The broken file to retrieve or to leave ?
21/08/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Endodontic cases involving broken instruments are among the most challenging and stressful in the field. Even the top experienced endodontists will agree that removing broken tools demands unwavering calm and exceptional self-control. This procedure isn't for everyone, as a rushed decision or improper removal can lead to failure. It's important to remember that any attempt to extract a broken instrument from the canal carries a high risk of complications, including re-separation, perforation, ledging, loss of canal patency, overheating of periradicular tissues leading to necrosis, or even the transport of fragments into the maxillary sinus or inferior alveolar nerve. When faced with a broken instrument, the clinician has three options if the tooth is to be preserved:remove the instrument, perform a bypass, take no immediate action and continue monitoring the case.The cases discussed required a thorough radiological analysis using CBCT scans and meticulous treatment planning. Only after a precise evaluation of the canal system was an attempt made to remove the broken instrument fragments, as the anatomical conditions were favorable for success. If the conditions had been less favorable, bypassing would have been considered instead. Each attempt to remove an instrument carried the risk of endodontic complications, and in the first case, even the potential for ENT complications. Every case involving a broken instrument must be assessed individually, with a careful evaluation of the real risks associated with removing the fragment and the likelihood of long-term success in preserving the tooth's function within the mouth.To remove a broken file, we can use the ultrasonic (US) technique or a combination of the US and loop techniques. The loop technique is preferable in cases when the broken file length is more than 4,5 mm, or a separated instrument is engaged in the root canal. The following case with a broken file was managed by a combination of US and loop techniques.
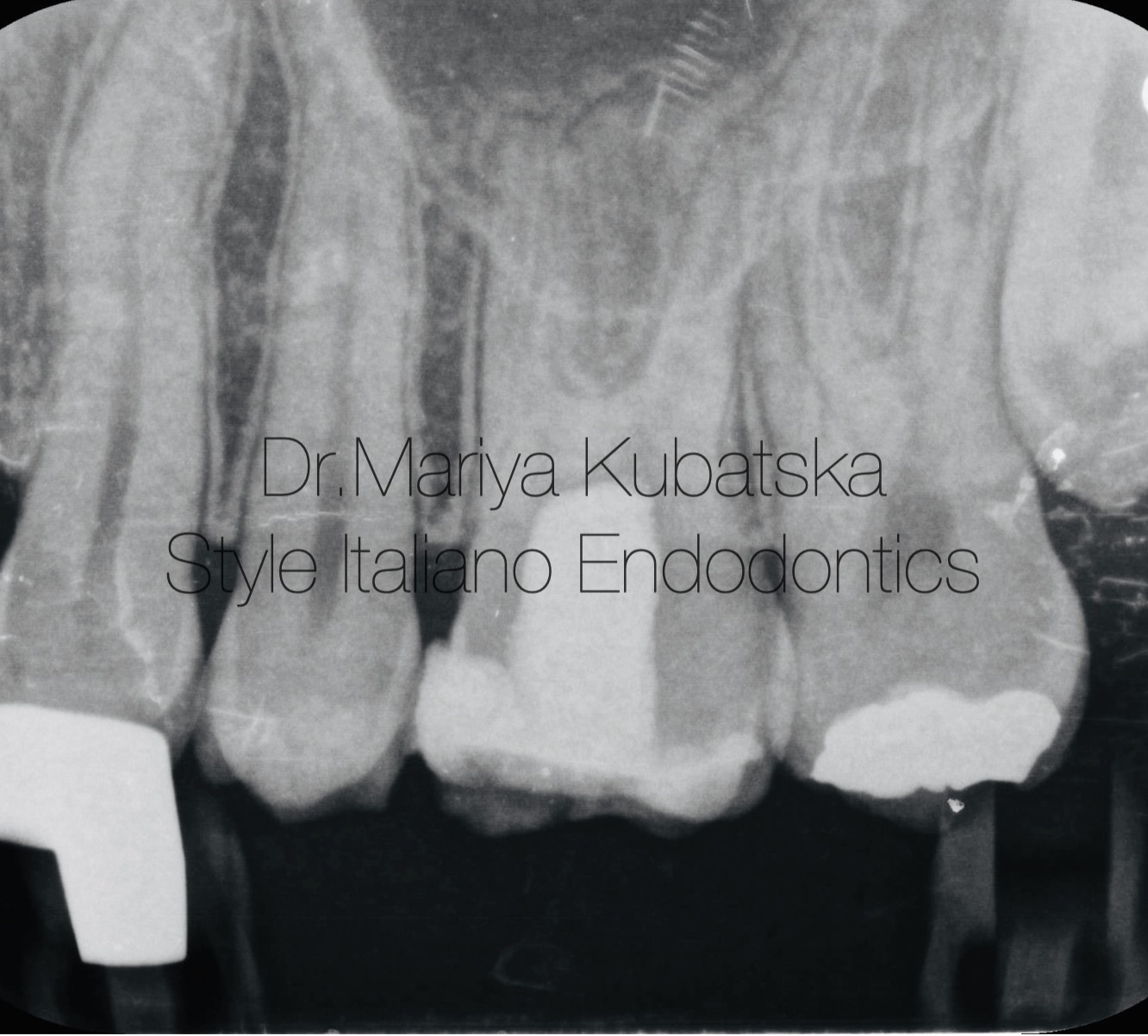
Fig. 1
A 30-year-old patient was referred to me. The referral dentist informed about the separation of the mechanical instruments while performing a root canal treatment in tooth 26 . During the clinical examination, temporary filling IRM was detected. No signs of crack or fracture. The probing depth was no more than 3 mm. No pain on percussion or palpation. No mobility.Pulp status: Necrosis. Diagnosis: Asymptomatic apical periodontitis. The pre-op RVG examination showed a separate file in the apical part of a palatal root canal, and the length of the file was 4 mm. Due to the short length of the palatal root canal, 15 mm, the decision was made to remove the instrument. On account of the instrument being engaged in a root canal was, the combined technique of US + loop to remove the broken file.
