The endodontic dark hole
24/10/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Internal resorption is a complex case that requires multiple tools and knowledge to treat it properly.
Internal resorption is a condition in vital cases where is the loss of dentin in the canal space, and is caused by multi-nucleated giant cells called dentinoclasts.
This case was referred to me by a dear colleague after opening access he found severe bleeding and a lot of tissues, he thought he made a perforation that’s why he referred her.
In this case after taking pre operative xray I sent the patient to make a cone beam CT to determine whether it was a perforating resorption or not.
After viewing CBCT it was perforating the tooth mesially and distally , at this moment we decided the treatment plan and how we will close the tooth.
Operator must have sufficient knowledge, skills and tools to manage such cases.
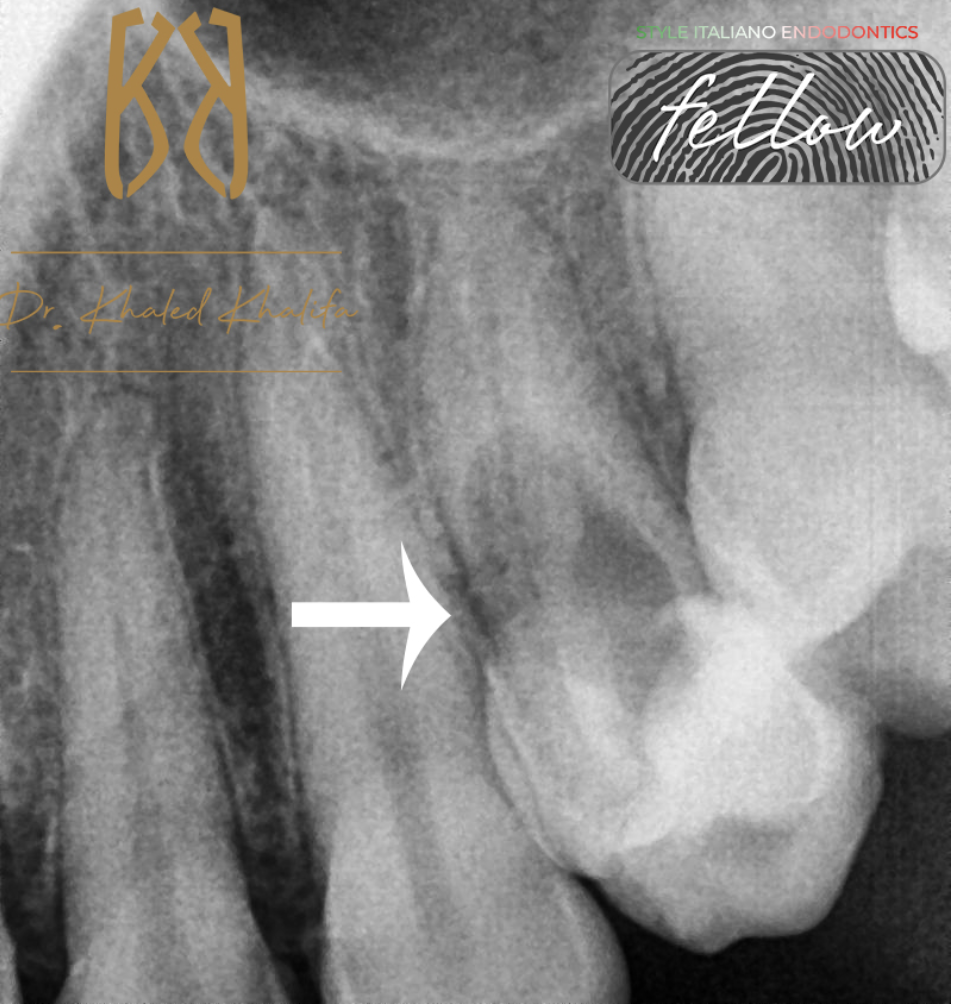
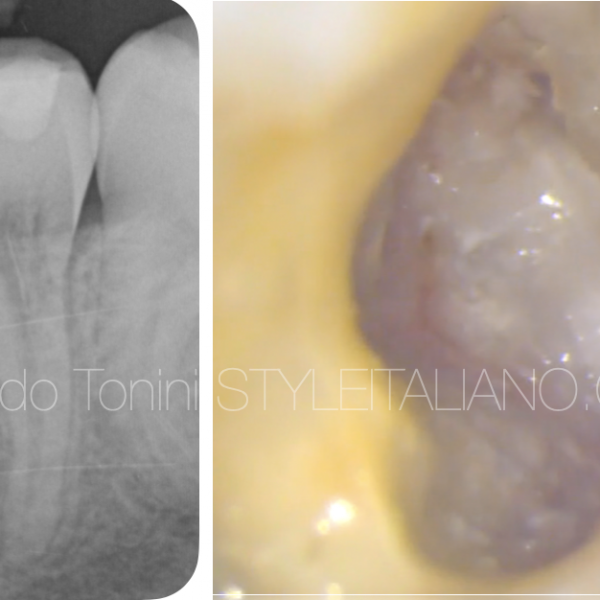
Fig. 1
Preoperative X-Ray showing massive internal resorption inside the premolar.
