Retreatment case with two types of perforations
29/06/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Root perforations were the second greatest cause of failure accounting for 9.62% of all unsuccessful cases. Seltzer et al. also attributed 3.52% of all endodontic failures to perforation. This perforation if left untreated leads to act as a pathway for microorganisms either from periodontal tissues or perforation site, results in secondary periodontal infection, suppuration, fistula formation, and prognosis of that infected teeth become questionable and which leads to extraction of teeth. The presence of root canal variation increases the difficulty of this treatment. It has been reported that 42% of retreatment cases are due to missing canals. Therefore, there is great clinical significance for dentists to master the morphological characteristics of root canals. Branch root canals are common morphological variations in root canal systems, whose morphology can present either as one or more small lateral branches from the main root canal or as two equally large bifurcated root tips on the apical segment.
The anatomical variations in the root canal system of the mandibular premolar are known. Mandibular second premolars typically have one root canal with a reported prevalence of 98.8%. However, it is quite common for the mandibular premolars II to have two canals; with an occurrence range of 1.2% to 29%. and missed anatomy
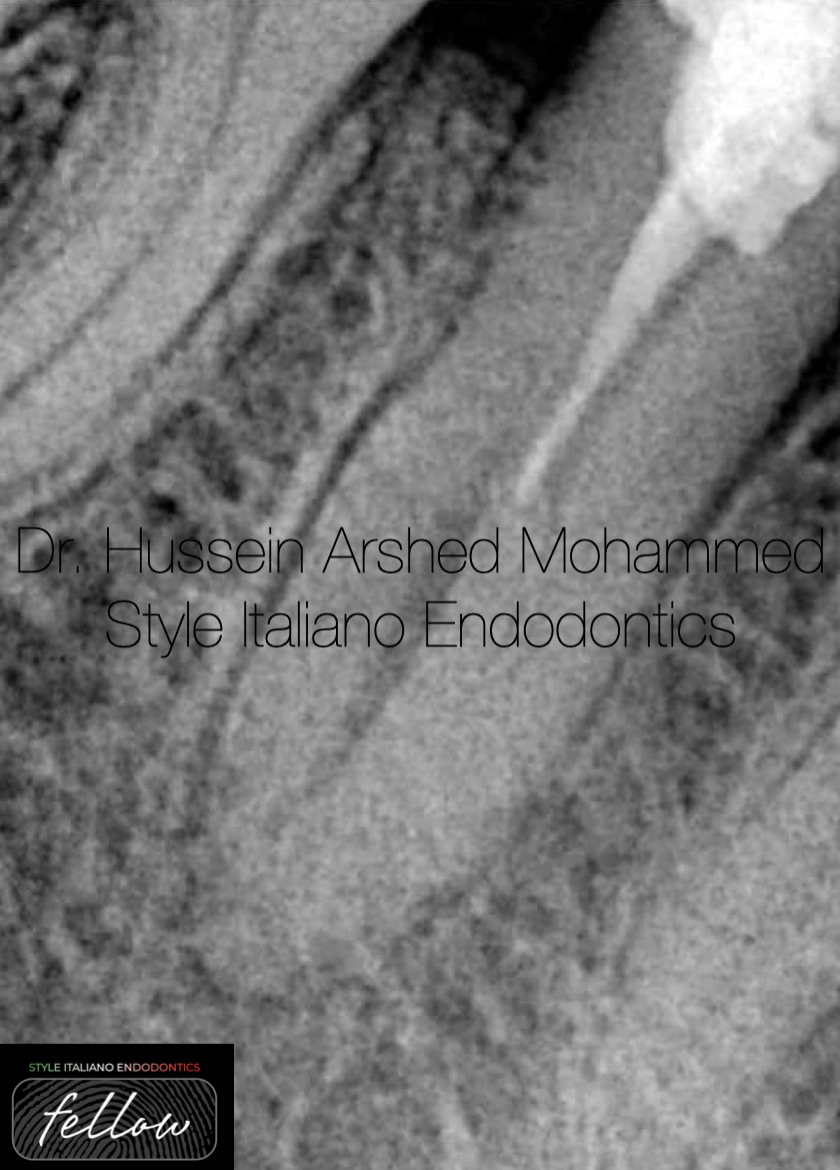
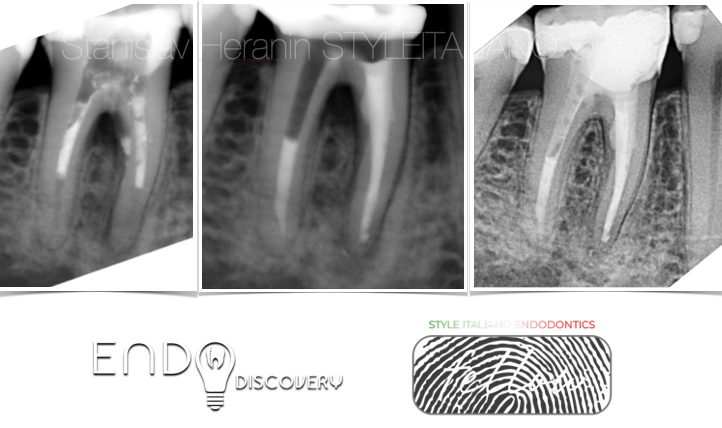
Fig. 1
Pre-op X-Ray sent from colleague dentist showed lower second premolar with fast-break phenomenon (sudden disappearance of pulp space), in this type of configuration there is expectation of extra anatomy, with very short gutta-percha extend only to the middle third of the root.

Fig. 2
