Single Cone Obturation: Mastering The Technique with Bioceramic sealers
15/06/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The final objective of endodontic treatment as described by Schilder in 1967 is ‘‘the total obturation of the root canal space’’ and since then many materials and techniques have been developed for obturating the radicular system (1). In the last decade, the development of bioceramic or calcium silicate-based (CSB) sealers has led to the re-introduction of a simplified obturation approach called the ‘single cone (SC) technique’. CSB sealers do not shrink and are insoluble in tissue fluids, thus they have changed the obturation principle that the sealer should be as thin as possible in order for the radicular space to be occupied by the core material. In the SC technique, the flowable CSB sealer is the main component of the root filling and a single gutta-percha (GP) point of appropriate size and taper is used to deliver the sealer through hydraulic condensation into the irregularities of the root canal space (2-5). The SC technique with CSB sealers is as effective as the conventional obturation techniques, so it’s up to the clinician to decide which obturation technique is suitable for each clinical case.

Fig. 1
Case Selection
The SC technique with CBS sealers outmatches the continuous wave of condensation technique (CWC) in cases of narrow, long and curved canals. In these types of anatomy penetration of the System B plugger 4-5 mm short from the working length (WL) can sometimes be impossible. A more conservative canal preparation can be achieved with the use of SC technique in such cases. In contrast, warm obturation techniques seem to have an overall better obturation quality and a smaller void incidence in oval and wide canals compared to the SC technique. However, similar results in obturation volume can be obtained with the SC and CWC techniques in internal root resorption cavities (6,7). Moreover, in presence of cracks, the SC technique will apply smaller forces into the canal than the CWC technique.
In the preoperative x-ray a case with appropriate characteristics for the use of the SC technique is depicted: A 16 year old Greek female patient with symptomatic apical periodontitis in tooth #36 with long (27mm), narrow roots and hypotaurodontism.

Fig. 2
Final Irrigation Protocol
CSB sealers need an aqueous environment for the initiation of their setting process, but also for the activation of their biological properties. The degree of residual humidity inside the root canal does not seem to affect automixed and powder/liquid formulations CSB sealers, but single syringe (premixed) sealers need dentinal tubule moisture to harden. Consequently, irrigant - CBS sealers interactions are important as they will change the dentinal microstructure and the sealer properties. These interactions still remain unclear, but the following recommendations can be found in the literature (2-5,8,9) :
- EDTA irrigation for the smear layer removal is mandatory for single syringe sealers as they need the dentinal fluid to set.
- CHX improves the antimicrobial effect but also causes modifications to the physical properties of CSB sealers.
- Phosphate-buffered saline compromises the antimicrobial effect of CSB sealers.
- A final rinse with ethanol is contra-indicated as it will cause intracanal dentin desiccation.
- A final rinse with sterile water can be used to remove the last irrigant before root canal drying.

Fig. 3
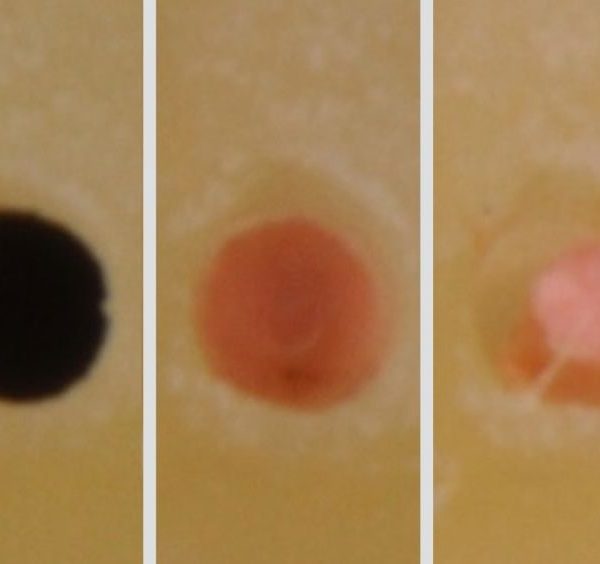
Root Canal Drying Technique
Although CSB sealers need moisture as forementioned, blood and tissue fluids seem to negatively influence their setting. In addition, the presence of blood also reduces their antimicrobial properties, therefore the root canal should be clean without any blood before obturation. The exact degree of moisture at the time of obturation and the method to achieve it is never mentioned by the manufacturers. Intracanal dentin desiccation should be avoided. Older studies reported that the canal should be slightly wet and recommended the use of fewer paper points or intracanal micro-suction/Luer Vacuum Adapter and then one sterile paper point before obturation. However, a recent review concluded that the canals should be completely dry at the time of obturation. Further research on this subject is needed.

