Triple MTA apical plug in second lower molar with overextended guttapercha
04/02/2021
José Conde Pais
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Mineral trioxide aggregate (MTA) was developed in the 1990s as a root-end filling material and has also been recognized as promising when used to form an apical barrier because of its superior biocompatibility and ability to seal and set in the presence of blood . The use of MTA as an obturation material might ultimately provide long-term benefits that enhance the prognosis and retention of the natural dentition in conventional and complex therapies. This material is very useful in cases where we cannot guarantee a correct apical seal with conventional filling techniques.

Fig. 1
A 55-year-old female patient presented in our private endodontic office for evaluation of tooth 47, which had received nonsurgical endodontic treatment years ago. The presenting symptoms included swelling in the buccal vestibule and pain. His health history was unremarkable and radiographic examination revealed a big prefabricated metal post on distal root, overextended gutta-percha associated with extensive periapical bone loss. Clinical examination dis- closed fluctuant swelling in the vestibule proximal to the molar, no mobility and pain on percussion. The diagnosis was acute peri-apical abscess, after discussing treatment options, we decided on an orthograde retreatment. The patient was informed of the pros and cons of the treatment and informed consent was obtained.
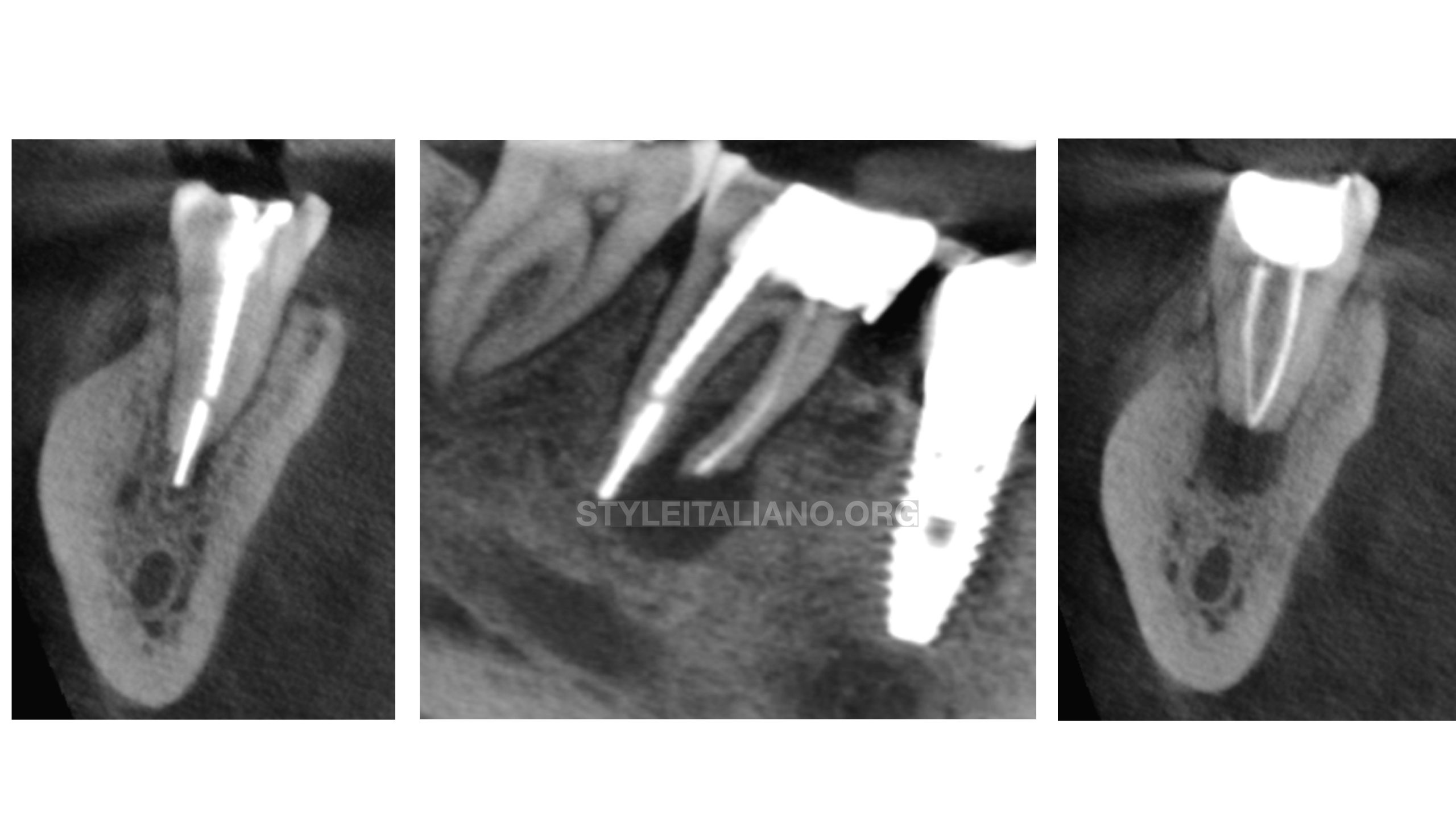
Fig. 2
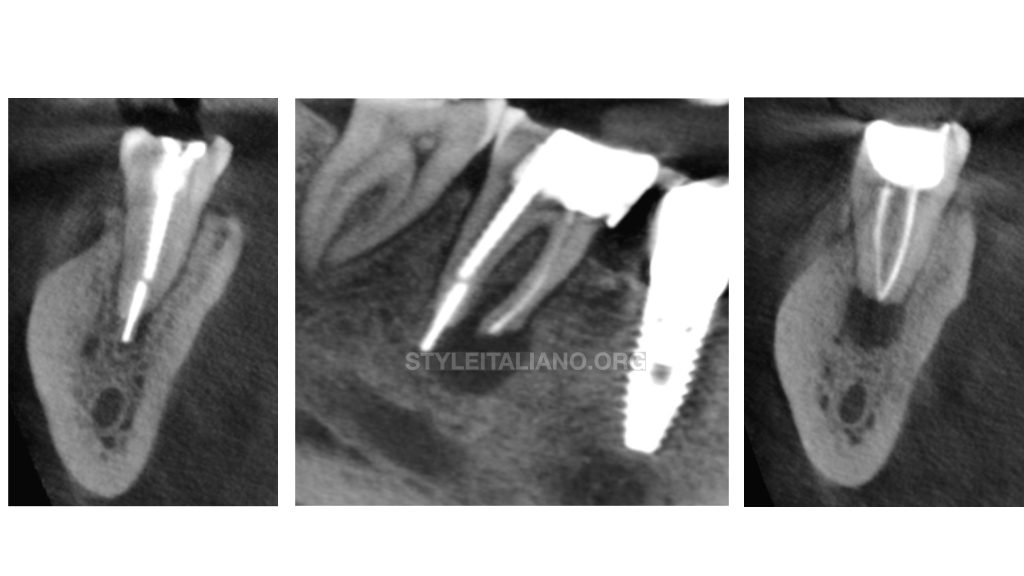
Cone beam sections where we can see overextended material and the apical lesion
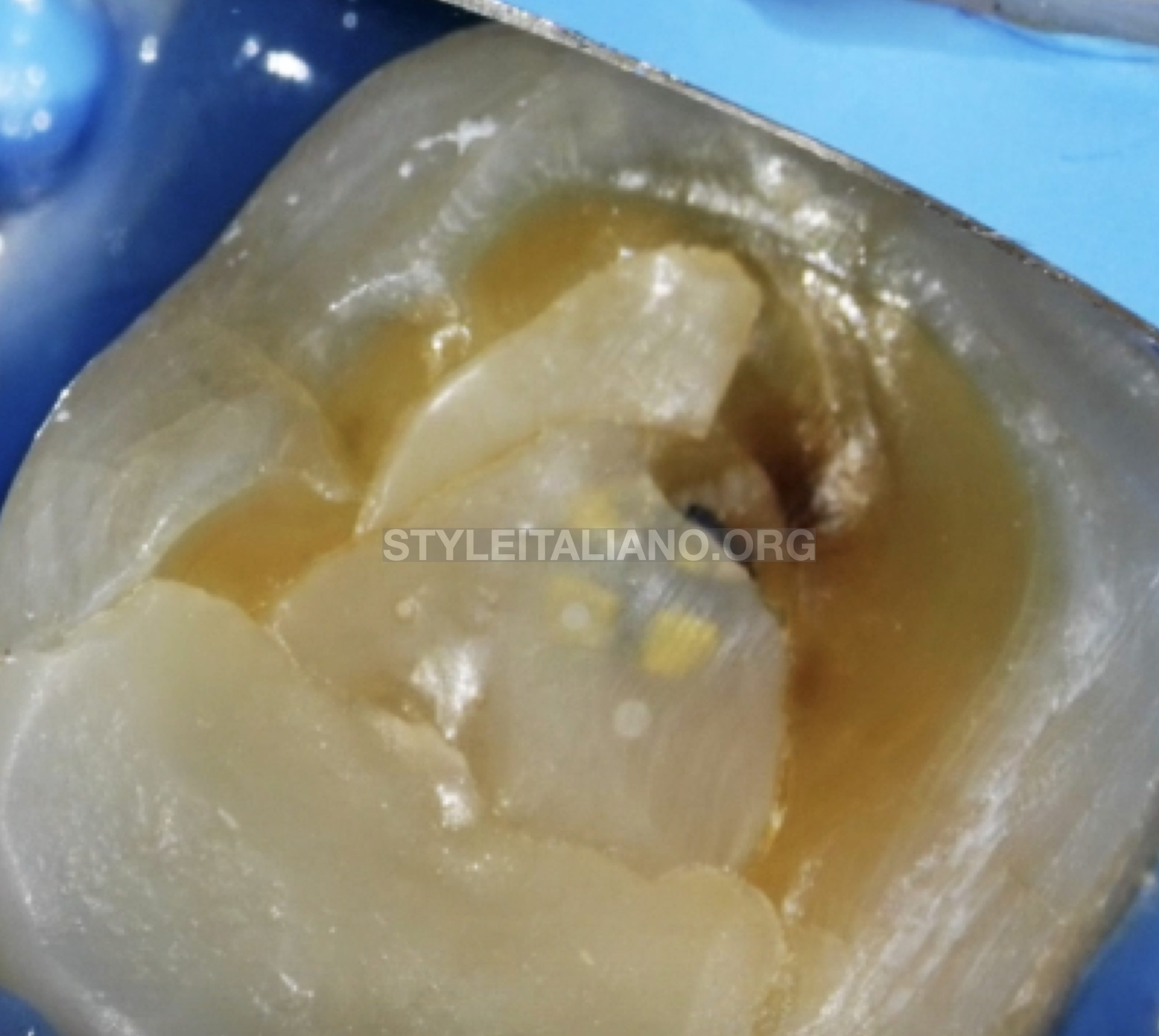
Fig. 3
In this image we can see the preoperative situation and the location of the metal post. After anesthesia and rubber dam isolation, the molar was accessed through the crown .