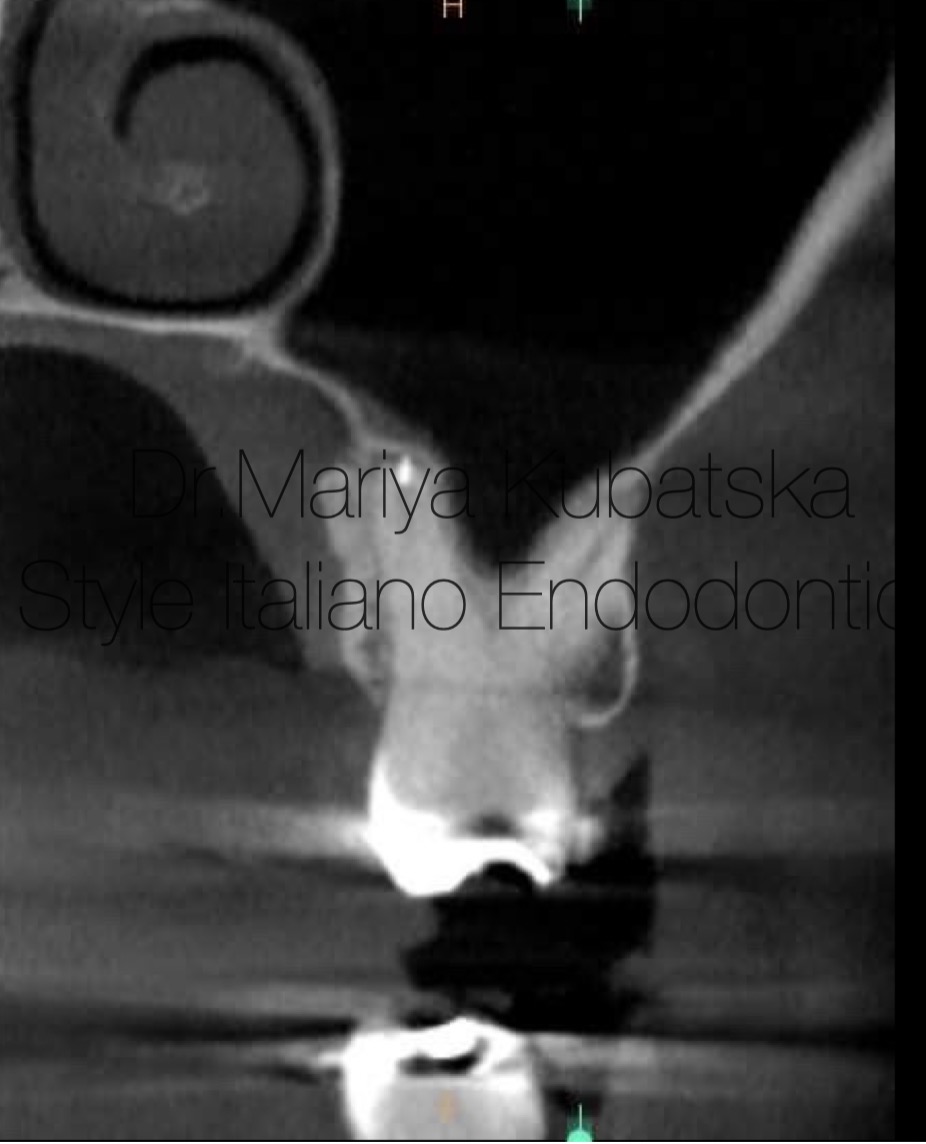
Fig. 2
CBCT was taken to locate the exact position of the separated file and the position of the palatal root relative to the maxillary sinus. On pre-op CBCT, the axial slice , the broken file, was located in the apical part of a palatal root canal, and the length of the separated file was approximately 4 mm.
