The probability of two fives
30/03/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The teeth exhibit considerable anatomical variation and abnormalities regarding the number of roots and root canals ( Chandra et al 2009). These variations occur commonly and present a constant challenge in successful diagnosis and endodontic treatment, especially in multirooted teeth, and the clinician needs to be aware of this variability. Understanding the anatomical variations of the root canal system will lead to a complete debridement and filling of the root canals which is essential to the success of the endodontic treatment.
The majority of mandibular first molars usually have two roots with two mesial and one or two canals in the distal root( Vertucci et al 2006). However, the mandibular first molars exhibit considerable anatomical variations regarding the number of roots and canals, and one of them is the presence of an extra root canal in the mesial or distal root called Middle Mesial and Middle Distal Canal, respectively. In a systematic review ( Bansal et al 2018) about the morphology and prevalence of middle canals in mandibular molars was found that the prevalence of MMC and MDC in various populations was reported as up to 53.8% and 10% respectively.
Gupta et al reported that MMC and MDC were found confluent with their respective mesial/distal buccal canals at the junction of the middle and apical 1/3, indicating the presence of three orifices and two apical foramina in each root.
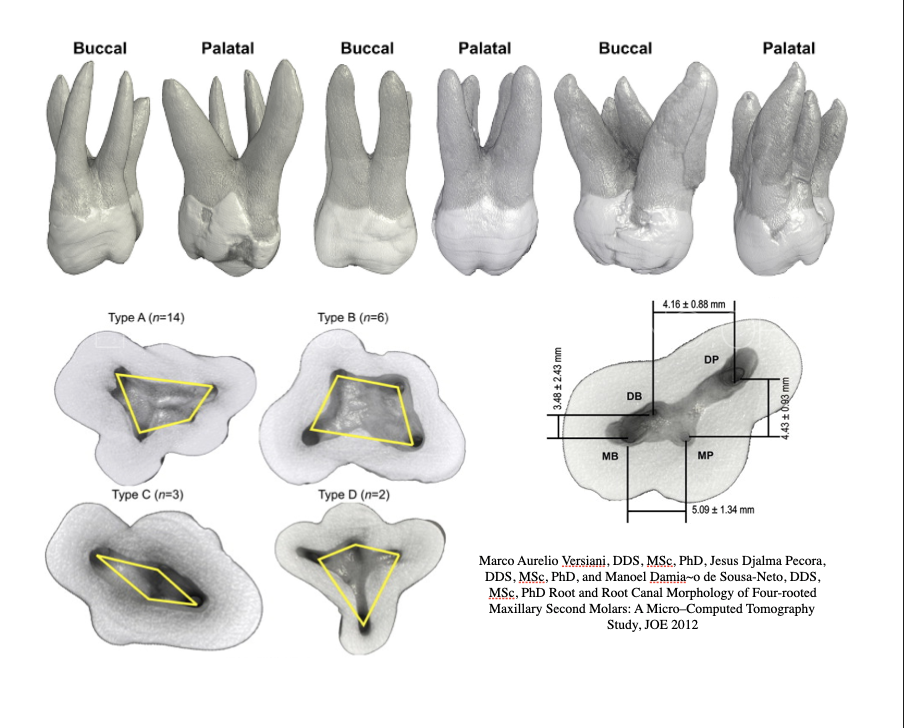
Maxillary second molars usually have three roots and three canals, while a second mesiobuccal canal is found in 56,9%-79,6% of cases( Peikoff et al 1996). However, the rare variation of having three mesial canals in the mesio-buccal root of second molars has not widely been reported in literature.
Three-canal mesiobuccal roots have been reported to occur in 0,2-12.5%, 0,6-4,2% and 1.3% of first, second and third maxillary molars, respectively (Degerness et al 2010).
Sert& Bayirli (2004) studied the anatomy of 400 maxillary first and second molars in Turkish population and found MBR with three canals in only 5 specimens.
Ordinola-Zapata et (2020) imaged 265 extracted maxillary first and second molars with different root configurations with a micro-CT scanner. MB3 canal was observed in 10 maxillary first and only 6 maxillary second molars.
The present case report describes the clinical detection and successful endodontic management of a mandibular first molar with three distal canals and a maxillary second molar with three mesiobuccal canals , both exhibiting confluent root canal configuration. The interesting part was that both teeth were identified in the same patient.