Fig. 4
Type of Gutta-Percha
Some manufacturers suggest that bioceramic‑coated (BC) GP points are bonding with CBS sealers resulting in a uniform 3D obturation within the root canal. Depending on the type and the chemical composition of the GP a different interface might be created between the GP point and the CSB sealer. However, there is lack of scientific evidence supporting the use of CBS sealers with BC GP points, so any type of GP can be used with the CBS sealer based SC technique.
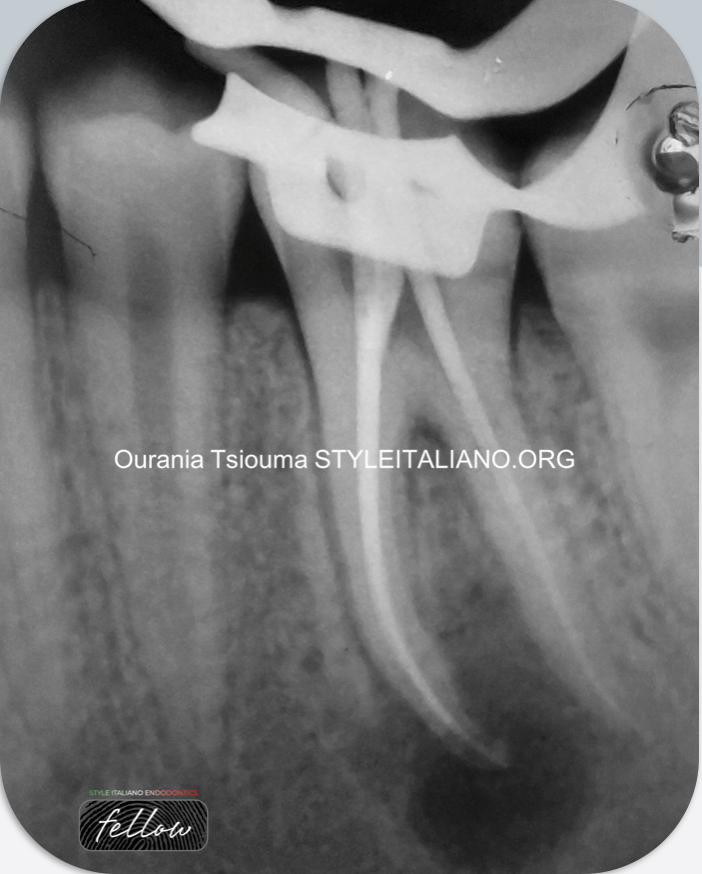
Fig. 5
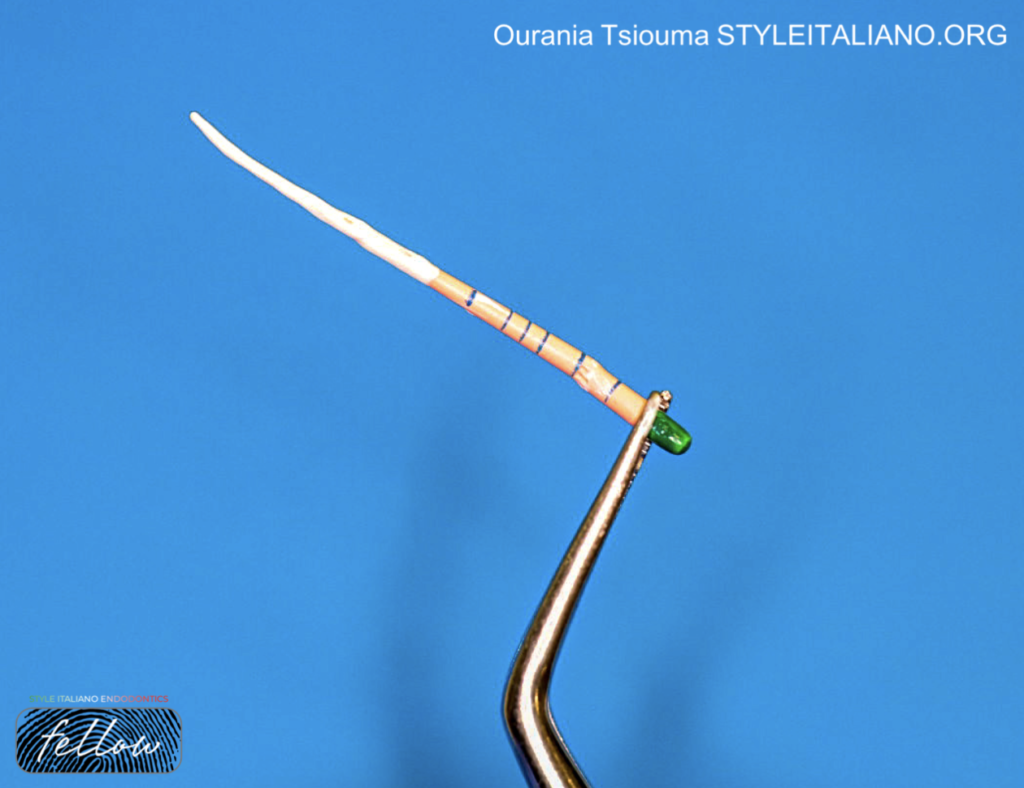
Cone Fit
The master cone in the SC technique should have the same size and taper as the last shaping instrument. A master GP point should be selected according to the article about cone fit. http://styleitaliano.hime.host/obturation-step-no-1-cone-fit.