Fig. 4
The metal Post was removed using ultrasonic tip.
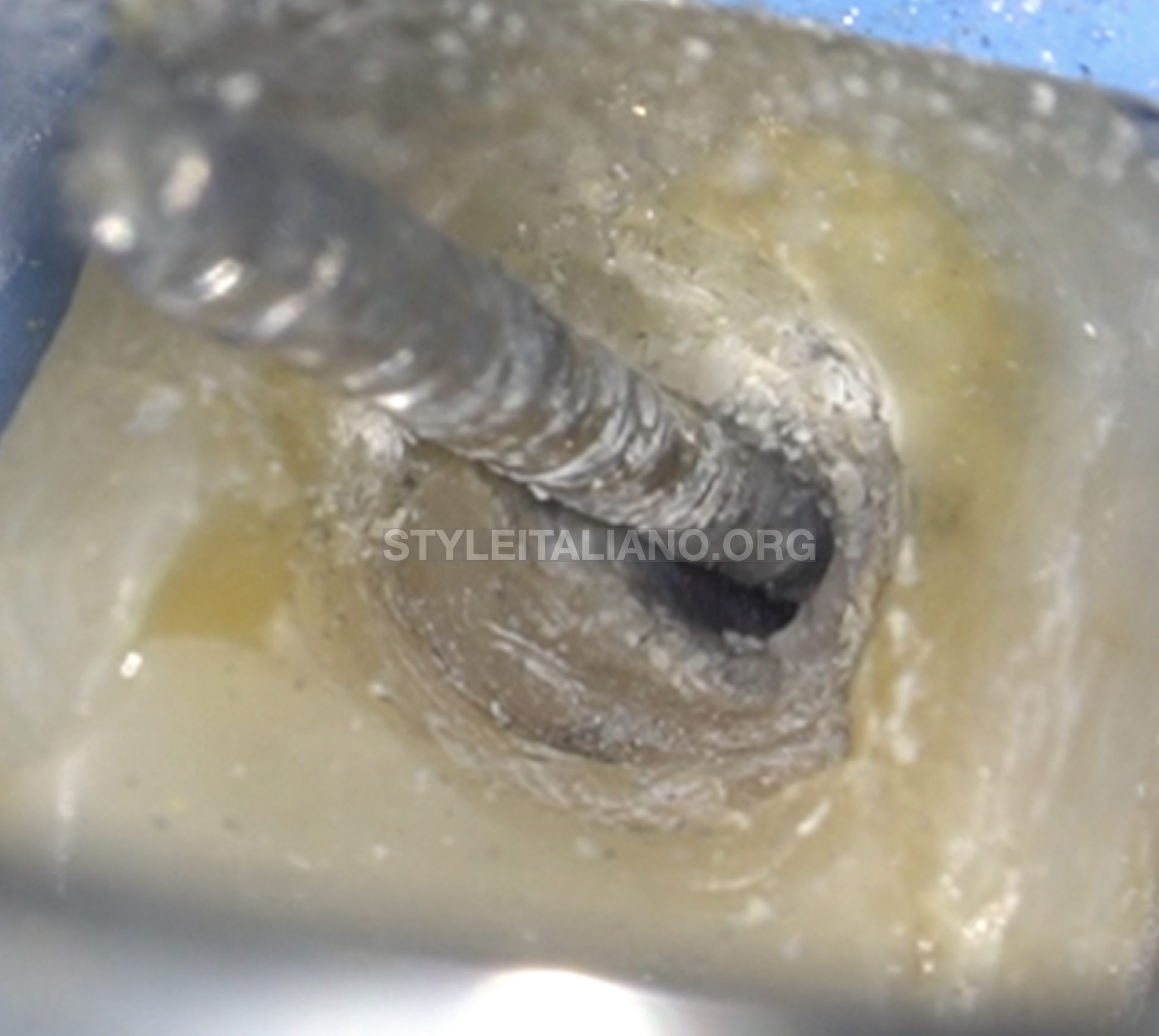
Fig. 5
Metal post removed.