Pre operative clinical photo shows that there is cervical supra bony perforation happened when the dentist try to negotiate the canals.
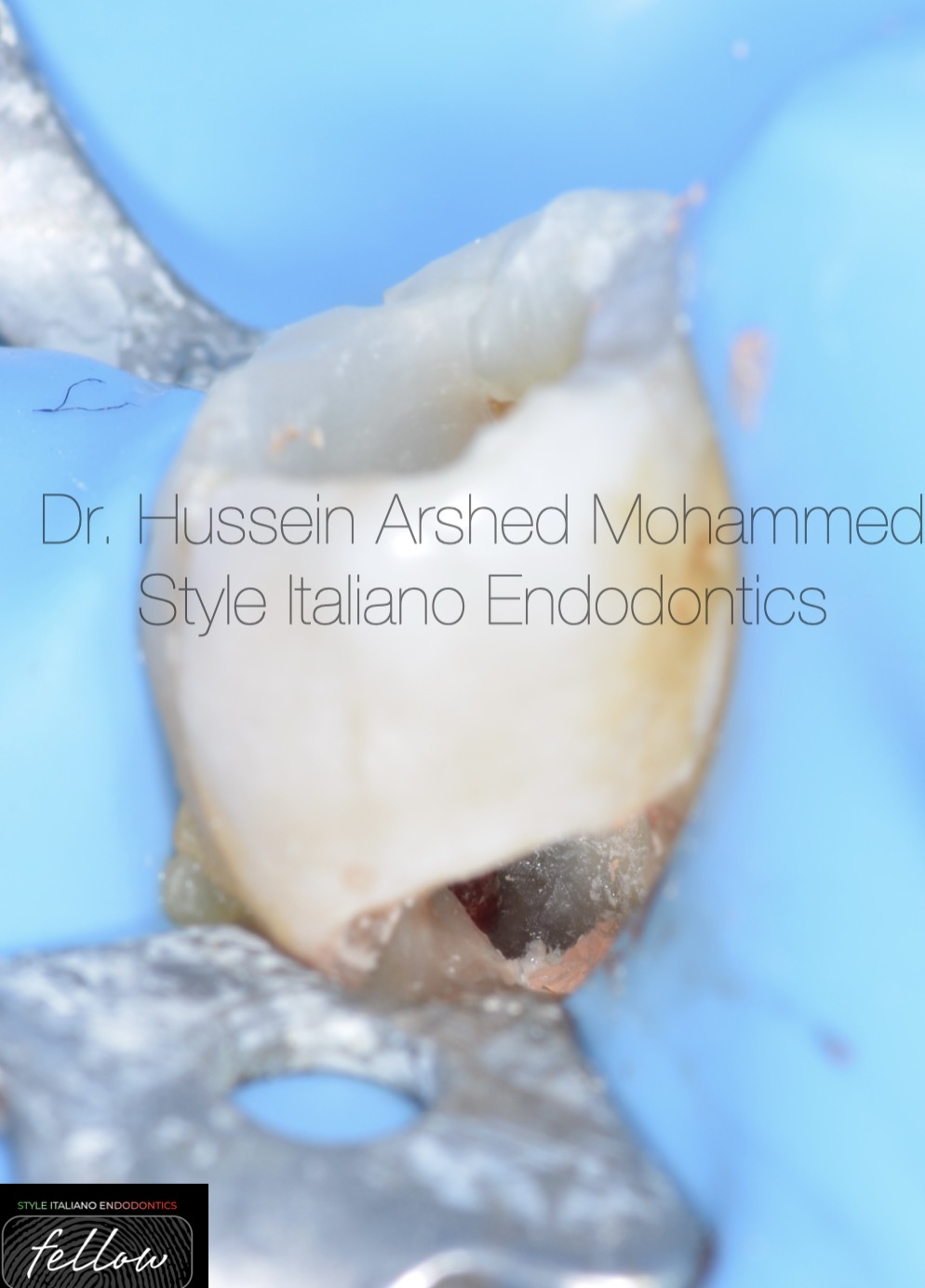
Fig. 3
Rubber dam isolation.
Temporary filling removal.
Refinement of the cervical perforation with caries removal.

Fig. 4
Negotiation of the canals.
There is one lingual and one buccal orifices.
The lingual canal was very tinny.
There is another infra bony perforation.

Fig. 5
Two canals join at the apical third Vertucci type II.
The canal was patent.
Working length was determined by iRoot Apex locator from Bomedent and confirmed by x-ray for all the canals.
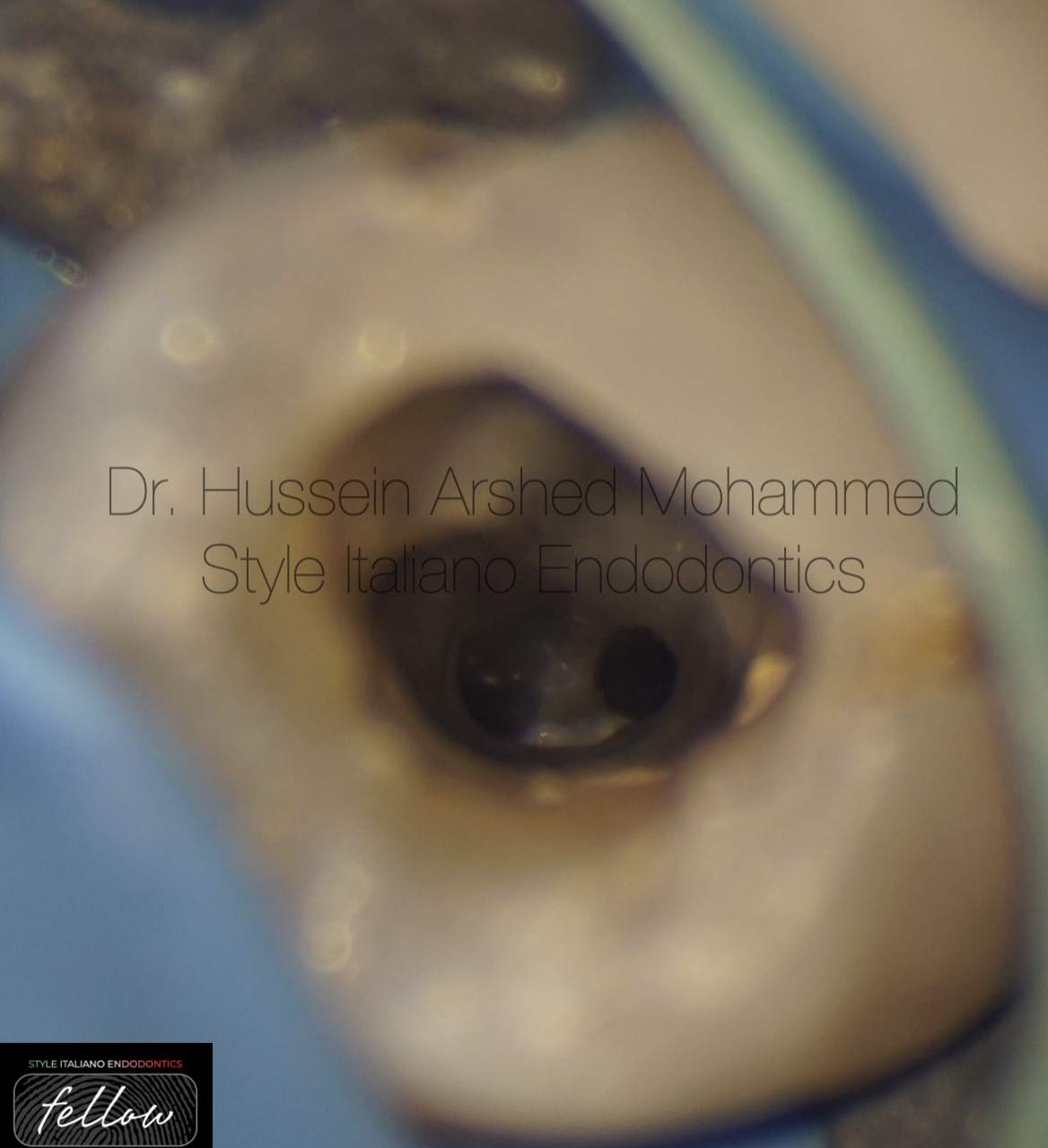
Fig. 6
Microscopic view of the pulp chamber showing the buccal and lingual orfices of the canals after flaring.

Fig. 7
Shaping till the full working length 30/04 for all the canals and master apical cone confirmed.
The shaping protocol :-