Sending patient to CBCT is a must to determine if its perforating the root or not.
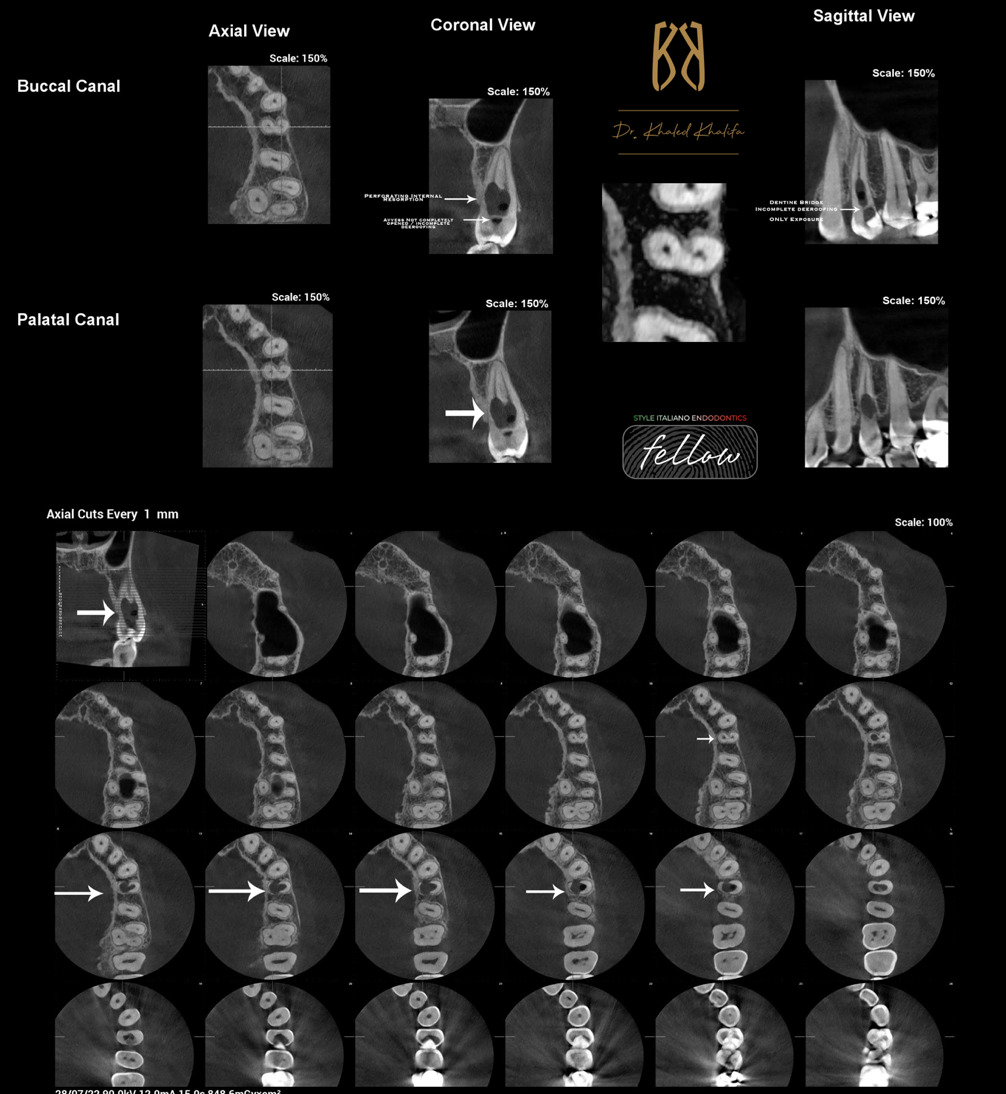
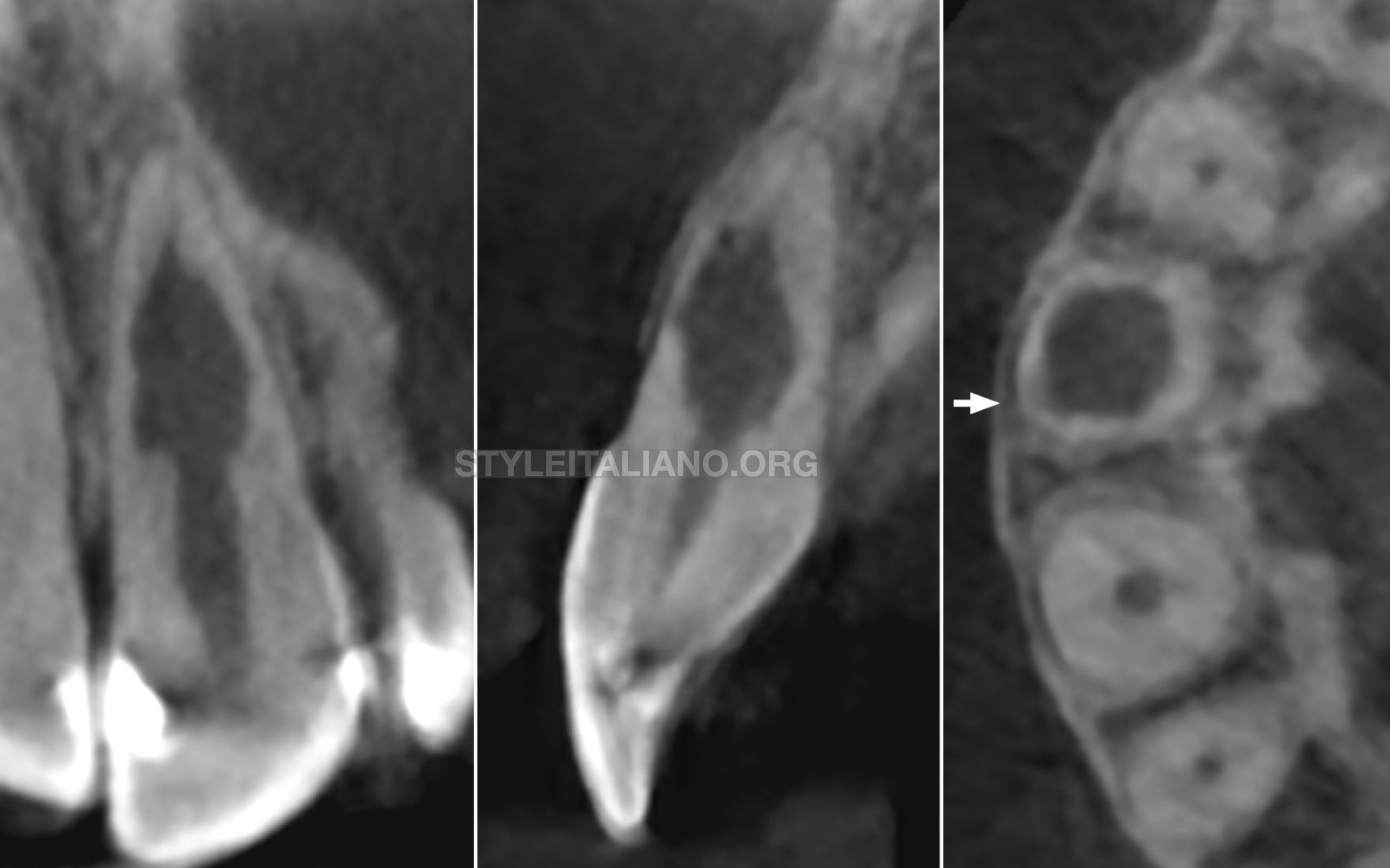
Fig. 2
CBCT Examination showed:
- Incomplete deerofing of pulp chamber by previous dentist
- Massive internal resorption
- Level of canal opening is very deep below internal resorption
- Perforating mesially and distally in multiple cuts
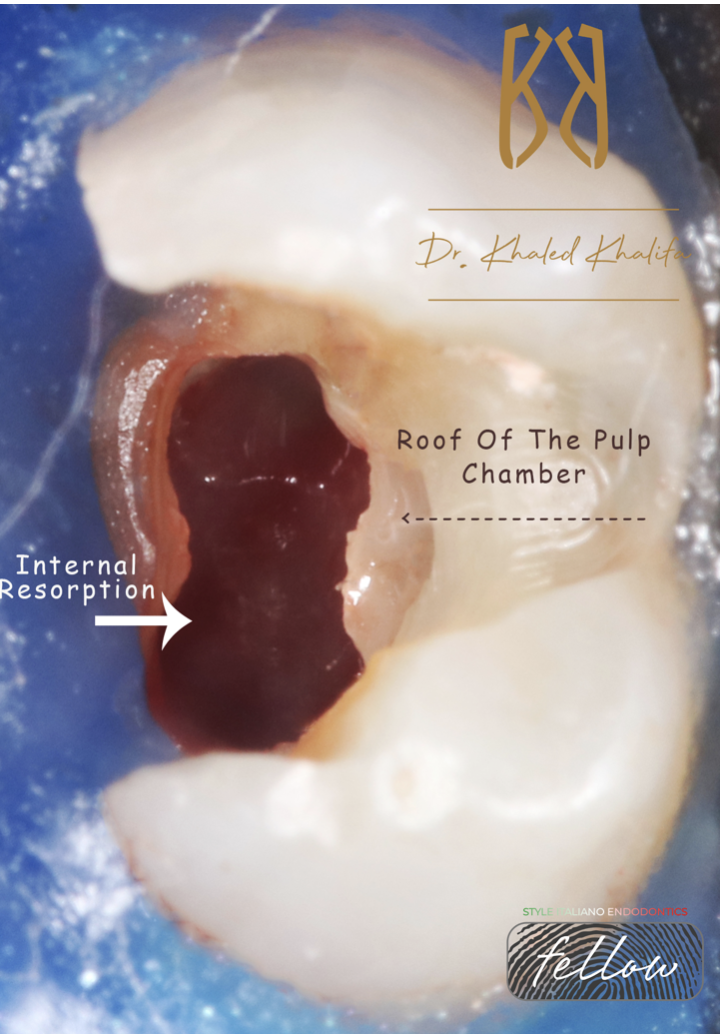
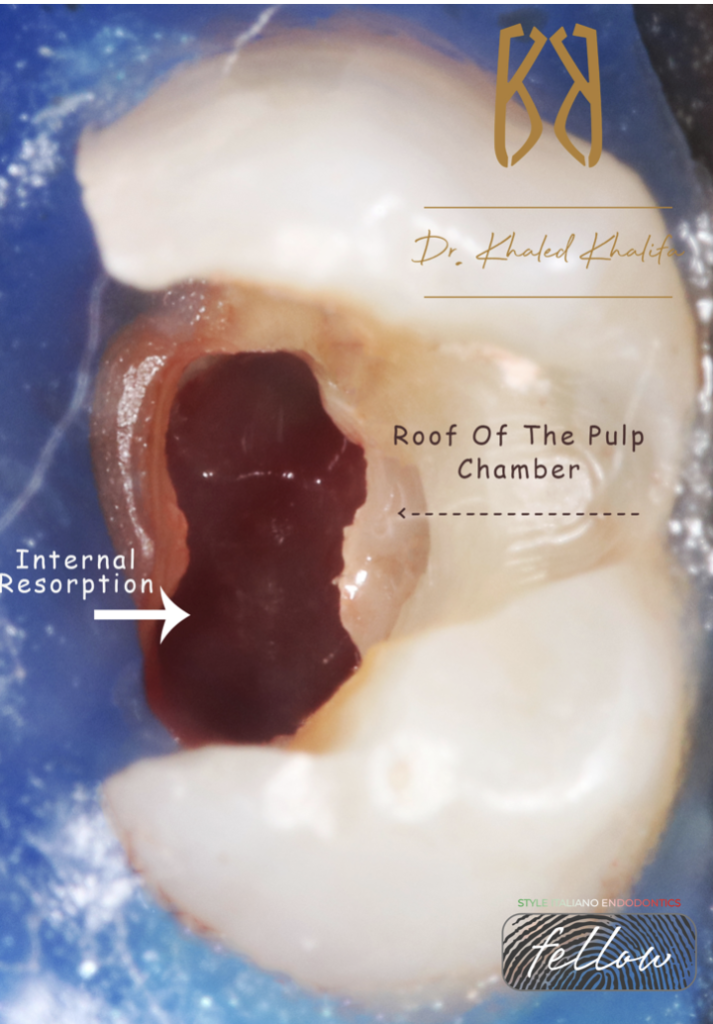
Fig. 3
After removing the temporary filling, incomplete deerofing and internal resorption tissues were evident.