Fig. 6
After removing the post, excess cement was removed with a tapered ultrasonic tip and the gutta-percha was exposed.

Fig. 7
Overextended gutta-percha was extracted using a # 30 hedstrom file.

Fig. 8
The canals was chemomechanically shaped and cleaned using the following protocol:
Desobturation Technique : Reciprocating File R25
Shaping : Protaper Next X1- X5
Irrigation; Sodium hypochlorite 5,25% + Saline Solution + Edta 17% PUI + sodium hypochlorite 5,25% PUI
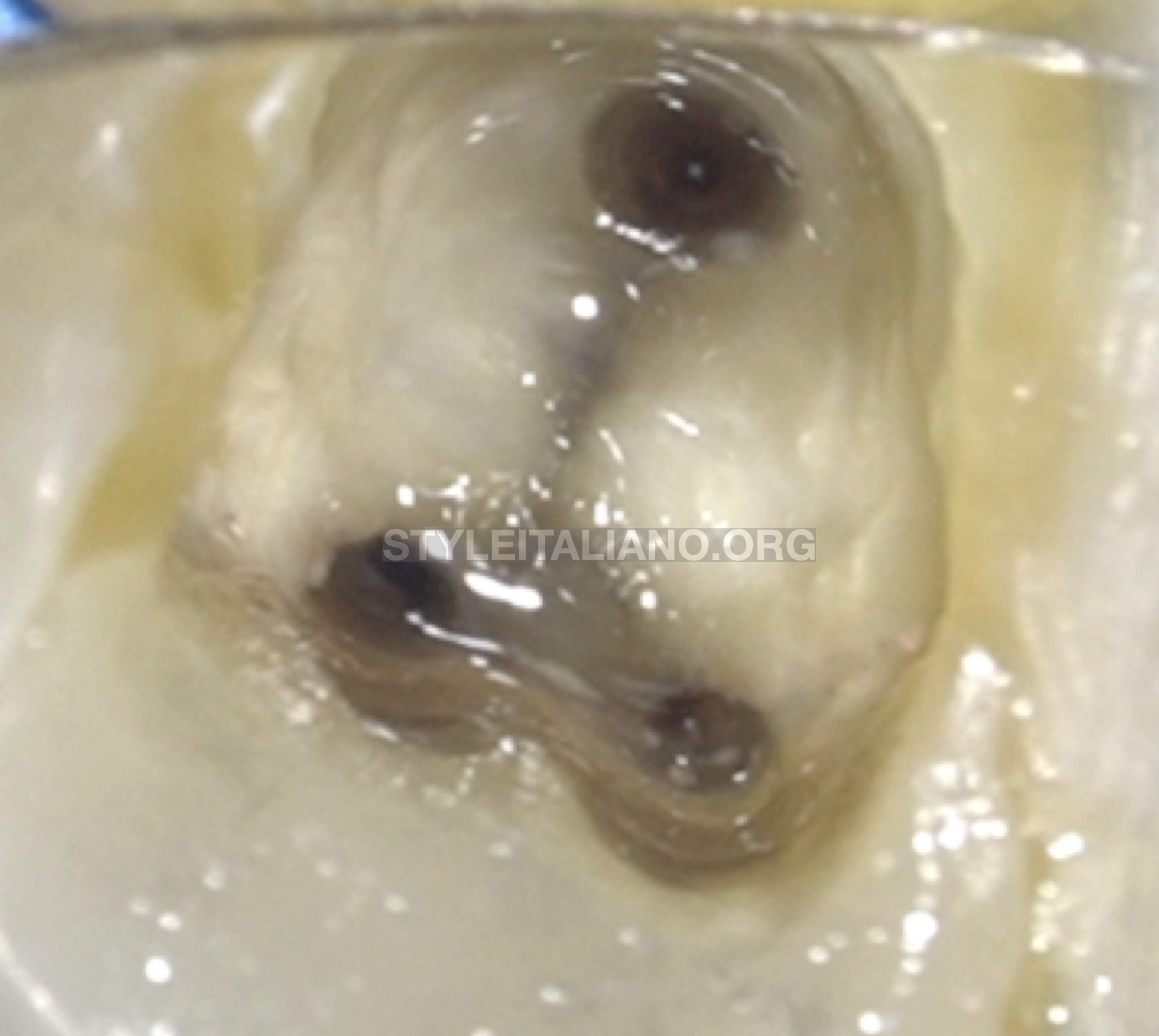
Fig. 9
At the end of the first visit, we remove the remains of gutta-percha adhered to the walls with eucalyptol and let it act for several minutes.

Fig. 10
Image at the end of the first visit, before the application of intracanal medication.

Fig. 11
We apply Calcium Hydroxide as an intracanal medication for two weeks to raise the pH.