- coronal flaring with orifice opener file
- D finder file # 10.
- Rotary file 15/03
- Rotary file 17/04
- Rotary file 25//04
- Rotary file 30/04
With copious amount of NaOCl 5.25% between each file, EDTA 1cc for all the canals with sonic activation for 1 minutes to remove the smear layer and followed again with NaOCl to disinfect again.
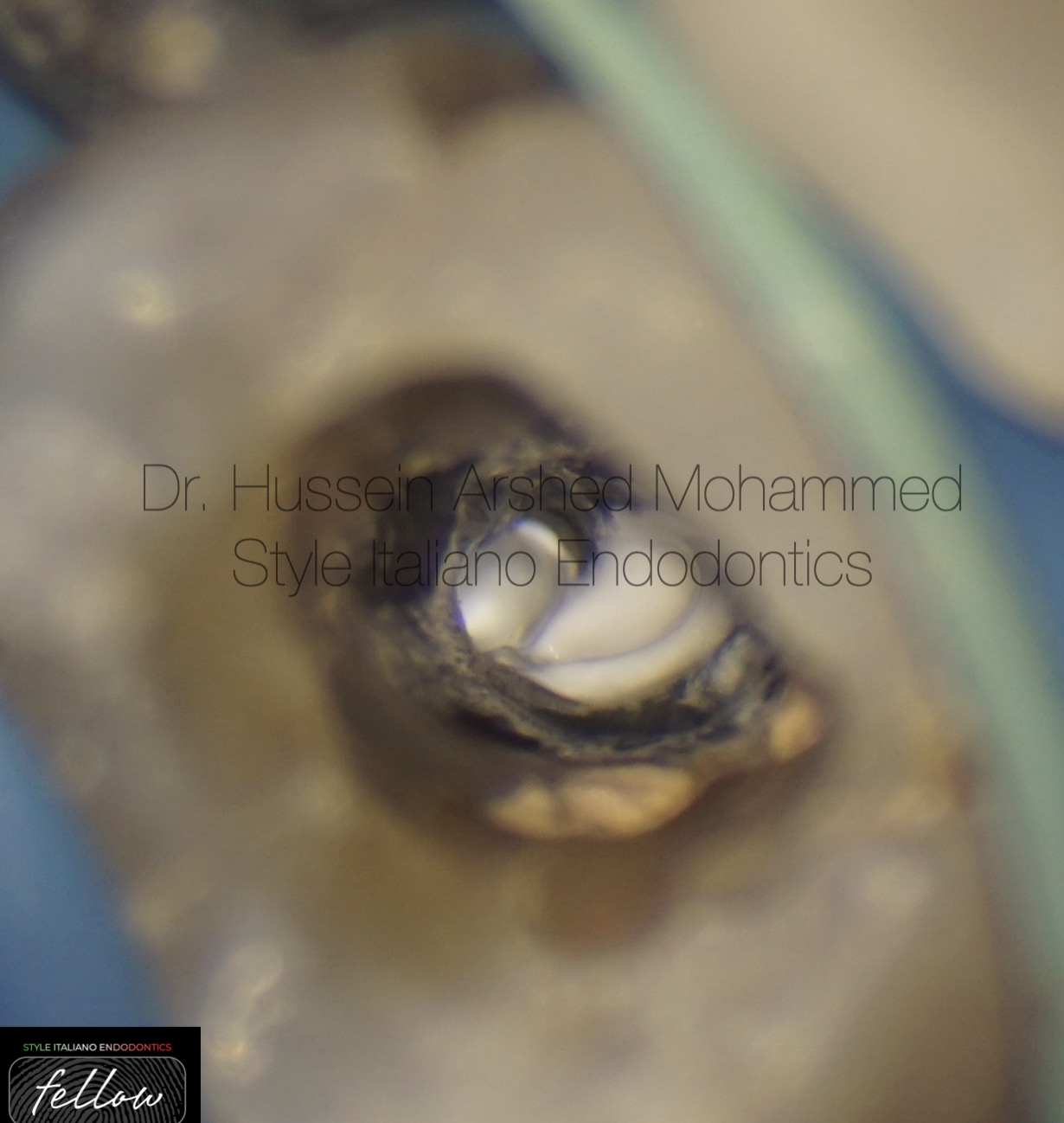
Fig. 8
Injection of neosealer bioceramic sealer from Avalon Biomed for both of the canals.
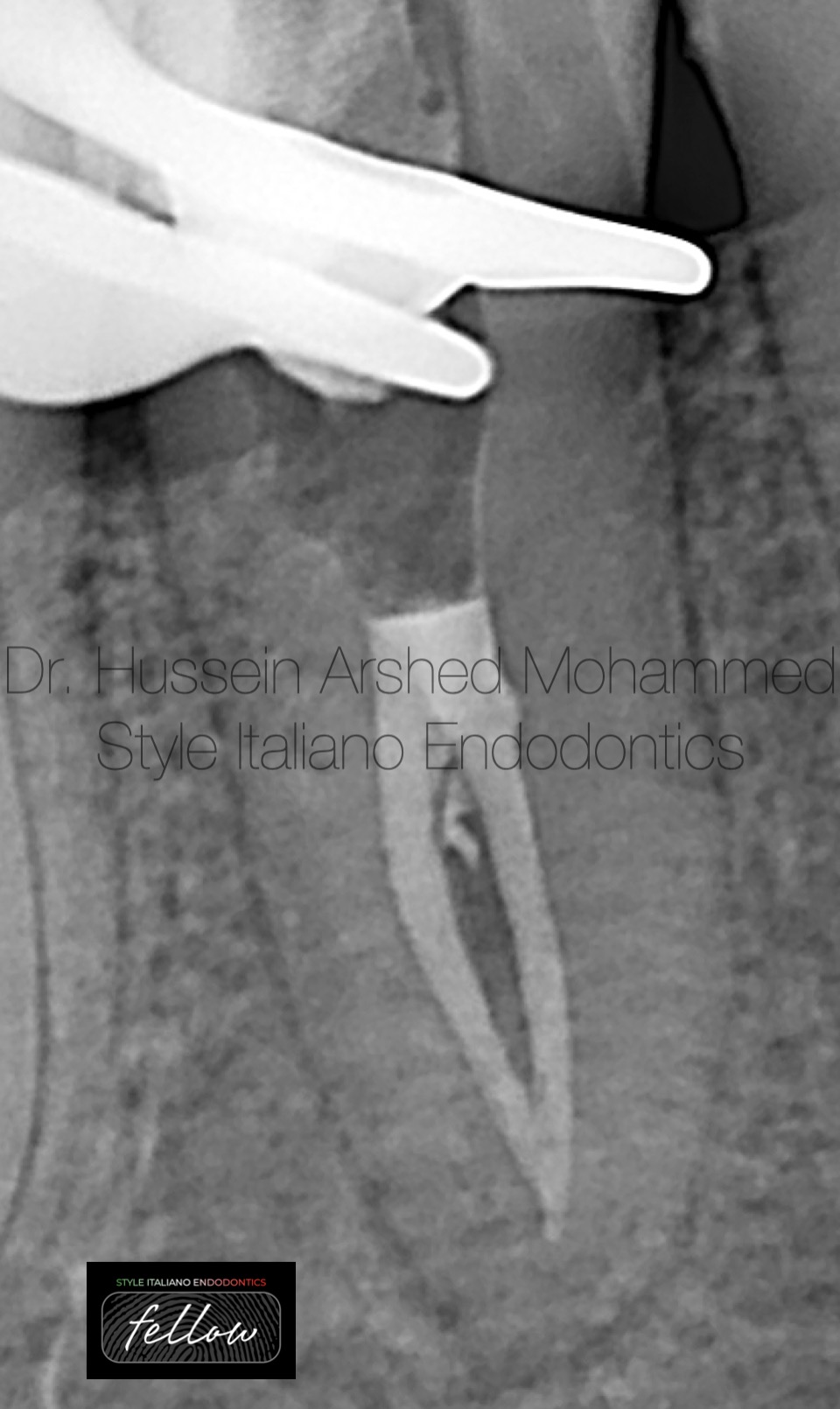
Fig. 9
Obturation of the canals by single cone with neosealer bioceramic sealer from Avalon Biomed. After cutting the guetta-percha with obturation pen with the confirmation of the final x rays, short obturation was noticed.

Fig. 10
Removal of the obturation material to re-establish the full working length again.

Fig. 11
Removal of the obturation material to re-establish the full working length again.