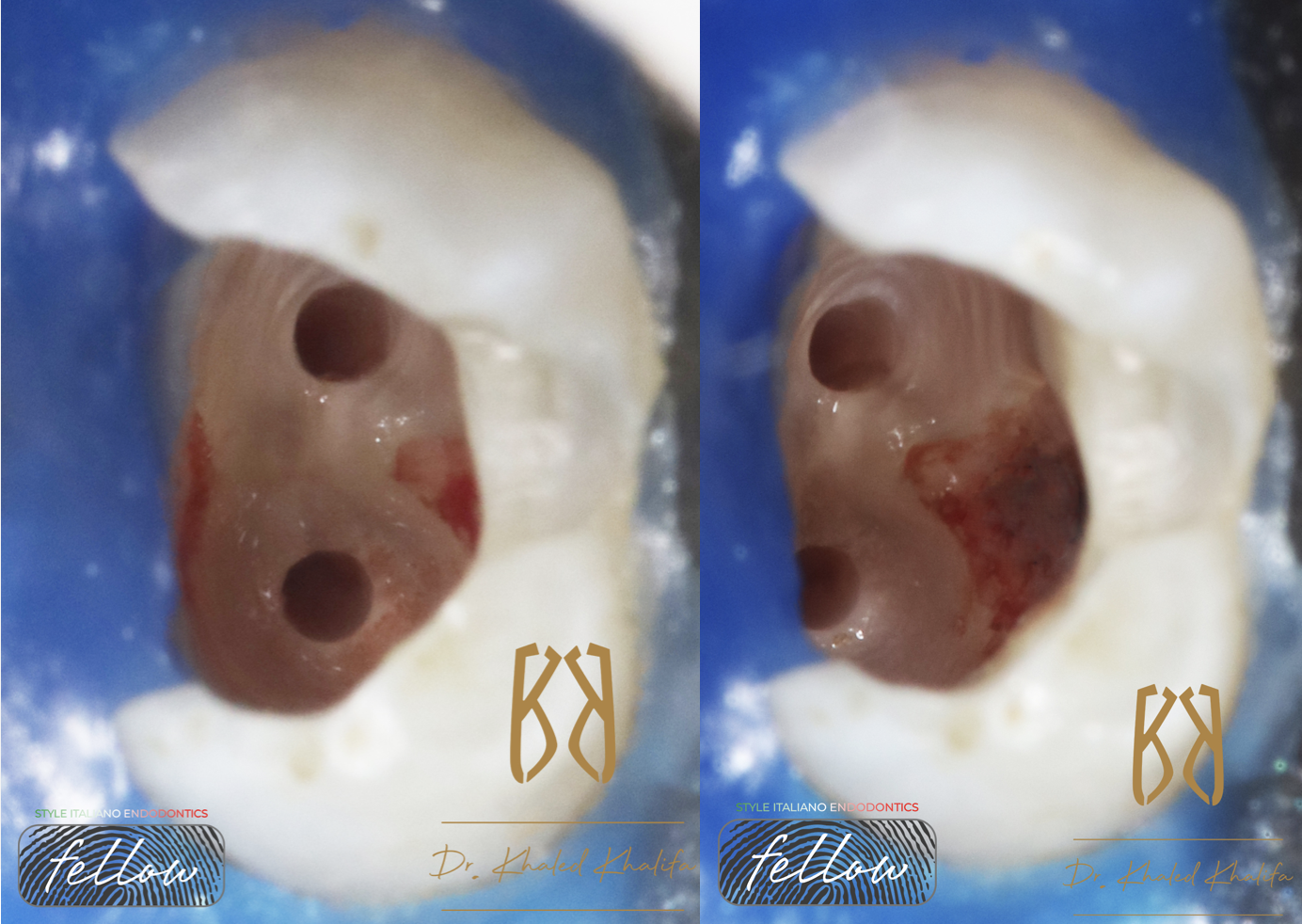
Fig. 4
The treatment strategy was to remove all granulation tissues resulted from internal resorption using sodium hypochlorite and activation devices in order to dissolve them all.