Fig. 12
After two weeks we proceed to seal the root canals. In this case, we could not ensure a correct seal with conventional gutta-percha (due to the large apical gauge), we decided to seal with three MTA plugs.
For this process we use the Map System carrier ( Needle Nº 2 ), which ensures easy and predictable handling of the MTA. This system provides a unique and efficient method for precisely placing MTA by orthograde or retrograde approaches.
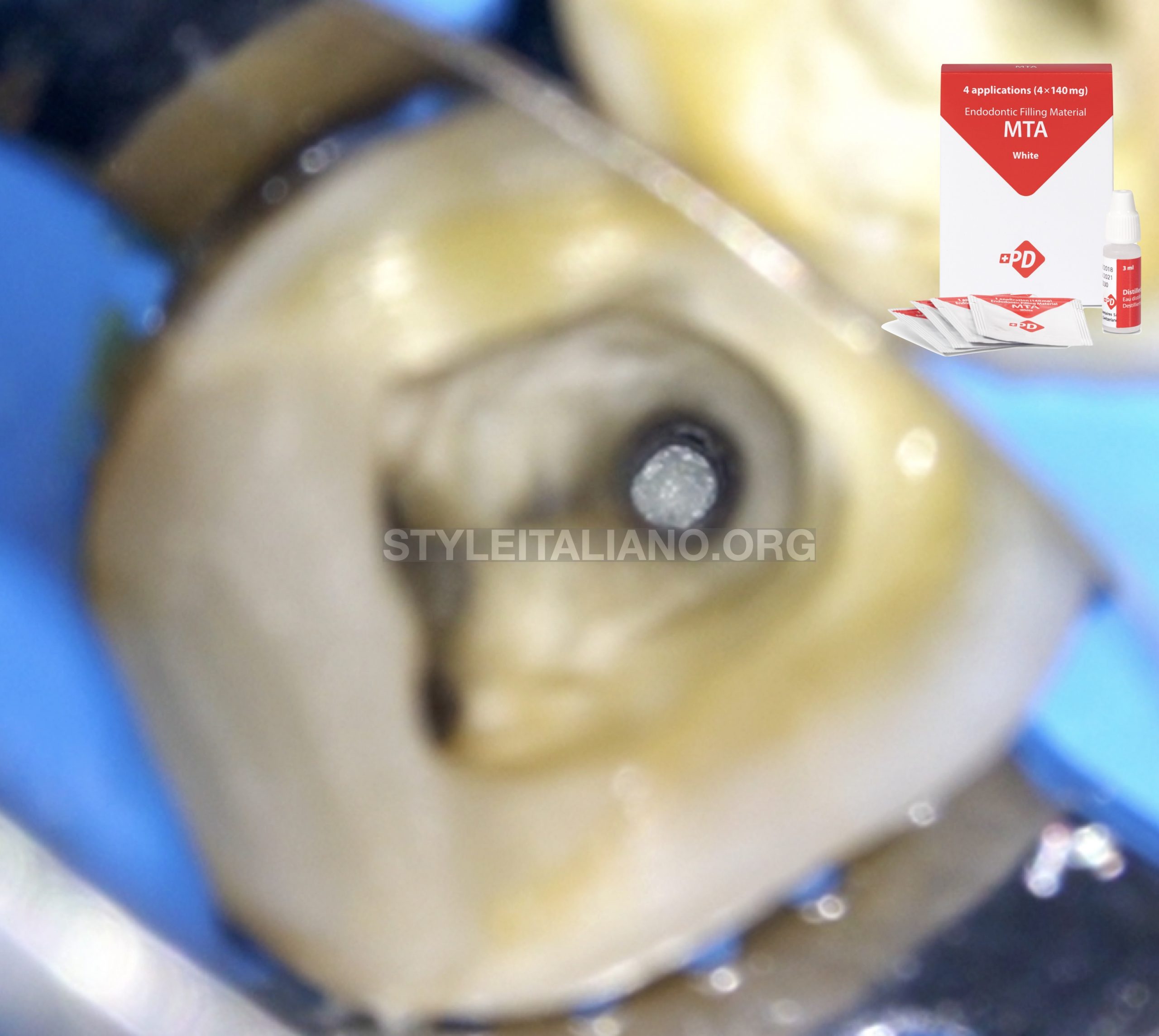
Fig. 13
In this picture we can see the distal apical Plug.

Fig. 14
In this picture we can see the mesial apical plugs

Fig. 15
After sealing the apical third with MTA, we proceed to fill the root canal with injected gutta-percha and make an immediate seal.

Fig. 16
Final Orthoradial xRay

Fig. 17
Final Mesioradial xRay .

