Revive and Shine: Retreaty – The Perfect Partner for Flawless Endodontic Retreatment
05/09/2024
Viresh Chopra
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The success of endodontic treatment hinges on a comprehensive understanding of the root canal system of each tooth, including the potential presence of extra canals. Essential to the success of endodontic therapy are thorough cleaning, shaping, and obturation of the entire root canal system. Therefore, in-depth knowledge of root canal morphology and anticipation of possible variations are crucial to minimizing the risk of endodontic failure.
For successful outcomes, several key parameters must be adhered to: accurate diagnosis, effective isolation of the operating field, complete chemo-mechanical preparation of the intricate endodontic system, and three-dimensional obturation of the root canals, followed by proper post-endodontic restoration. Adhering to these protocols is critical for achieving both short- and long-term success in endodontic treatment. Failure to maintain the integrity of any step within this protocol can result in treatment failure. The preoperative periapical radiograph, despite its two-dimensional nature, plays a vital role in providing preliminary insights into the root canal anatomy that will be encountered.
This case report presents the management of a case of Symptomatic Apical Periodontitis (SAP) with a chronic abscess, associated with a mandibular molar that had undergone a previous root canal treatment with insufficient obturation.
The success of endodontic treatment hinges on a comprehensive understanding of the root canal system of each tooth, including the potential presence of extra canals. Essential to the success of endodontic therapy are thorough cleaning, shaping, and obturation of the entire root canal system. Therefore, in-depth knowledge of root canal morphology and anticipation of possible variations are crucial to minimizing the risk of endodontic failure.
For successful outcomes, several key parameters must be adhered to: accurate diagnosis, effective isolation of the operating field, complete chemo-mechanical preparation of the intricate endodontic system, and three-dimensional obturation of the root canals, followed by proper post-endodontic restoration. Adhering to these protocols is critical for achieving both short- and long-term success in endodontic treatment. Failure to maintain the integrity of any step within this protocol can result in treatment failure. The preoperative periapical radiograph, despite its two-dimensional nature, plays a vital role in providing preliminary insights into the root canal anatomy that will be encountered.
This case report presents the management of a case of Symptomatic Apical Periodontitis (SAP) with a chronic abscess, associated with a mandibular molar that had undergone a previous root canal treatment with insufficient obturation.
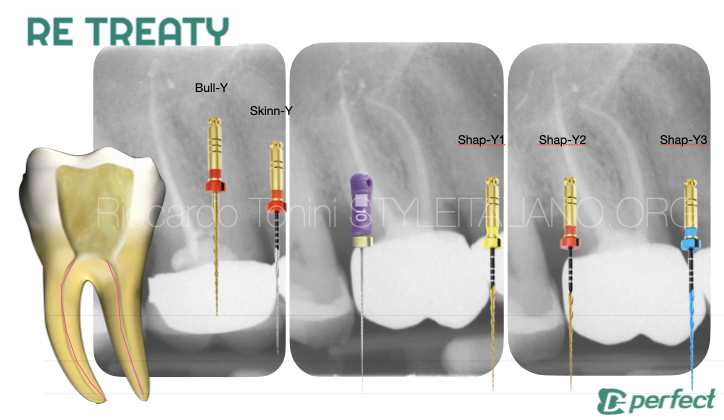
Details about the Retreaty kit
The ReTreaty Kit by Perfectendo, developed in collaboration with Style Italiano Endodontics, is designed to simplify and enhance the predictability of endodontic retreatment procedures. The kit includes five instruments made from three different alloys, utilizing two types of rotary motions. The instruments are named and identified by avatars for easy recognition, eliminating the need for traditional codes or letters.
Key instruments include:
- : A 25/07 file made from gold heat-treated alloy, designed for efficient gutta-percha removal from the coronal third of the canal.
- : The thinnest yet robust file in the kit, used for removing gutta-percha at mid-root levels.
- : Three files (Shap-Y1, Shap-Y2, and Shap-Y3) with varying dimensions and heat treatments, designed to reshape the canal conservatively without altering its original anatomy. The Shap-Y3, in particular, is used for final shaping of the apical region.
The ReTreaty Kit's design emphasizes minimal invasiveness while ensuring thorough cleaning and shaping of the root canals, making it a reliable choice for modern endodontic retreatments
Treatment plan:
Confirm the diagnosis of the mandibular molar requiring retreatment through clinical examination and radiographic analysis.
Evaluate the existing root canal filling material and assess the anatomy for any untreated or missed canals.
Achieve proper isolation of the tooth using a rubber dam to maintain a clean and dry working field.
Re-access the pulp chamber and remove any existing restorative material, including the previous root canal filling material.
Locate all canals, ensuring any previously missed canals are identified.
Thoroughly clean and shape all canals, extending to the full working length.
Employ irrigation with appropriate disinfectants (e.g., sodium hypochlorite) to ensure effective debridement of the root canal system.
Perform final irrigation using a sequence of solutions to eradicate any remaining bacteria and dissolve organic debris.
Consider using intracanal medicaments, such as calcium hydroxide, if needed, between appointments to ensure disinfection.
Achieve a three-dimensional obturation of the root canals using an appropriate obturation technique (e.g., cold or warm vertical condensation) to prevent future microbial infiltration.
Ensure that the obturation material reaches the correct working length in all canals.
Place a suitable coronal seal to prevent reinfection and restore the tooth’s structural integrity.
Plan for definitive full coverage restoration (e.g., crown) to protect the tooth from fracture.
Schedule follow-up visits to monitor the healing process and assess the success of the retreatment both clinically and radiographically.

