned and, considering the distal localization of the defect, an only internal management was the strategical choice.
First of all it is always necessary to perform an access cavity that is able to show us completely the defect. Then, with a bur mounted on a low speed handpiece, all affected tissue must be removed and the tunnel connection between the bone and pulp chamber must be highlighted.
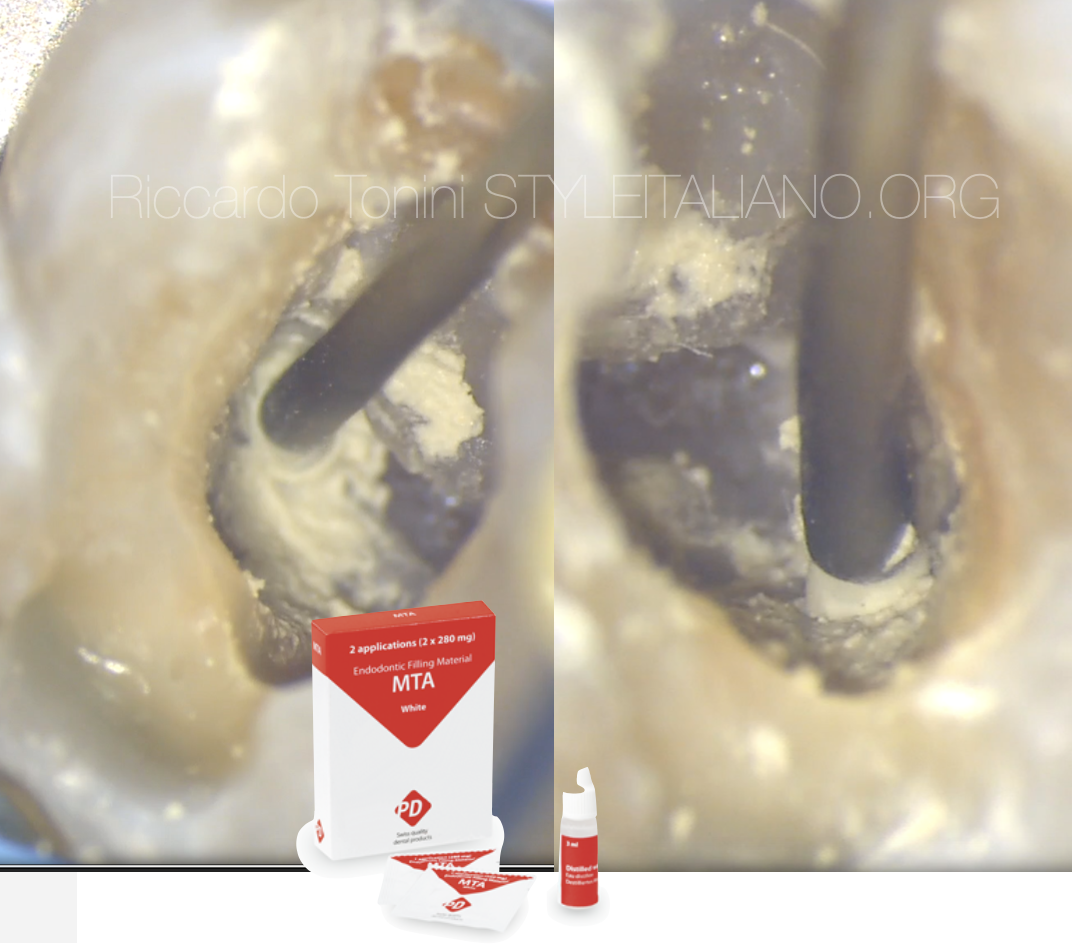
Fig. 4
The canal was isolated with a teflon tape before the placement of white MTA (Produits Dentaires SA), in order to avoid an accidental penetration of MTA inside the canal. The MTA was delivered with Map System in order push the material inside the communication tunnel.
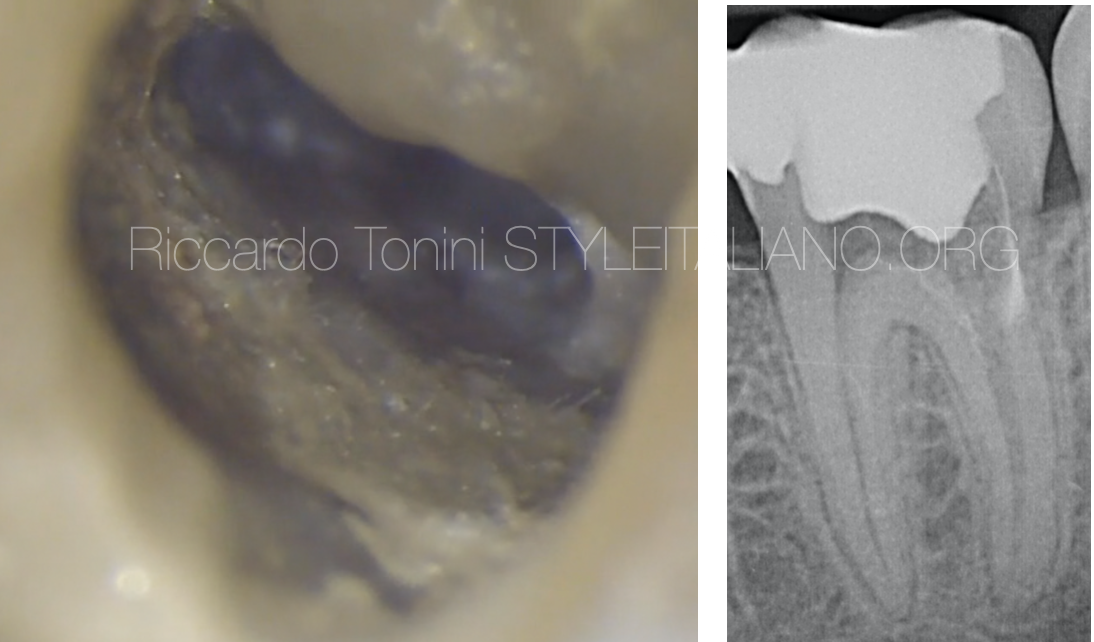
Fig. 5
Post operative x-ray and a microscopic picture that show the right placement of White MTA (Produits Dentaires SA).

