RETREATY : CONSERVATIVE RETREATMENT FOR UNUSUAL ANATOMY “MB1, MB2, MB3”
23/08/2024
Abdullah AboHalima
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Abiding by the Style Italiano Endodontics philosophy, Retreaty kit allows having a conservative approach in retreatment cases, thanks to 3 different alloys that help managing the cases in feasible, teachable & repeatable way.
There are multiple reasons a primary root canal therapy may be unsuccessful. Before taking on a retreatment case, the clinician must determine if there is an improvement to be made and, thus, a favorable prognosis to be obtained.
Among the reasons initial therapy may have failed include insufficient debridement of tissues, incomplete obturation, missed anatomy, coronal leakage, and/or vertical root fracture.
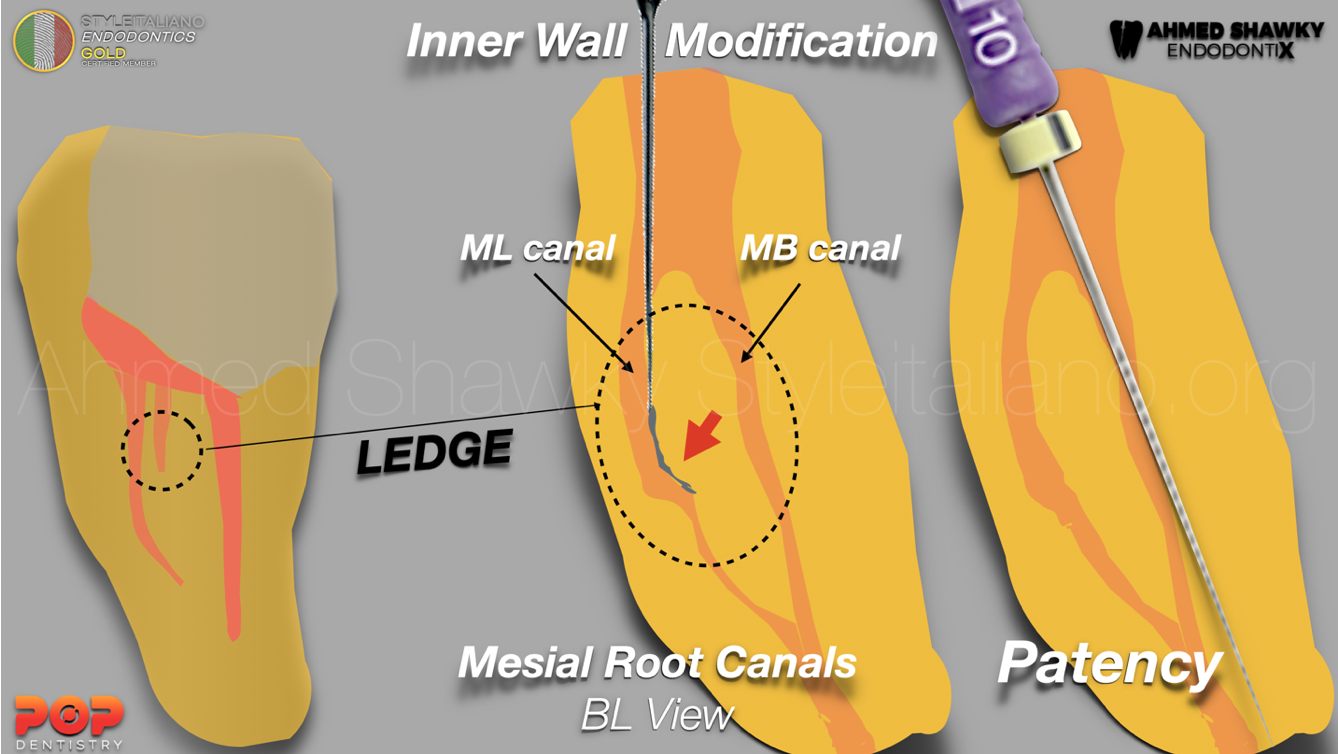
In this case report we will see an unusual anatomy with 3 canals in the mesial root (mb1, mb2 and mb3): during the initial treatment two out of three canals were missed (mb2,mb3), disinfection was insufficient disinfection and and the other canals were under-filled: all these reasons led to the failure of the therapy.