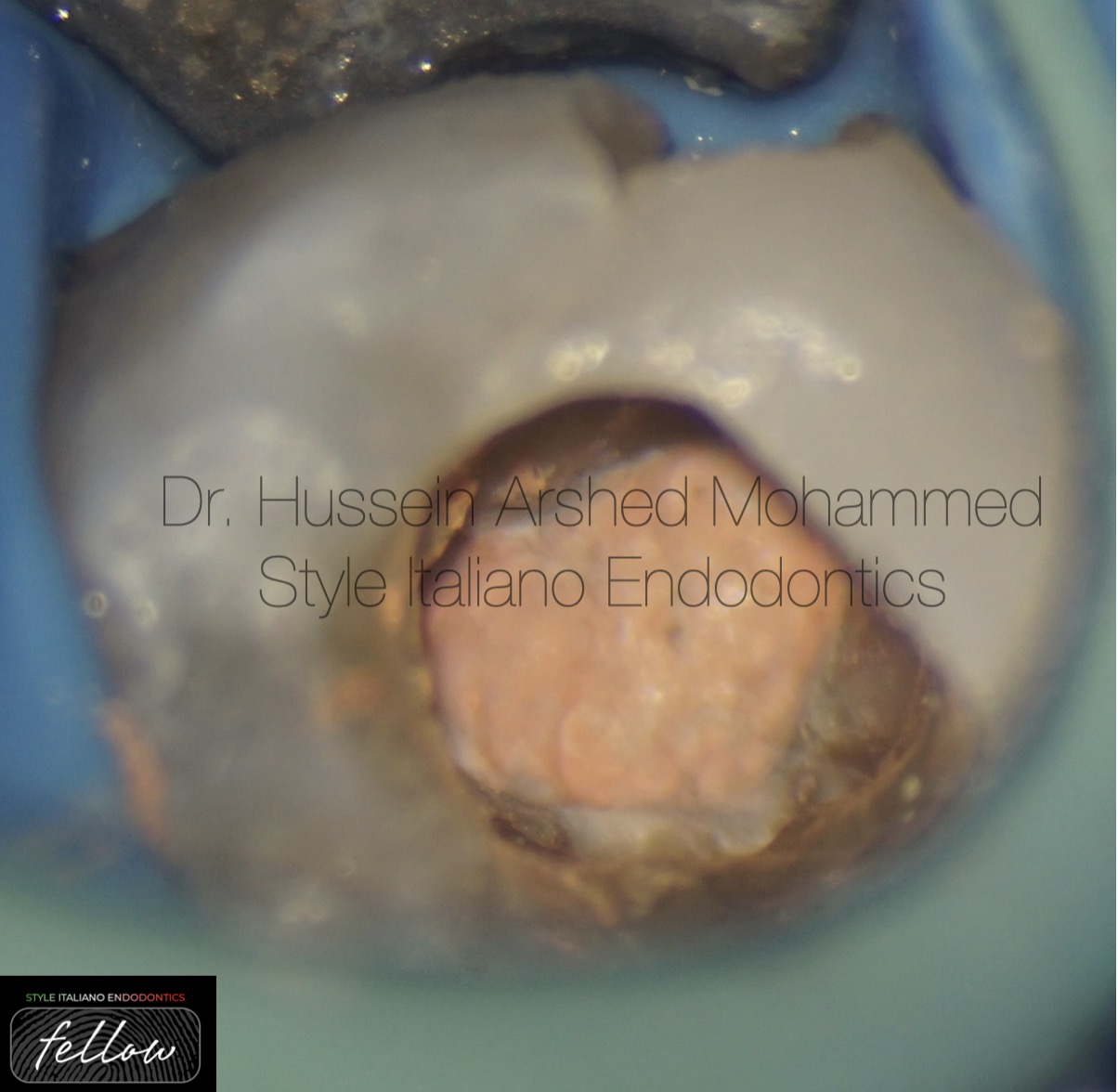
Fig. 12
Sealing of the orfices by injecting heat softened guetta-percha

Fig. 13
Cleaning and disinfecting of the infra bony perforation by removing the granulation tissue then application of cotton pell moistened with full concentration of NaOCl.

Fig. 14
Post-operative X-ray, sealing of the infra bony perforation with Neo MTR from Avalon Biomed and the super bony perforation with composite filling material with final restoration.

Fig. 15
About the author:
Dr. Hussein Arshed graduated in 2012 from Mustansyria university in Iraq.
- in 2018, he got high diploma in Endodontics from Mustansyria university
- In 2023, he got master degree in Endodontics from Mustansyria university
- He works in Rivan dental clinic in Baghdad
- He has been offering lectures, training courses, webinars for dentists.
- He is international lecturer and gives many lectures locally and internationally.