Fig. 6
Sealer Delivery Methods
Several methods have been proposed for the delivery and distribution of CBS sealers:
- Coating the master cone or a hand file (same size as the last shaping instrument) with the CSB sealer followed by its slow insertion to the full WL or close to the WL respectively. This approach might be insufficient in oval or wide canals.
- Plastic carrier and Modified Irriflex Needle technique according to https://endodontics.styleitaliano.org/bioceramic-sealers-application-the-ultimate-guide/.
- Special rotary endodontic instrument usage like a Lentulo spiral at low speed (around 700–800 rpm) up to 2 mm short of the WL. The procedure is done until the CBS sealer is visible at the canal orifice.
- The technique that is mostly recommended in the literature is the injection of the sealer into the canal with a flexible cannula capillary tip connected to the syringe. The sequence of this technique will be described below:

Fig. 7
The first step is to check the sealer extrusion on the rubber dam, otherwise air/gas can be introduced to soft tissue spaces from the applicator tip through the root canal.

Fig. 8
The syringe tip is then placed in the canal at the level of the coronal or middle third. It is recommended to supply the applicator tip with a rubber stop approximately 5-6mm from the predetermined WL.

Fig. 9
A small amount of the product is smoothly injected into the root canal by gently pressing the plunger of the syringe and withdrawing the tip till the sealer is visible at the root canal orifice. Sonic, ultrasonics and other sealer activation procedures may also facilitate CSB sealer distribution.