Passive ultrasonic irrigation was used to ensure removing all tissues and micro endodontic escavator to remove the bulk of tissues.
Complete cleaning and shaping of all canals after achieving hemostasis which was easy after removing all internal resorptive tissues.
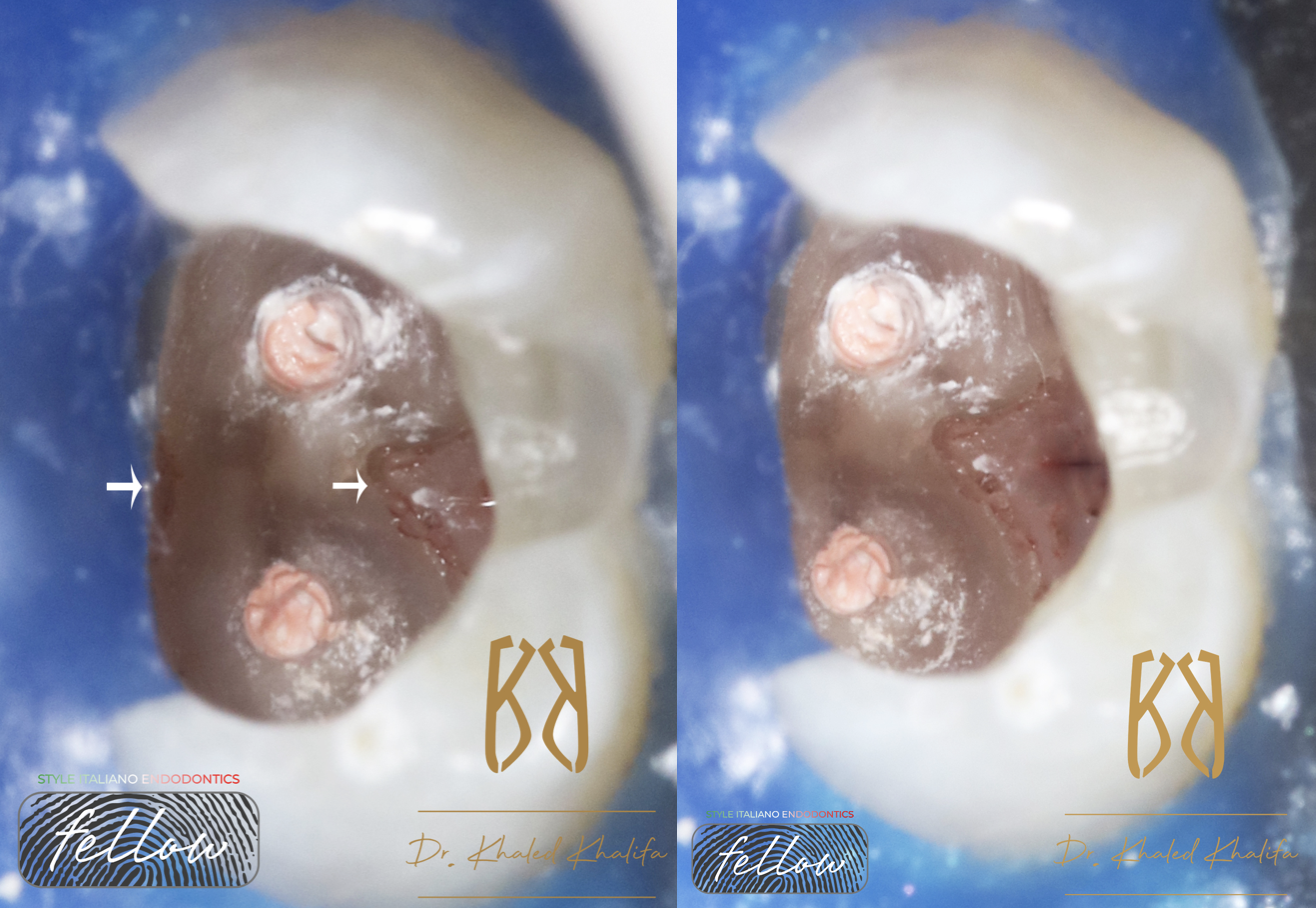
Fig. 5
In this case I preferred to fill the canals by gutta percha and Bioceramic sealer, then close the rest with bioceramic putty to ensure closing all perforation mesially and distally and to use the putty in proper thickness in order to give me proper compressive strength as well.