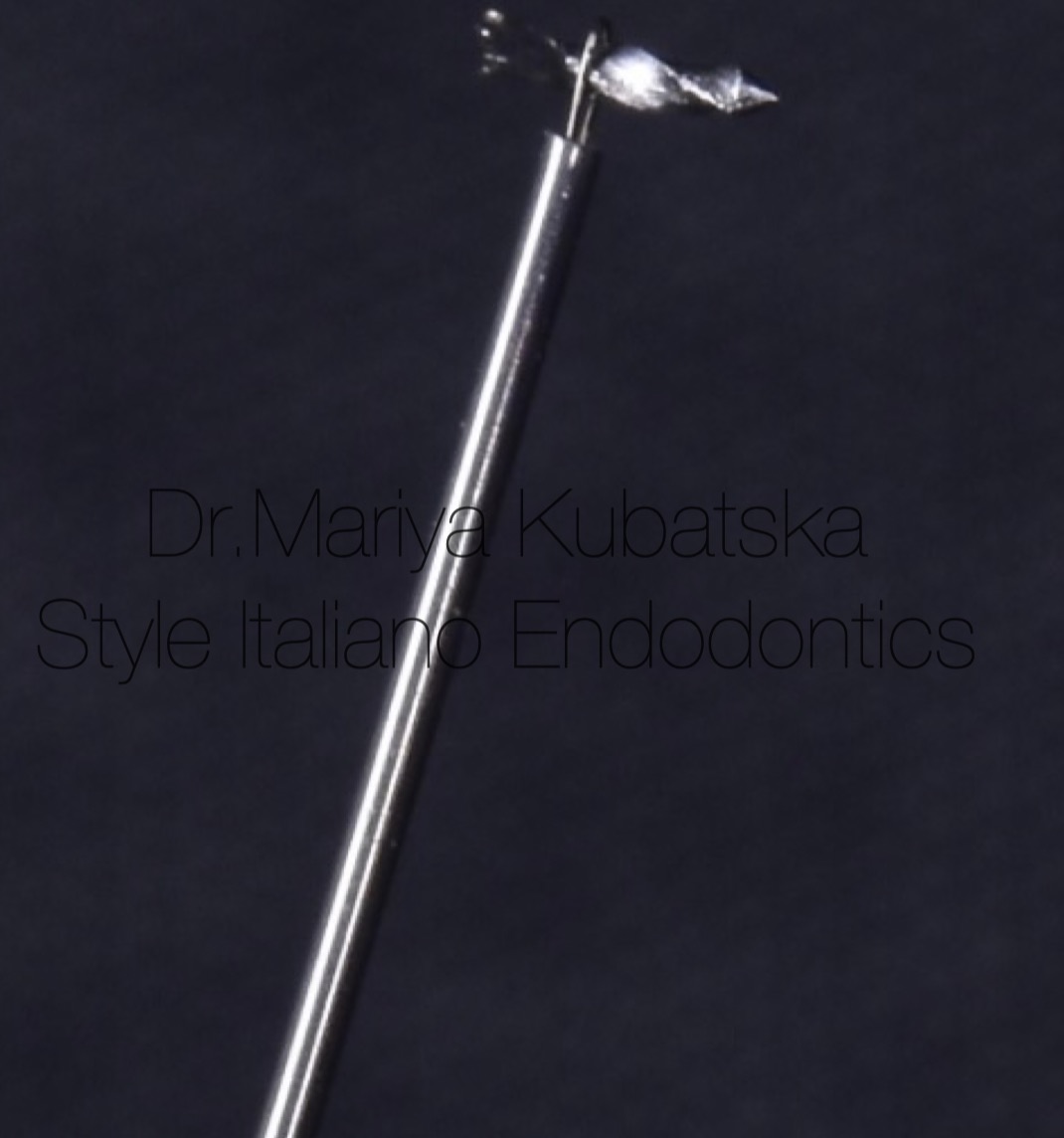
Fig. 3
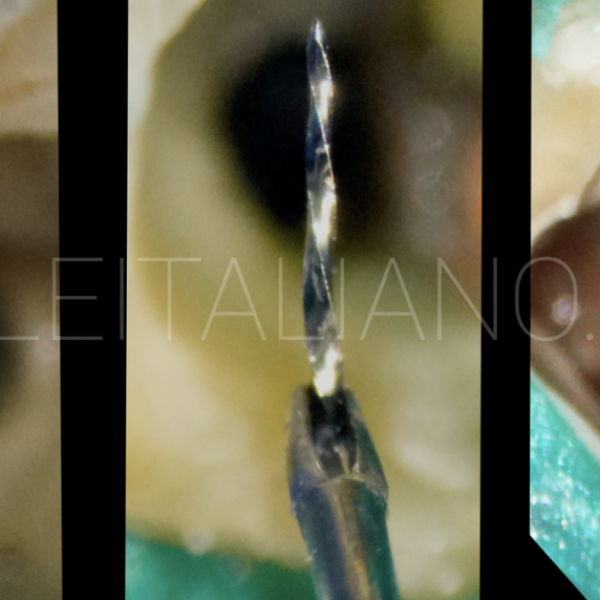
Photo of broken file removed with the usage of the loop technique

Fig. 4
Control x-ray after broken file removal

Fig. 5
The appearance of the pulp chamber after the phases of shaping and cleaning.
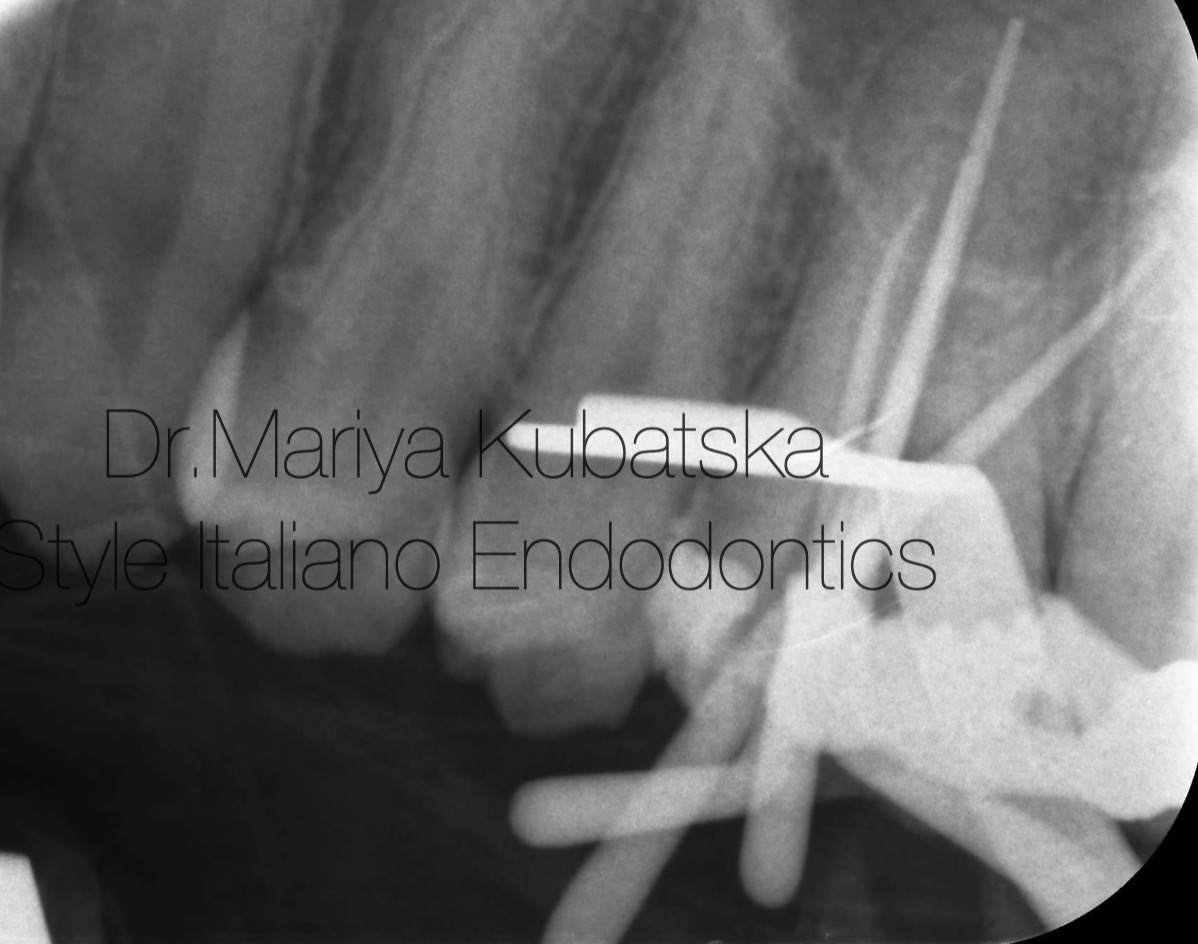
Fig. 6
Intra-op X-ray with gutta-percha points showed the correct working length in all root canals.

Fig. 7
Post-operative x-ray. Obturation was made with epoxy sealer and gutta-percha by using a continuous wave technique
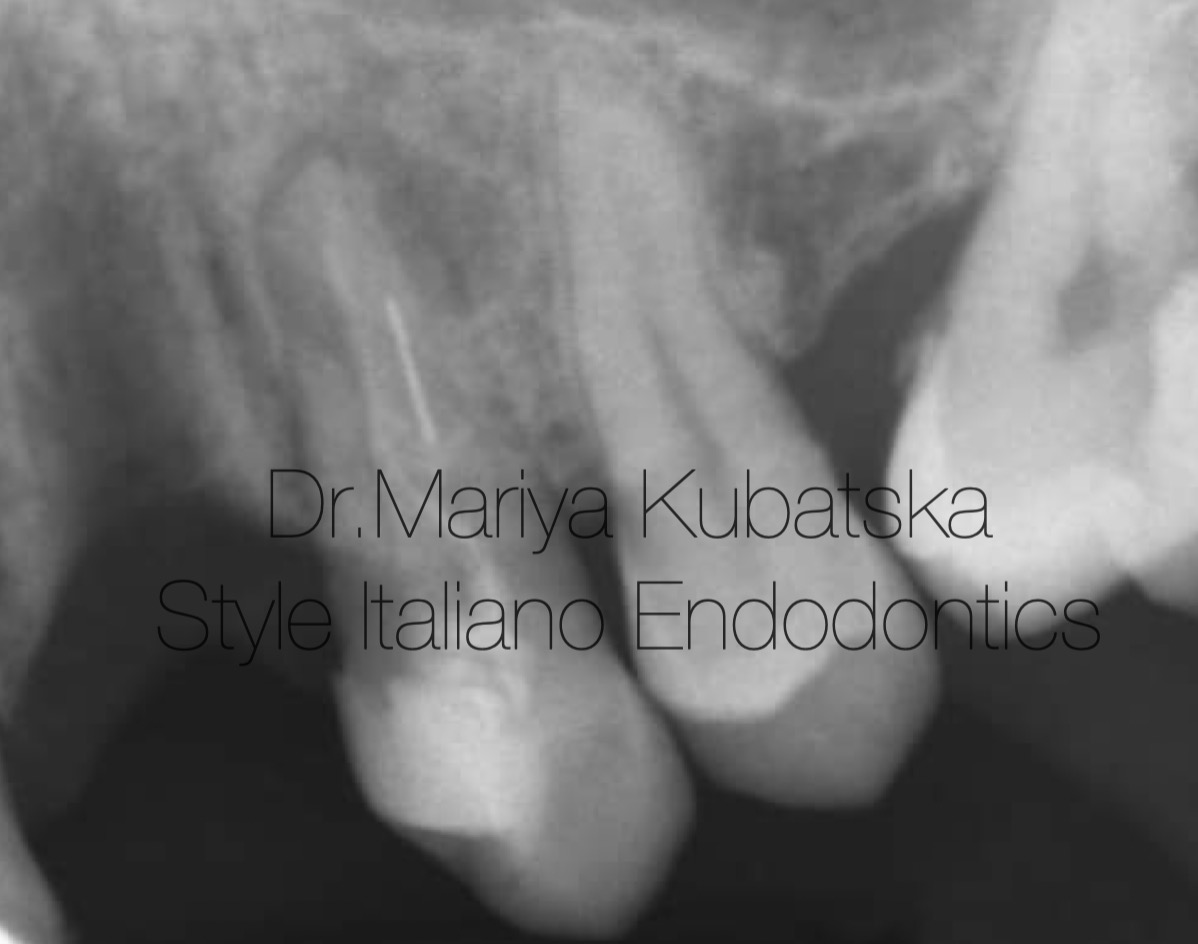
Fig. 8
A 50-year-old patient was referred to me by my colleague. The referral dentist informed me about the separation of the mechanical instruments while performing a root canal treatment in tooth 24. The referral dentist attempted to remove the broken file that caused the apical displacement of the instrument. During the clinical examination, temporary filling IRM was detected. No signs of crack or fracture. The probing depth was no more than 3 mm. No pain on percussion or palpation. No mobility.Pulp status: Necrosis. Diagnosis: Asymptomatic apical periodontitis. The pre-op RVG examination showed a separate file in the middle part of the palate root canal.