Fig. 10
After Sealer Delivery
The tip of the master GP cone is coated with the CBS sealer, followed by its insertion into the root canal up to the WL. Insertion of the GP point should be done slowly (3-5 sec) to avoid sealer extrusion into the periapical tissues and void formation into the sealer mass. In addition, the slow insertion of the GP cone will prevent sealer accumulation under the GP preventing it from reaching the full WL. If the GP point cannot reach the full WL, the sealer must be removed with a hand or rotary instrument and then the process is repeated. It should be noted, that if a retreatment is needed and there is only CSB sealer at the apical portion of the root canal filling then the patency will be difficult or even impossible to be achieved, due to the CBS sealer’s hardness and penetration into the dentinal tubules.
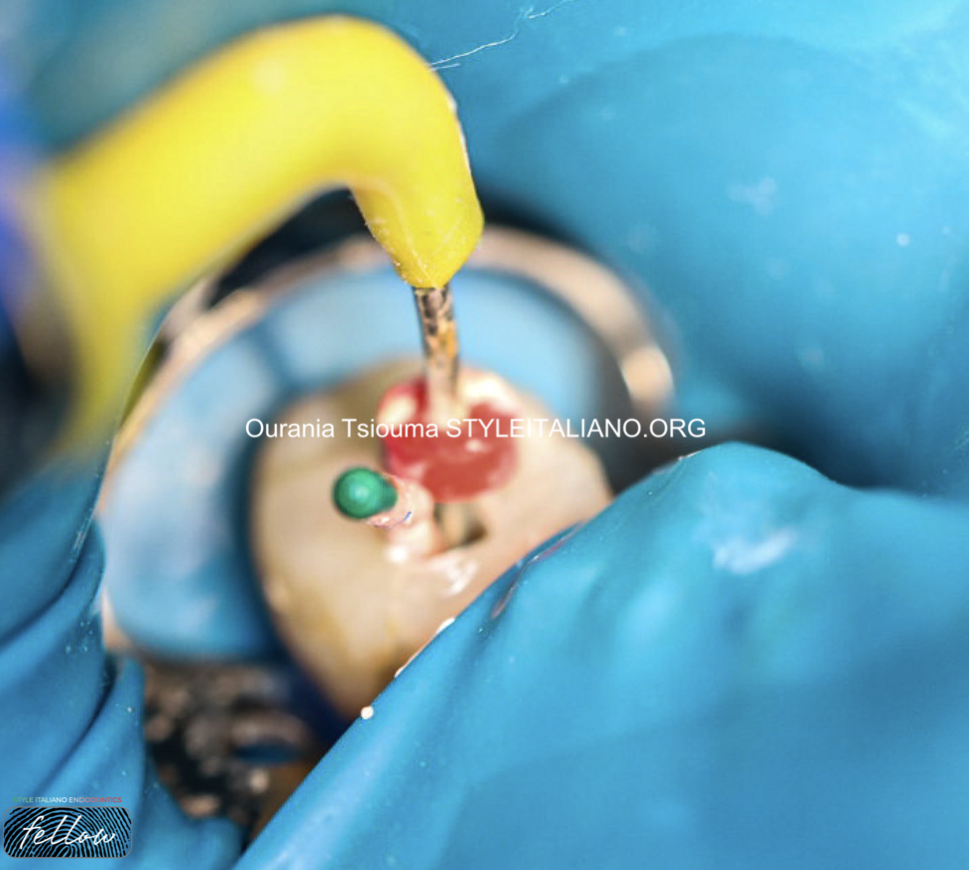
Fig. 11
In oval and wide root canals auxiliary GP points can be passively inserted with no compaction along the master GP cone. The tip of an activated System B plugger or a hot instrument is then used to sear the master GP cone and the auxiliary GP points at the CEJ in single rooted teeth or at the orifice level in multi-rooted teeth.

Fig. 12
A wide plugger is utilized to vertically condense the remaining GP at the orifice by applying apical pressure on the warm GP as it cools.
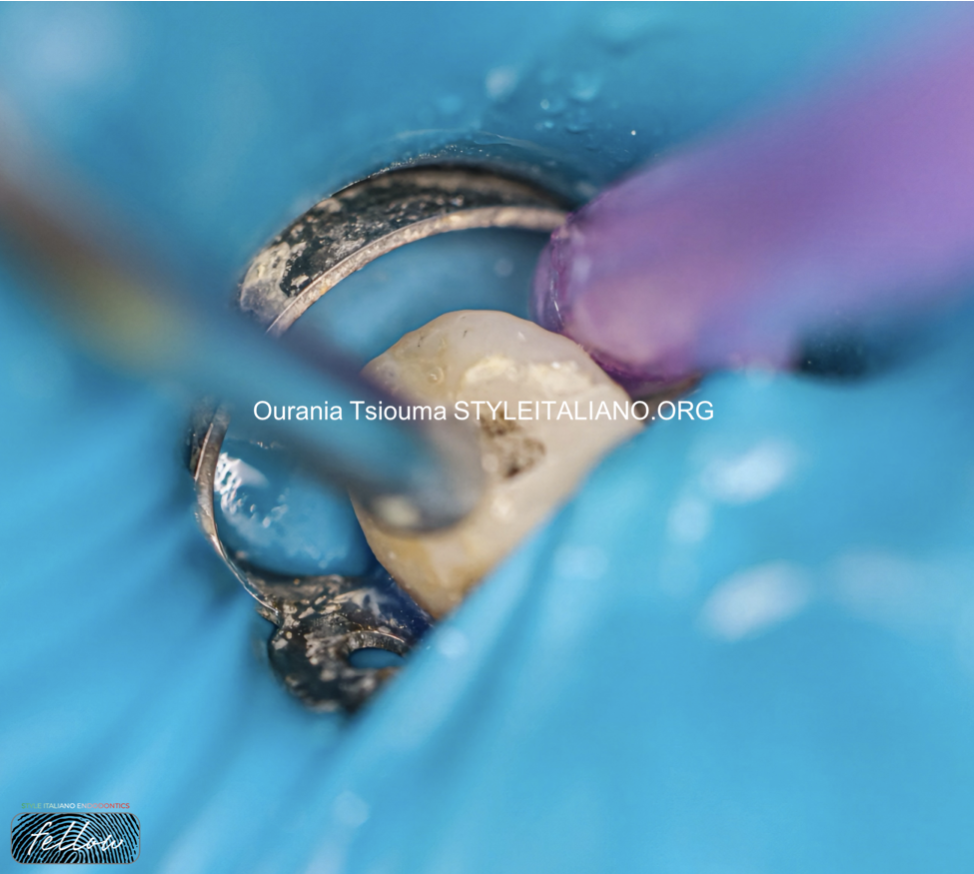
Fig. 13
When the obturation of all the canals is finished, sealer remnants are cleaned with an air/water spray or a wet cotton pellet from the access cavity.