Fig. 6
During the second appointment a complete RCT was performed and a composite direct restoration sealed completely the access.

Fig. 7
2 years follow up
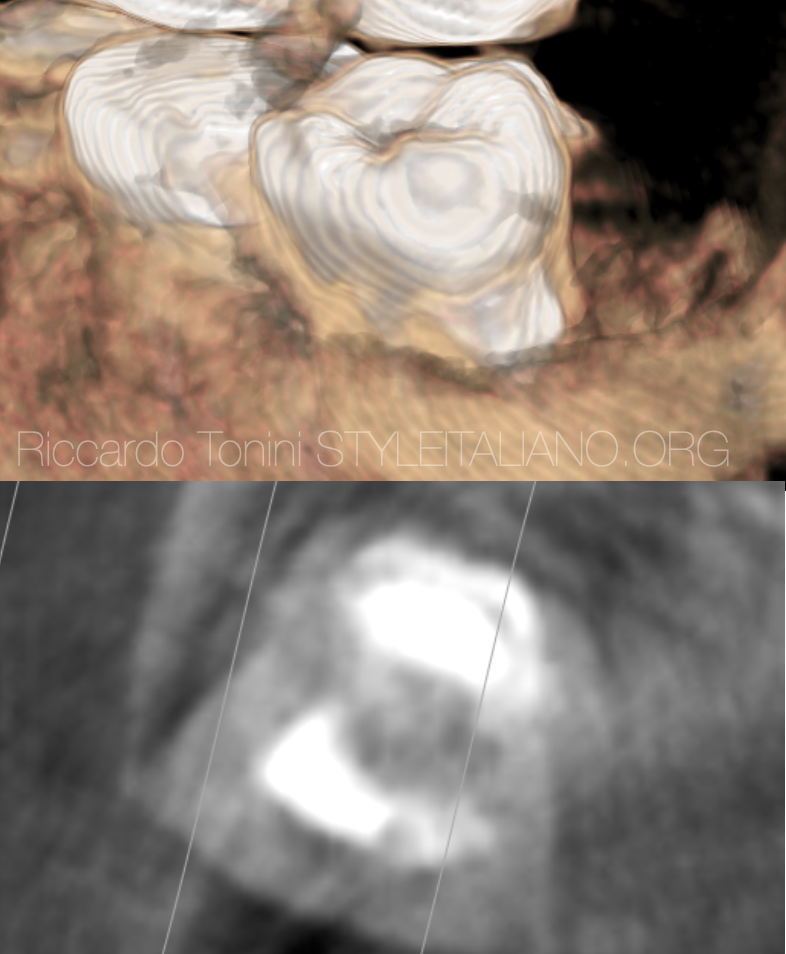
Fig. 8
After 3 years the patient extracted the 3.8 and after 4 years the 4.8. A CBCT was requested for the extraction of 4.8 and it was a good opportunity for checking the MTA seal.

Fig. 9
5 years follow up.
Conclusions
ECR resorptions are always a challenge for the clinician. MTA can be considered the ideal material for sealing from the acces cavity the defects in a predictable way . MTA is a bioactive bioceramic material and it’s 100% biocompatible. A combined delivering with Map System creates a perfect match for managing difficult and extreme clinical situation like ECR
Bibliography
1 American Association of Endodontists. Glossary of Endodontic Terms 2016, 48. Chicago, IL: American Association of Endodontists; 2016.
2. Gold SI, Hasselgren G. Peripheral inflammatory root resorption: a review of the literature with case reports. J Clin Periodontol 1992;19:523–34.
3. Mavridou AM, Hauben E, Wevers M, et al. Understanding external cervical resorption in vital teeth. J Endod 2016;42:1737–51.
4. Heithersay GS. Invasive cervical resorption. Endod Topics 2004;7:73–92.
5. Mavridou AM, Hauben E, Wevers M, et al. Understanding external cervical resorption patterns in
endodontically treated teeth. Int Endod J 2017;50:1116–33.
6. Mavridou AM, Bergmans L, Barendregt D, et al. Descriptive analysis of factors associated with external cervical resorption. J Endod 2017;43:1602–10.