Choosing the right instrument with a proper irrigation protocol and choosing the appropriate obturation technique in each canal will help in getting the most favorable prognosis.
Before any intervention we have to analyze the whole situation using the diagnostic tools of clinical examination and radiographic inspection
This patient came with a previous RCT with an old PFM crown with a huge periapical lesion related to the MB root and palatal root.
Using CBCT radiographic examination it was possible to identify that there was a missed anatomy in the MB root where I found mb2 and mb3 (3 canals) and an under filling in the distal and palatal root as well, so I decided to go for non surgical retreatment.
I started with the coronal disassembly. I sectioned the crown starting from the buccal and palatal aspects and joined the line occlusally. Then I split the crown to assess the restorability after removing any old filling and recurrent caries.
Isolation is always mandatory as the situation is already compromised so perfect isolation without any leakage is highly recommended for a better outcome
Any old restoration (amalgam) was removed, then I made sure I had a caries free zone. Then I used ultrasonic tips to remove the old metal post as a part of the coronal disassembly, and continued using ultrasonics to refine the access cavity. The CBCT confirmed the existence of missed anatomy, so I searched for MB2 and MB3 canals.
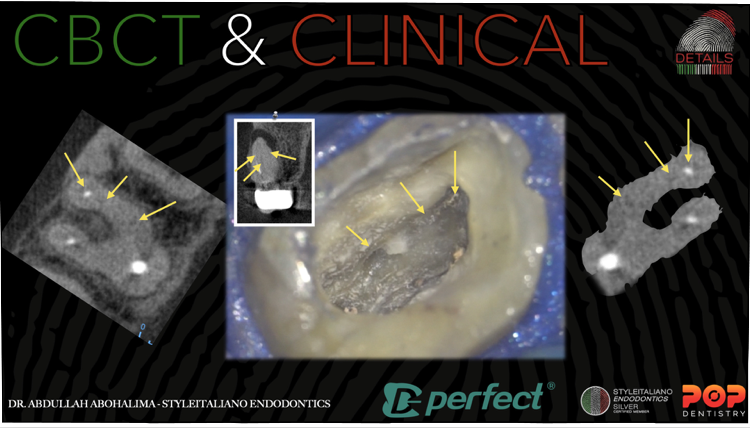
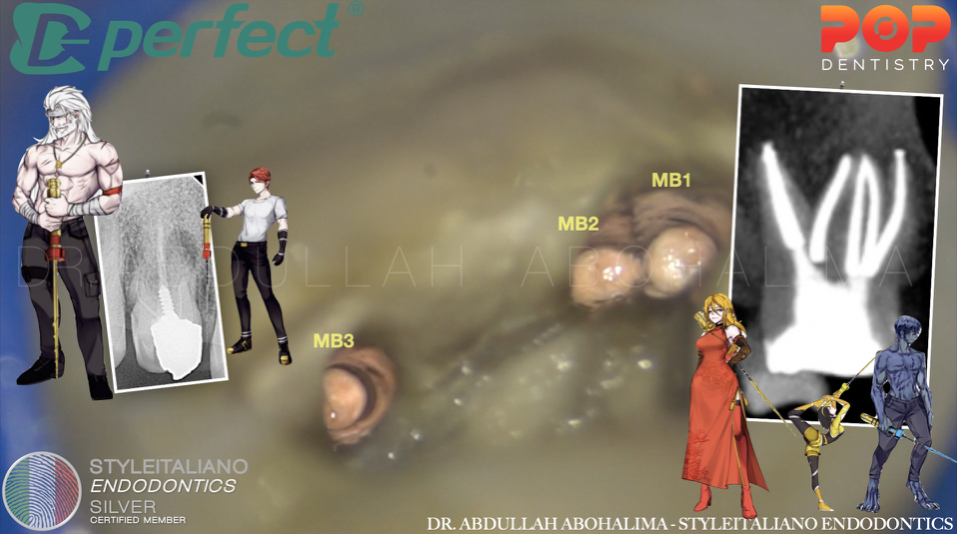
Fig. 1
Confirming CBCT finding with the clinical situation: in the mesio-buccal root there are two missed canals, MB2 and MB

Fig. 2
time to use ReTreaty kit for conservative retreatment, designed by Style Italiano Endodontics and manufactured by Perfect Endo
-Moving into the gutta percha removal phase starting with the first file BULLY which has a size of 25 and 7% taper specifically used for removing coronal gutta percha. The gold treatment of the alloy, the tip design, and the shorter length of the file provide to the instrument the right features for removing in a short time the Gutta-Percha without any solvent.