Fig. 14
End Of Treatment
The postoperative radiographic x-ray of cases obturated with the SC technique is similar to the ones obturated with the CWC technique.

Fig. 15
About The Author:
Ourania Tsiouma
-2016: Award of Excellence in the Physiology course from the Laboratory of Experimental Physiology, Medical School, National and Kapodistrian University of Athens.
-2015-2019: <<Antonios Papadakis>> scholarship holder during her undergraduate studies.
-2019: 1st "Ioannis Karkatzoulis" Prize for the best Oral Presentation in the 19th Pampeloponnesian Dental Congress.
-2020: Graduated second with honours from the Dental School of the National and Kapodistian University of Athens, Greece.
-2020–2022: Research Associate in the Department of Endodontics, Dental School, University of Athens.
-2023: Master in Clinical and Surgical Microendodontics, University of Turin, Italy.
-Author of scientific articles published in national and international peer-reviewed journals.
-Fellow Member of Style Italiano Endodontics.
-Private practice focused on Endodontics and Restorative Dentistry in Athens, Greece.
Conclusions
The SC obturation in conjunction with CSB sealers is a quick and simplified technique that does not require a long learning curve, expensive armamentarium, and significant clinical experience, characteristics that make it rapidly appealing among general dentists and endodontists. However, the usual endodontic protocol has to be slightly revised by the practitioners, for the best clinical outcome to be achieved.
Bibliography
- Schilder H. Filling the root canal in three dimensions. Dent Clin North Am.1967;November:723–44.
- Trope, M.; Bunes, A.; Debelian, G. Root filling materials and techniques: Bioceramics a new hope? Endod. Top. 2015; 32, 86–96.
- Debelian G, Trope M. The use of premixed bioceramic materials in endodontics. G Ital Endod. 2016; 30: 70–80.
- Drukteinis S. Root canal obturation techniques with hydraulic calcium silicate-based materials. Clin Dent Rev. 2021; 5, 22.
- Drukteinis S. Hydraulic calcium silicate-based materials for root canal obturation. Clin Dent Rev. 2022; 6, 1.
- Sharki AM, Ali AH. Three-Dimensional Measurement of Obturation Quality of Bioceramic Materials in Filling Artificial Internal Root Resorption Cavities Using Different Obturation Techniques: An In Vitro Comparative Study. J Endod. 2024; Apr 7:S0099-2399(24)00226-7.
- Yazdi KA, Aminsobhani M, Alemi P. Comparing the Ability of Different Materials and Techniques in Filling Artificial Internal Resorption Cavities. Eur Endod J. 2018 Dec 13;4(1):21-27.
- Sfeir G, Zogheib C, Patel S, Giraud T, Nagendrababu V, Bukiet F. Calcium Silicate-Based Root Canal Sealers: A Narrative Review and Clinical Perspectives. Materials (Basel). 2021 Jul 15;14(14):3965. doi: 10.3390/ma14143965. PMID: 34300886; PMCID: PMC8306764.
- Cardinali F, Camilleri J. A critical review of the material properties guiding the clinician's choice of root canal sealers. Clin Oral Investig. 2023 Aug;27(8):4147-4155. doi: 10.1007/s00784-023-05140-w. Epub 2023 Jul 17. PMID: 37460901; PMCID: PMC10415471.