Fig. 1
A 70 years old male with clear medical history was referred for endodontic assessment and treatment of #46 and of #27.
Both teeth had very extensive amalgam restorations that were broken and the patient started to have pain on biting on both teeth, and on #27 sensitivity to hot and cold was getting worse.
Upon clinical examination recurrent decay was noted on both teeth, the #46 was very tender to percussion and had no response on thermal stimuli. Tooth #27 was also tender to percussion but also hypersensitive to thermal stimuli.
The teeth were not mobile, and periodontal probing around the teeth was within normal limits.
Patient was going to have both teeth restored with crowns, and #27 was a strategic tooth to retain due to the loss of #26 a few years ago.
A decision to perform endodontic treatment of both teeth was made and a written informed consent was obtained from patient.

Fig. 2
Tooth #46
Diagnosis of Pulp necrosis and Symptomatic Apical Periodontitis was made for #46.
Caries removed and the restorability of the tooth was assessed. Sufficient ferrule was present for an adequate indirect restoration.
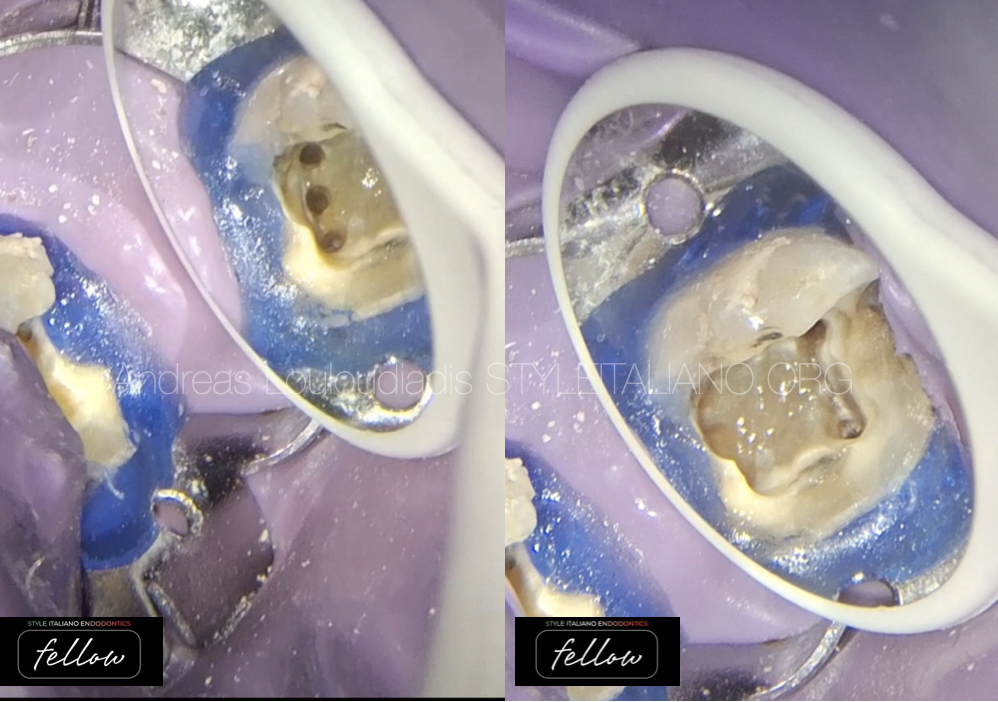
Fig. 3
Rubber dam seal used
Access Cavity Preparation was made and 4 canal orifices were detected initially: MB, ML and D and DL.
Troughing under high magnification with US tip and exploration using a DG 16 explorer revealed an additional MD canal.
Working length Determination with Electronic Apex Locator .
Apical patency was achieved using 08, 10 stainless steel hand files. Cleaning and shaping of the root canals were done with rotary instruments taper 4% under copious irrigation with 3%% sodium hypochlorite throughout the procedure.