Fig. 1
Description of the case
A 26-year-old female patient presented with a chief complaint of persistent pain while eating, despite having initiated root canal treatment at another dental facility. The patient reported no relief in pain following the initial treatment. Her medical history was non-contributory, and the tooth in question was identified as the left mandibular first molar (Tooth 36).
Clinical Examination Findings:
Tooth 36 was found to be tender to percussion, and an initiated access cavity was observed on the preoperative radiograph. The occlusal surface exhibited temporary filling material. Periodontal probing depths were within normal limits.

Fig. 2
Step wise Treatment provided
An inferior alveolar nerve block, supplemented with buccal infiltration anesthesia, was administered to achieve profound anesthesia. The tooth was then isolated using a rubber dam, and preoperative examination under the microscope was conducted.
- Gutta perchas within the root canal were removed using the Retreaty kit files in sequence specifically made for this purpose.
Profuse irrigation was conducted using 3% sodium hypochlorite to effectively cleanse and disinfect the root canal system (1).

Fig. 3
Step wise Treatment provided
2. Endodontic access was prepared through the existing restoration, and older gutta perchas were located.
3. Gutta perchas within the root canal were removed using the Retreaty kit files in sequence specifically made for this purpose. Fig 4 (Video 1 - 4).
4. Profuse irrigation was conducted using 3% sodium hypochlorite to effectively cleanse and disinfect the root canal system (1).
Root canal re-treatment protocol followed:
Gutta percha were removed using Bully file from prefect endo (video 1). The files is designed to:
- Remove the bulk of GP from the coronal part of root canal.
- Effectively enlarge the coronal position of the root canal so that subsequent files do not have to encounter any stress while entering the root canal.
This file should never be taken to the complete Working length.
Once the GP was removed, 08K and 10K endodontic files were pre-curved and employed to negotiate the calcified canals (2). C+ files were additionally utilized to open the apically calcified segments of the root canals (3). These files were used with passive motion in the presence of irrigants (4). Upon successful negotiation of the calcified sections, the working length was determined using an electronic apex locator (5) and confirmed with a periapical radiograph
Profuse irrigation was performed in between every instrument using 3% sodium hypochlorite for adequate disinfection. The glide path was established using Skinny file.
Profuse irrigation was performed in between every instrument using 3% sodium hypochlorite for adequate disinfection. Ultrasonic activator was also used to activate the irrigant inside the canals (video 6)
The canals were finally shaped using ShapY 1, ShapY 2 file (video 3 and Video 4).
These files were taken to the established WL.
Canal shaping with Shapy 2
Irrigation and activation
Master cone fit was checked clinically as well as radiographically and the canals were prepared for obturation. Obturation was performed using Calcium silicate sealer along with the Gutta percha cones (Fig 3) (video 3). Recommended single cone obturation technique was used with Calcium silicate sealers. The obturation was verified Clinically (video 5) and radiographically

Fig. 4
Radiographic verification of obturation
Conclusions
Endodontic success is contingent upon meticulous care and precision, with the root canal system serving as the foundation for effective treatment. A comprehensive approach involves four critical phases: thorough cleaning, precise shaping, effective disinfection, and achieving a complete three-dimensional obturation.
The success of this process hinges on a deep understanding that each canal within the root canal system requires careful attention. Failure to identify and treat all anatomical variations can leave residual microorganisms, leading to incomplete cleaning and shaping. This oversight can undermine the effectiveness of the initial root canal treatment and contribute to potential treatment failure.
The practice of endodontics blends scientific precision with skilled technique. Success depends on the ability to navigate the complexities of each canal, understanding its unique characteristics and responding accordingly. Mastery over these variations is essential for achieving a comprehensive seal and effective disinfection.
Endodontic retreatment is a critical procedure for addressing persistent or recurrent infection in previously treated teeth. It involves re-evaluating and revisiting the root canal system to rectify shortcomings from the initial treatment, such as missed canals, inadequate cleaning, or suboptimal obturation. Success in retreatment depends on careful diagnosis, thorough removal of the previous filling material, meticulous cleaning and shaping of the canals, and achieving a hermetic seal with proper obturation. By leveraging advancements in endodontic techniques and technology, retreatment can effectively resolve periapical pathology, preserve the natural tooth structure, and restore the tooth's function, offering patients a second chance at a healthy, pain-free dentition.
Bibliography
- Smith R, Jones A, Blackwell A. Techniques for negotiating calcified canals. J Endod. 2015;41(3):245-250.
- Johnson J, Lee W. Apical calcification management with C+ files. Int Endod J. 2018;51(7):732-738.
- Brown P, Green E, Turner R. Endodontic file use with passive irrigation: A clinical study. J Clin Endod. 2019;45(5):500-506.
- Miller T. Electronic apex locators: A review and clinical applications. Dent Today. 2020;39(8):56-60.
- Haapasalo M, Shen Y. Irrigation of the root canal system. In: Hargreaves KM, Berman LH, editors. Cohen's Pathways of the Pulp. 11th ed. St. Louis, MO: Mosby; 2013. p. 299-342.
- Peters OA. Current challenges and concepts in the preparation of root canal systems: A review. J Endod. 2004;30(8):559-67.
- Ruddle CJ. Endodontic canal preparation: Shaping goals and strategies. Dent Clin North Am. 2004;48(1):39-63.
- Dentin AK, Sharma V, Patel MH. Efficiency of novel rotary systems in canal preparation: A review. Int J Dent Med Res. 2020;6(1):34-40.