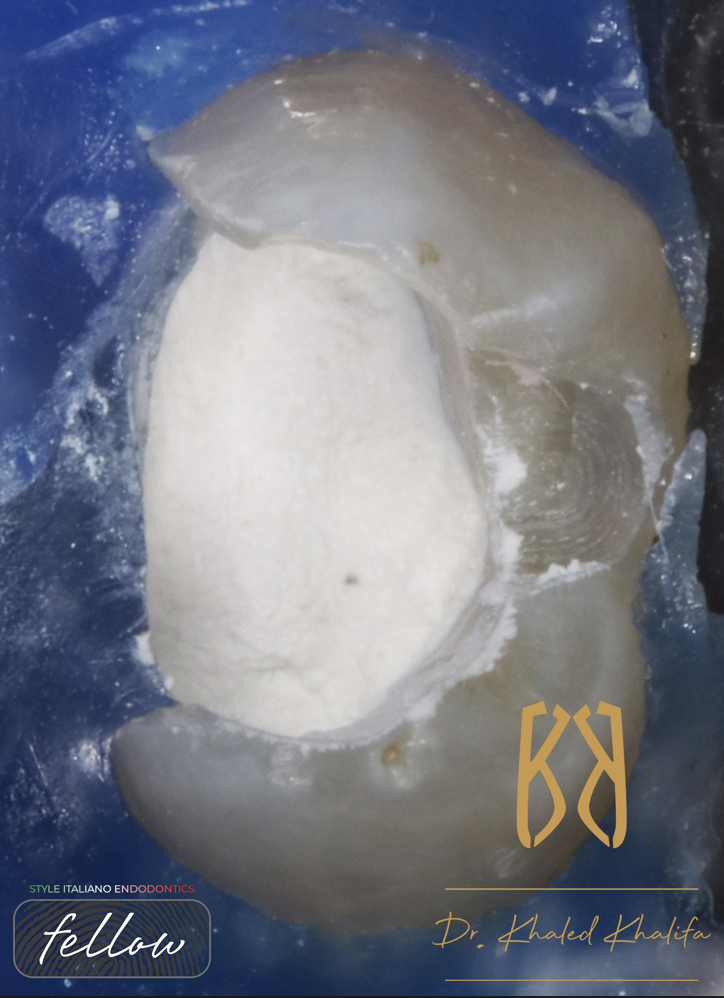
Fig. 6
Bulk of bioceramic putty placed deep down from middle half of the root where the canals started up till CEJ.
This ensures complete closure of all perforation and compressive strength to equalize the massive loss in tooth structure by internal resorption.