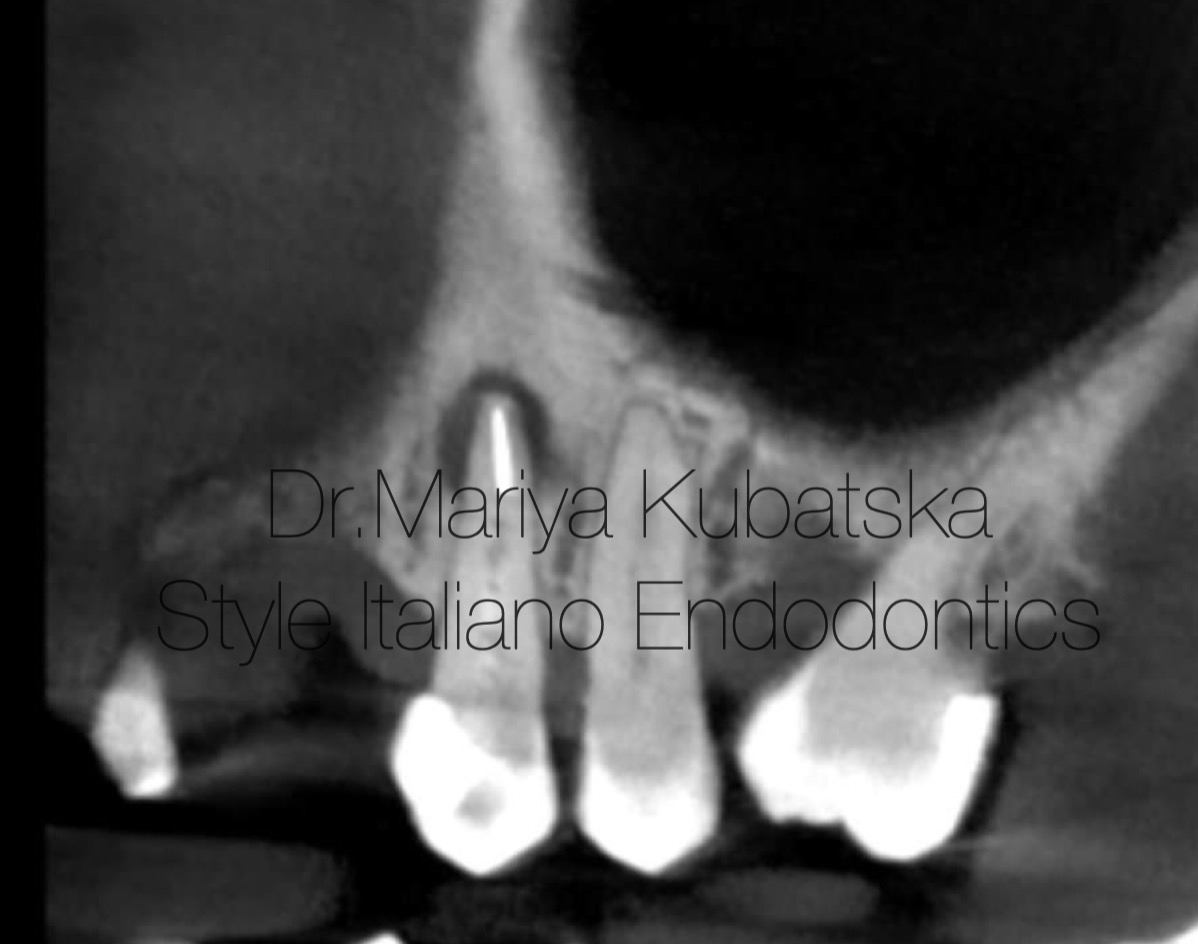
Fig. 9
CBCT was taken to locate the exact position of the separated file.
On pre-op CBCT, the frontal slice, separated instrument was located in the apical part of the palatal root canal of tooth 24. Also was a present apical lesion.

Fig. 10
On account of the instrument being lodged in the root canal, a combined technique of ultrasonic activation and a loop was used to remove the broken file. X-ray shows a loosened instrument after using the US technique.