While removing the gutta percha from the palatal canal, I noticed a very wide canal with an open apex which alerted me to choose a suitable obturation technique later on
Then comes the role of SHAPY 1,2 and 3 in shaping the canals as conservative as possible

Fig. 3
The sequence used
Before and after ReTreaty

Fig. 4
Master cone fit and modification for MTA APICAL PLUG
Moving into the obturation phase.
As previously mentioned, the palatal canal had a violated apex (larger than 50 ISO): for this reason I went for an MTA apical plug. First I inserted into the lesion a collagen matrix to act as a barrier and then plugging the MTA to have a perfect hermetic seal.
3D obturation showing a beautiful anatomy.
MB1, MB2, MB3, DB and P canals.
3D obturation for the unusual anatomy
The 3D X-ray tells everything
MB1, MB2, MB3, DB, P
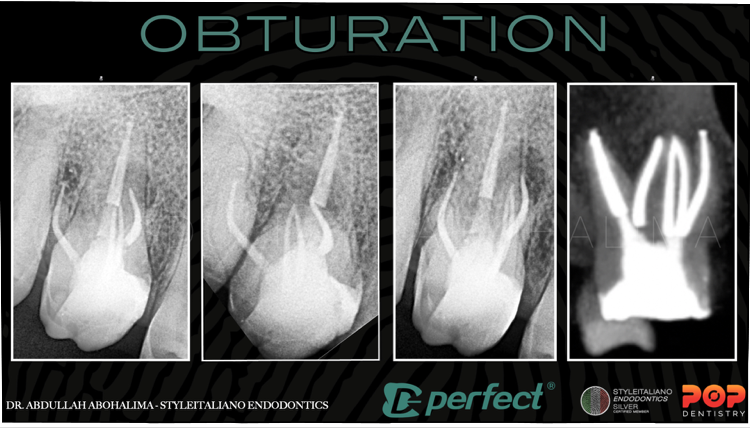
Fig. 5
Different angles MB1, MB2, MB3, DB, P
Conclusions
Non surgical retreatments do not start with gutta percha removal: they start with the strategy created in the clinician's mind, diagnosing and analysing the situation before any intervention being made. Operator skills and experience, together with the right tools (i.e. files tailored for such cases) and appropriare magnification will aid as well in complex cases
Bibliography
1- Schilder H. Filling root canals in three dimensions. Dent Clin North Am. 1967; : 723-74Reit C. Grondahl H.G. Management of periapical lesions in endodontically treated teeth:ùstudy on clinical decision making. Swed Dent J. 1984; 8: 1-7
2-Endodontic Facts, American Association of Endodontists. Available at: http://www. aae.org/about-aae/news-room/endodontic-facts.aspx. Accessed June 1, 2015.
3-Bergenholtz G. Assessment of treatment failure in endodontic therapy. Journal of oral rehabilitation.
4-Gorni FG, Gagliani MM. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod 2004;30:1–4.