Fig. 4
Irrigation protocol included irrigation with 3% Sodium Hypochlorite, 17% EDTA and ultrasonic activation of irrigants with the use of Ultra-X tip..
Irrigation with 3% Sodium Hypochlorite using irriflex needle tip
Ultrasonic activation of 3% sodium hypochlorite irrigant with Ultra-x blue tip.

Fig. 5
Final x-ray of #46.
Obturation of canals with pulp canal sealer utilizing WVC using Fast Pack and Fast Fill. The MD is converging with MB canal at the apical 1/3 showing a Sert and Bayirli Type XVIII canal configuration( Sert& Bayirli 2004).
Access cavity was restored with composite resin and patient was scheduled to return for RCT on#27.

Fig. 6
Final X-ray of tooth 46.
Mesial shift.

Fig. 7
Tooth #27
Pre-operative photo of tooth #27 revealing broken amalgam restoration and secondary decay.
Tooth was extremely sensitive to thermal stimuli and tender to percussion.
A diagnosis of Symptomatic Irreversible pulpitis and Symptomatic Apical periodontitis for #27.

Fig. 8
Removal of defective amalgam restoration, cleaned decay and pre –endo build up was performed with composite resin and access was made into pulp chamber.
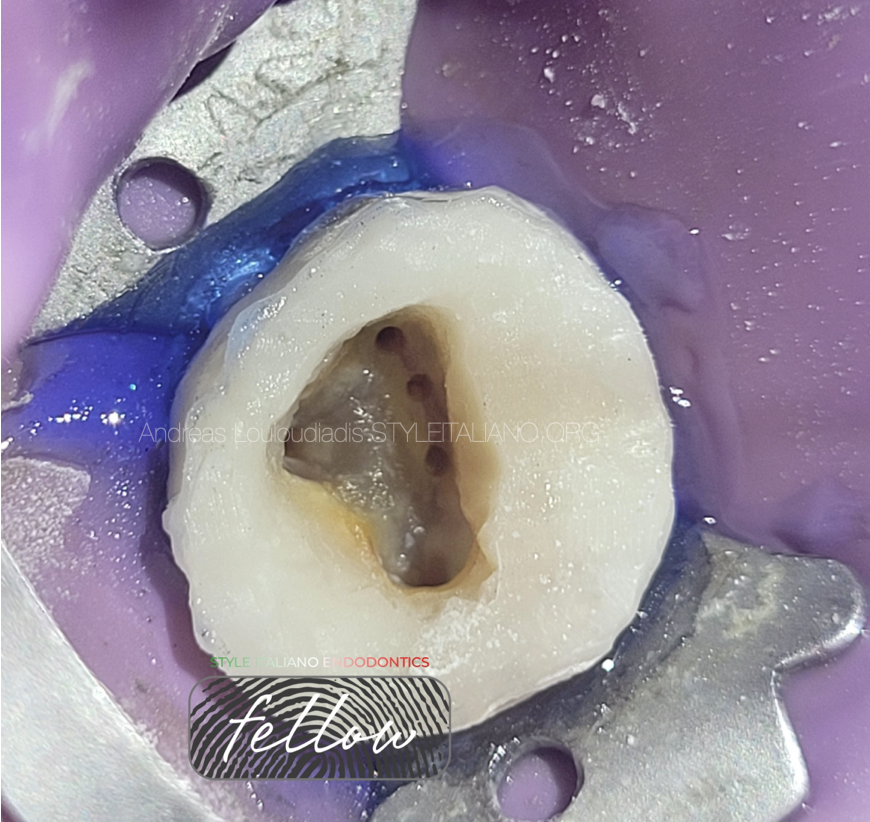
Fig. 9
Access Cavity Preparation.
Rubber dam seal used. The opening access was modified so that the pulp chamber could clearly be exposed. The chamber floor was examined with an endodontic explorer DG-16 under magnification. Five root canal orifices were revealed: three mesio buccal, one distobuccal and one palatal.