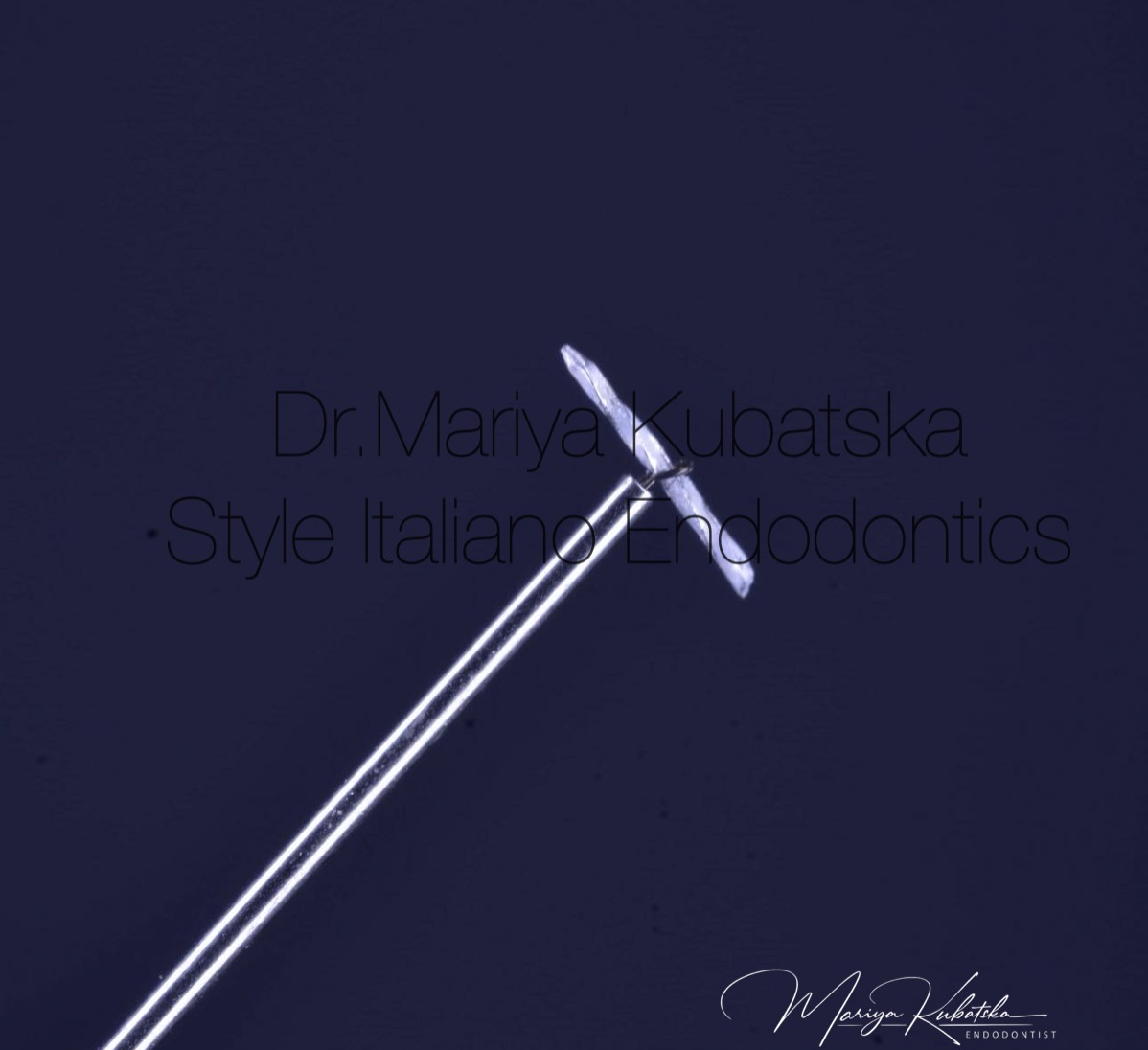
Fig. 11
Photo of broken file removed with the usage of the loop technique
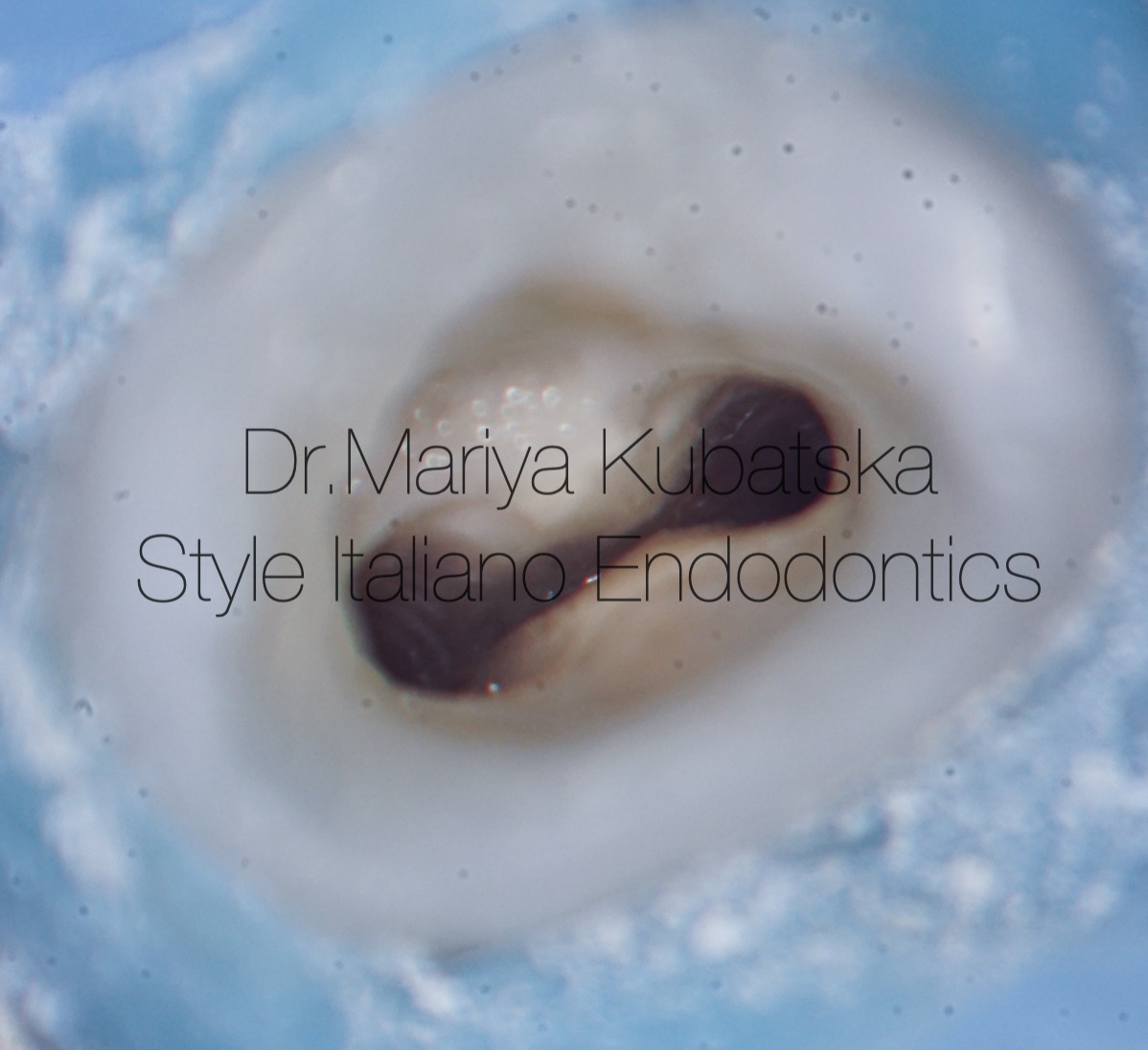
Fig. 12
The appearance of the pulp chamber after the phases of shaping and cleaning.