Fig. 18
Follow up 10 months.
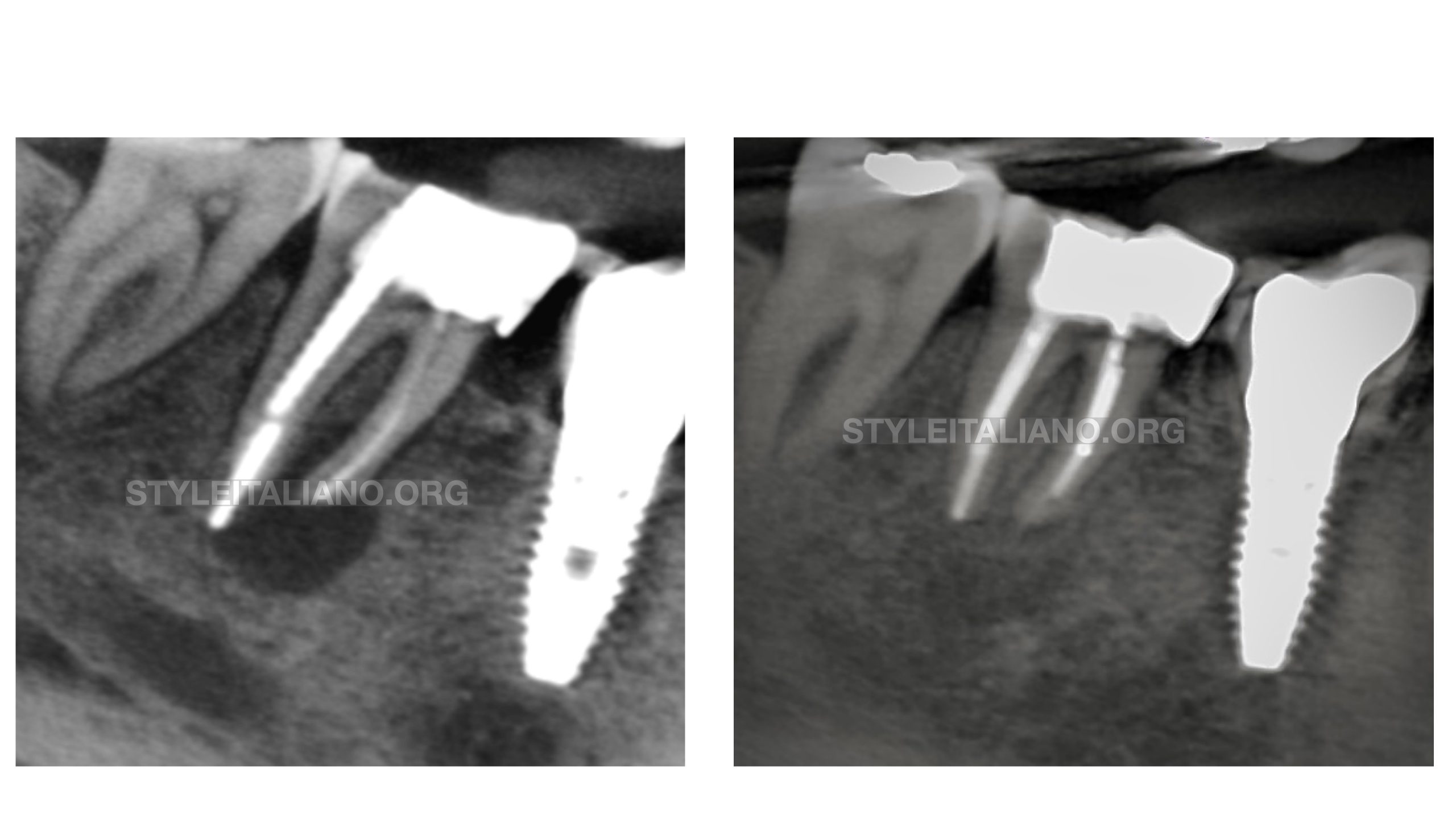
Fig. 19
Comparison
Conclusions
We can conclude that in those cases in which the conventional apical sealing techniques with gutta-percha are not indicated for caliber or irregular morphology, the apical MTA plug techniques is predictable and follows the principles of Style Italiano Endodontics that are feasible, teachable and repeatable.
Bibliography
1. Parirokh M, Torabinejad M, Dummer PMH. Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview – part I: vital pulp therapy. Int Endod J. 2018 Feb;51(2):177-205
2.Torabinejad M, Parirokh M, Dummer PMH. Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview – part II: other clinical applications and complications. Int Endod J. 2018 Mar;51(3):284-317.
3. Bogen G, Kuttler S. Mineral trioxide aggregate obturation: a review and case series. J Endod. 2009;35(6):777-790
4. Stefopoulos S, Tsatsas DV, Kerezoudis NP, Eliades G. Comparative in vitro study of the sealing efficiency of white vs grey ProRoot mineral trioxide aggregate formulas as apical barriers. Dent Traumatol. 2008;24(2):207-213.
5. Santos AD, Moraes JCS, Arau ́jo EB, Yukimitu K, Vale ́rio Filho WV. Physico-chem- ical properties of MTA and a novel experimental cement. Int Endod J 2005;38: 443–7.
6. Koh ET, Torabinejad M, Pitt Ford TR, Brady K, McDonald F. Mineral trioxide aggre- gate stimulates a biological response in human osteoblasts. J Biomed Mater Res 1997;37:432–9.