Fig. 10
Working Length determination.
The canals were scouted with 08k and 10k stainless–steel hand files.To determine the working length an electronic apex locator was used and confirmed radiographically.
The mesiobuccal canal anatomy was confluent with all 3 canals merging at the apical 1/3. They originated as a separate orifices, MB1, MB2 and MB3 but apically they joined with the MB1 canal.
Cleaning and shaping of the root canals were done with 4% taper rotary instruments under copious irrigation with 3%% sodium hypochlorite throughout the procedure.

Fig. 11
Irrigation protocol included irrigation with 3% Sodium Hypochlorite, 17% EDTA and Ultrasonic activation of irrigants with the use of Ultra-X tip.
Obturation done with Pulp canal sealer and with WVC.

Fig. 12
Photos of before and after obturation of tooth #27.

Fig. 13
Final X-ray of tooth 46.
The MB2 and MB3 are converging with MB1 canal at the apical 1/3.
Access cavity was restored with composite resin and patient was referred back to his dentist for indirect cast restorations of both #46 and #27.

Fig. 14
Final X-ray of tooth 27.
Distal shift.

Fig. 15
Pre-op and post op radiographs of both teeth #46, and #27.

Fig. 16
About the author:
Andreas Louloudiadis
DMD 2001 University of Alabama USA
PGDip in Endodontics 2005 Aristotle University Greece
MSc in Advanced Endodontics 2023 Siena Italy
Full time private practice limited to Endodontics
Tutor at the 2nd level Master of Advanced Endodontics, University of Siena Italy
Certified Member of European Endodontic Society
Member of British Endodontic Society
Member of Hellenic Association of Endodontists
Fellow of SIE
Conclusions
Variations of anatomy do exist more often than we think and may result in frustration for some and fascination for others.
This article focuses on an uncommon anatomical variation where both a right first mandibular molar and a left maxillary second molar on the same patient demonstrated a 5-canal root canal configuration. The incidence of a third distal canal in mandibular first molar and a third mesiobuccal canal in maxillary second molar is extremely low. Nevertheless, clinicians should be alert to the variations in the number of roots and root canals and the peculiar or eccentric locations of root canals . Also, clinicians should be aware of the possibility that more than one unusual anatomic variation can exist when they treat multiple teeth in the same patient as described in this article.
A thorough knowledge of root canal anatomy and its variations, careful interpretation of the radiograph, close clinical inspection of the floor of the chamber, proper access preparation , a detailed exploration of the interior of the tooth, proper armamentarium( magnification and illumination) and lots of patience are essential for a successful treatment outcome.
Bibliography
Chandra S, Rajasekerran M, Shankar P, Indira R. Endodontic management of a mandibular first molarwith three distal canals confirmed with the aiad of spiral computerized tomography. Oral Surg Oral Med Oral Path Endod 2009;108(4):77-81
Bansal R,Hedge S, Astekar M. Morphology and prevalence of middle canals in mandibular molars. A systematic review. J Oral Maxillofac Path 2018;22(2): 216-226
Degerness RA, Bowles WR. Dimension, anatomy and morphology of the mesiobuccal root canal system in maxillary molars. J endod 2010;36:985-989
Gupta S, Jaiswal S, Arora R. Endodontic management of permanent mandibular left first molar with six root canals. Contemp Clin Dent.2010;3:S130-3
Kottoor J, Velmurugan S&N. Middle Distal canal of the mandibular first molar: a case report and literature review. Int Endod J. 2010;43:714-722
Kimura Y, Matsumoto K. Mandibular first molar with three distal root canals
Int Endod J 2000;33:468-470
Peikoff MD, Christie WH, Fogel HM. The maxillary second molar: variations in the number of roots and canals.
Int Endod J. 1996;29:365-369
Ordinola-Zapata R, Martins NR, Bramante CM, Plancencia H, Versiani M. The MB3 canal in maxillary molars. A micro-CT study. Clin Oral Investig 2020;24(11):4109-4121
SertS, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth in Turkish population J Endodd 2004;30|:391-8
Vertucci F, Haddix JE, Britto LR. Tooth morphology and access cavity preparation. In: Cohen S, Hrgreaves KM, eds. Pathways of the Pulp 9th edn. St Luis , Mo USA :Mosby pp 148-232