Fig. 13
An intra-op X-ray with gutta-percha points after instrument removal showed the correct working length in all root canals.
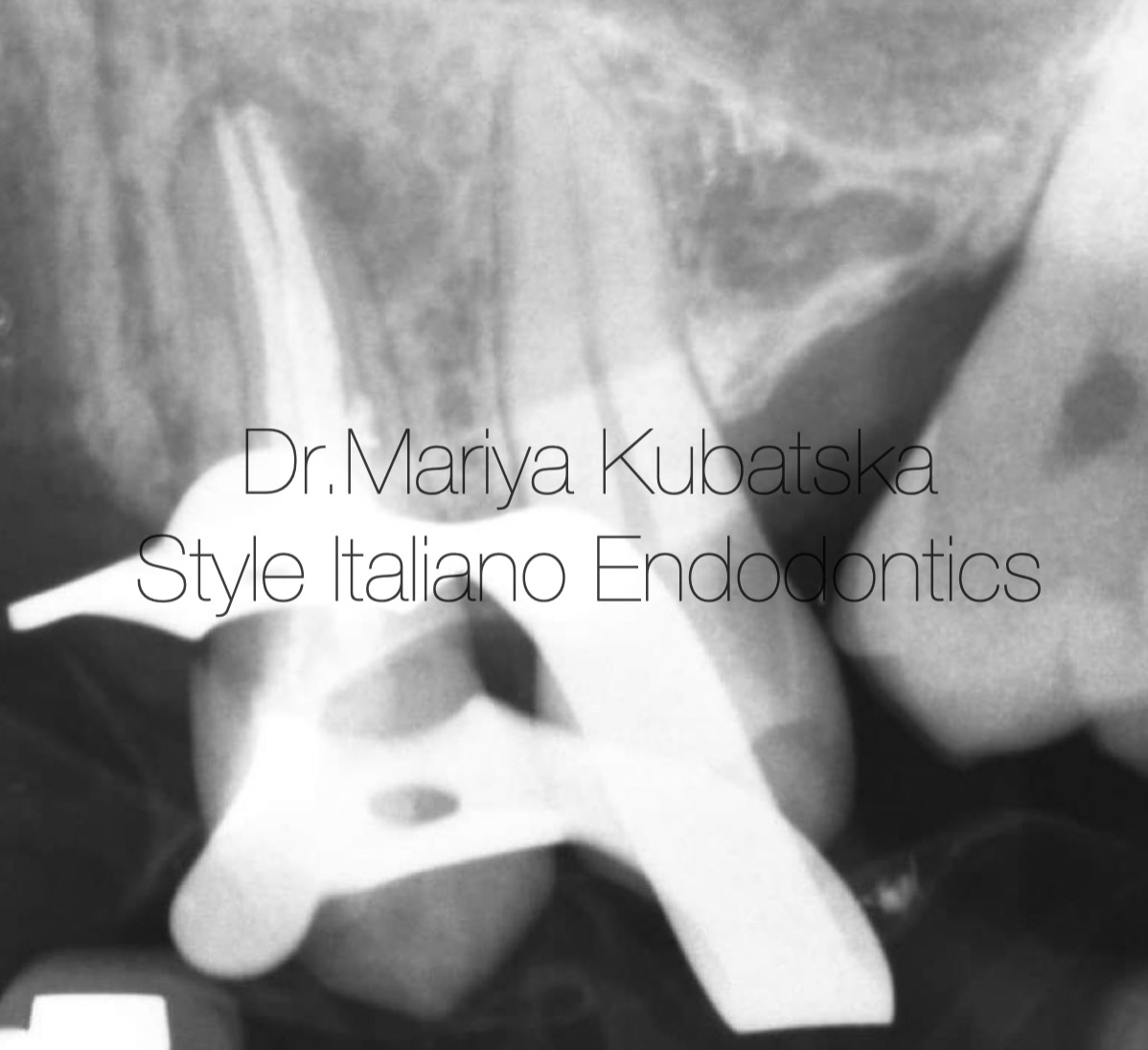
Fig. 14
Post-operative x-ray. Obturation was made with epoxy sealer and gutta-percha by using a continuous wave technique
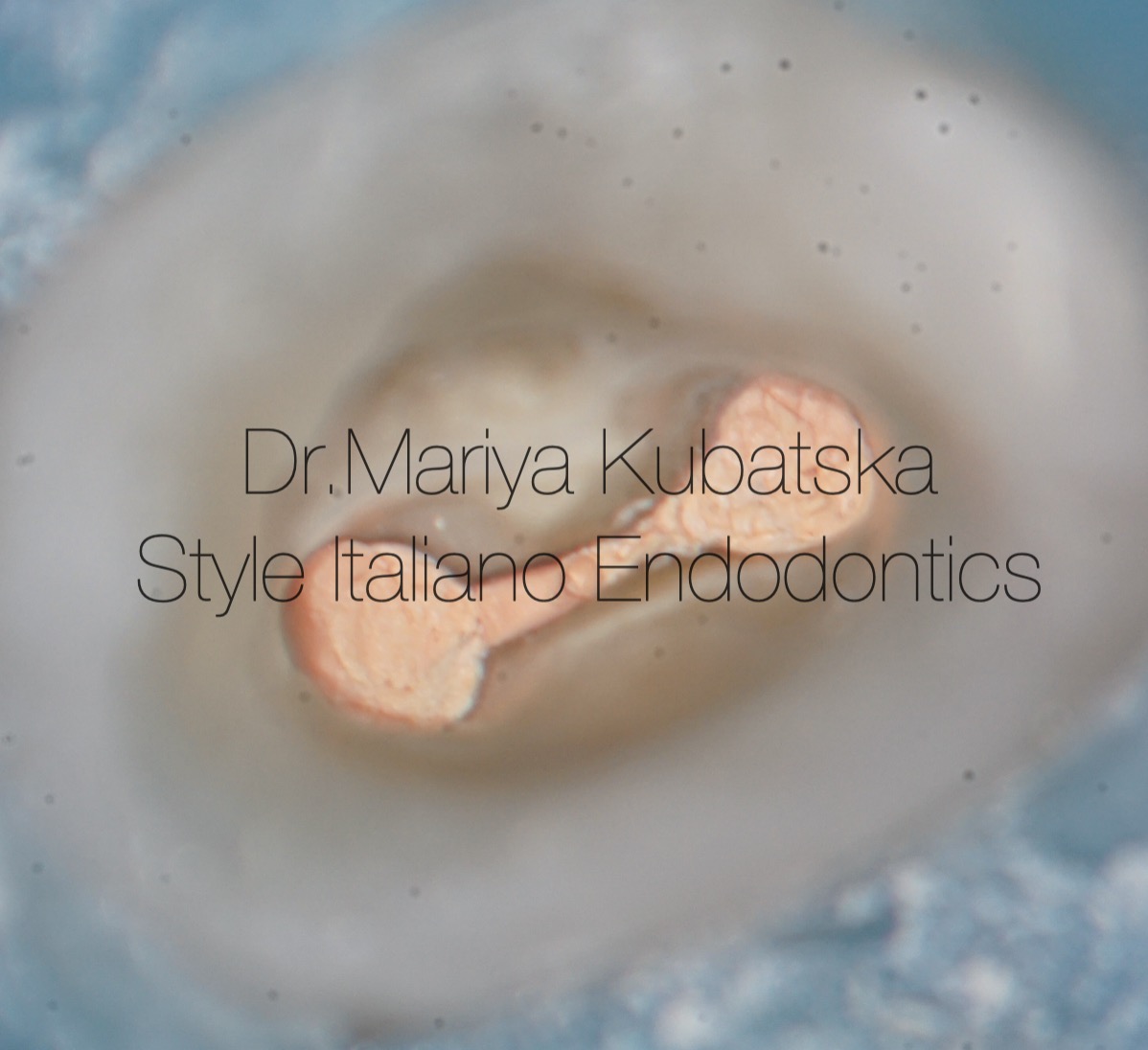
Fig. 15
The appearance of the pulp chamber after obturation of root canals

Fig. 16
Mariya Kubatska graduated medical university of Gdansk in 2014. Since graduation, I have been highly interested in Endodontics. Member of the European Society of Endodontology, the American Association of Endodontists, the Polish Endodontic Association, and the Department of Endodontology of the Polish Dental Society. Since 2023, Style Italiano Endodontics fellow. International speaker. Lecturer in Esdent and MCS Karas Dental Training centers. Author of case reports in Polish dental magazines. Since 2018, Mariya has worked in Oslo, Norway, focusing on endodontics, in private life piano lover.
Conclusions
Endodontic cases involving broken instruments present significant challenges and require a high degree of skill and composure from the clinician. The process of removing broken tools demands careful consideration and precise execution to avoid severe complications such as re-separation, perforation, or