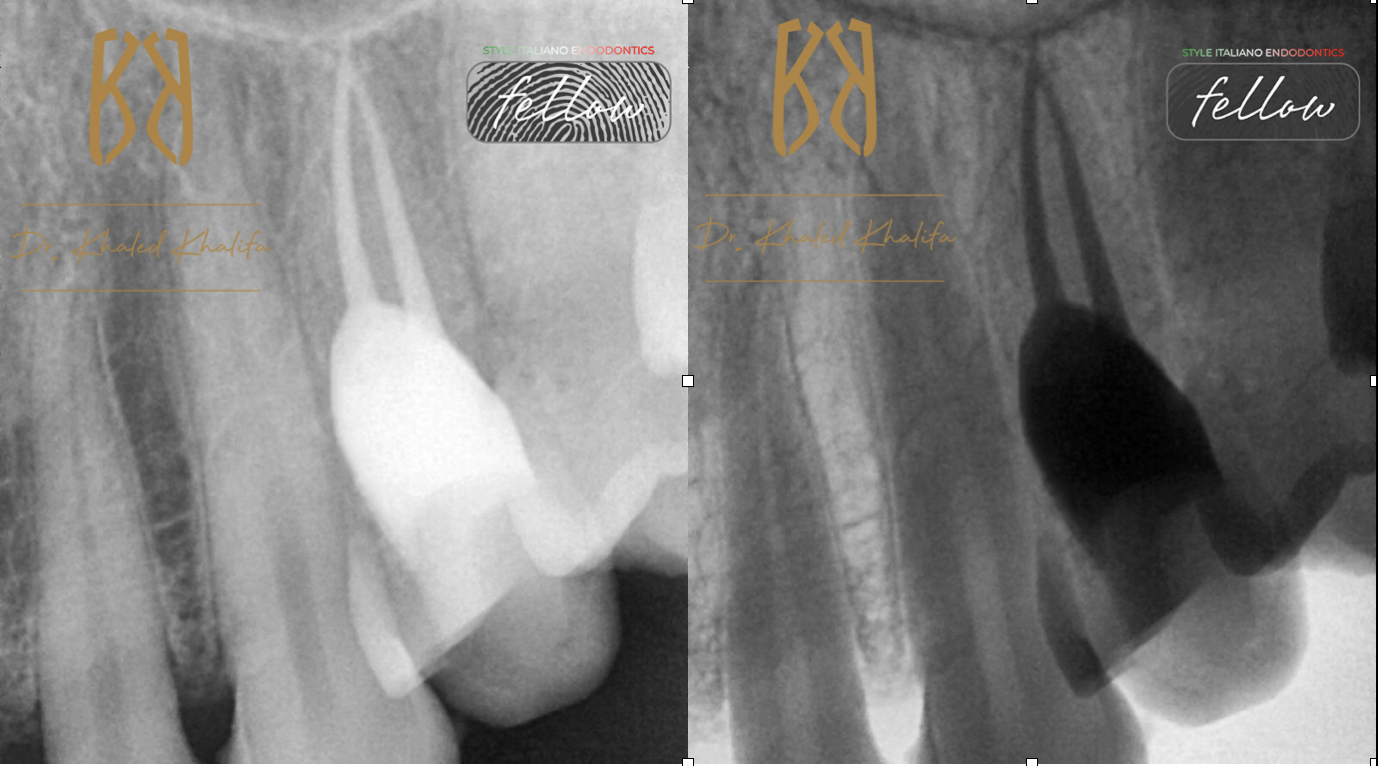
Fig. 7
Post operative X-ray shows very successful and promising treatment and complete adaptation of bioceramic putty in all spaces previously occupied by internal resorptive tissues.

Fig. 8
About the author:
Dr Khaled Khalifa
Endodontic Specialist
Course Director “The Endo Formula”
Endodontic Consultant in multiple private clinics
Member of The Royal College of Surgeons England (MJDF)
Member of The American Association Of Endodontics (AAE)
Member of British Association Of Endodontics (BES)
Practice limited to Endodontics
Conclusions
Internal resorption is a condition that requires a specialist to treat in order to handle such cases and do it properly without complicating it.
Skills, knowledge and armamentarium are essential to treat such cases.
Bibliography
Internal Root Resorption: A Review
Shanon Patel, BDS, MSc, MClinDent Domenico Ricucci, MD, DDS
Conor Durak, BDSc, MFDS RCS (Eng) Franklin Tay, BDSc (Hons), PhD
Published:May 20, 2010DOI:https://doi.org/10.1016/j.joen.2010.03.014
Repair of perforations with MTA: clinical applications and mechanisms of action
THOMAS CLAUDER, SU-JUNG SHIN
First published: 19 February 2009
https://doi.org/10.1111/j.1601-1546.2009.00242.x
Internal resorption in human teeth—a histological, scanning electron microscopic, and enzyme histochemical study
Cecilia Wedenberg, DDS 1
Lars Zetterqvist, DDS 1
Show footnotes
DOI:https://doi.org/10.1016/S0099-2399(87)80041-9