damage to adjacent structures. The clinician must evaluate each case individually, weighing the risks of instrument removal against the potential benefits of preserving the tooth. Advances in technology, including the use of ultrasonic techniques and loop devices, have improved the predictability and effectiveness of broken file removal. In the cases discussed, thorough radiological analysis and meticulous planning were crucial in determining the most appropriate approach.
Bibliography
1.-Suter B, Lussi A, Sequeira P. Probability of removing fractured instruments from root canals. Int Endod J 2005; 38: 112123
2.-Yoshi Terauchi , Christopher Sexton, Leif.K.Bakland .Factors Affecting the Removal Time of Separated Instruments
3.-Shahabinejad H, Ghassemi A, Pishbin L, Shahravan A. Success of ultrasonic technique in removing fractured rotary nickel-titanium endodontic instruments from root canals and its effect on the required force for root fracture. J Endod. 2013;39(6):824–8.
4.-Ruddle CJ: Ch. 25, Nonsurgical endodontic retreatment. In Pathways of the Pulp, 8th ed., Cohen S, Burns RC, eds., St. Louis: Mosby, pp. 875-929, 2002
5-Madarati AA, Hunter MJ, Dummer PM. Management of intracanal separated instruments. J Endod. 2013 May;39(5):569-81. doi: 10.1016/j.joen.2012.12.033. Epub 2013 Mar 15. PMID: 23611371.