- He is a fellow member of Style Italiano Endodontics.
- He is key opinion leader for Avalon Biomed company in Iraq.
Conclusions
This case report presents the successful endodontic treatment of a mandibular second premolar with double Canals. Before starting root canal treatment it is essential to always consider variations in pulp anatomy and morphology. using magnification tools, to magnify the internal anatomy of a root canal increases the probability of finding additional canals. The perforation management should be decided according to many factors. Thus, the clinician should have a thorough knowledge of the anatomy of tooth to prevent the chances of perforation. With the advent of newer materials and techniques for sealing, the clinical management and prognosis have been improved.
Bibliography
- Patel S, Dawood A, Ford TP, et al. The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J. 2007;40(10):818–30
2. Zhang R, Wang H, Tian YY, et al. Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular molars in Chinese individuals. Int Endod J. 2011;44(11):990–9.
3. Siqueira JF Jr. Aetiology of root canal treatment failure: why well-treated teeth can fail. Int Endod J. 2001;34(1):1–10.
Cohen S, Hargreaves KM. Pathways of the Pulp. 9th ed: St Louis: Elsevier Mosby; 2006. p. 216-7
4. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589–99
Yoshioka T, Villegas JC, Kobayashi C, et al. Radiographic evaluation of root canal multiplicity in mandibular first premolars. J Endod. 2004;30(2):73–4
5. Yang L, Han J, Wang Q, Wang Z, Yu X, Du Y. Variations of root and canal morphology of mandibular second molars in Chinese individuals: a cone-beam computed tomography study. BMC oral health. 2022;22(1):1–12.
6. Senthilkumar, V. and Subbarao, C., 2017. Management of root perforation: A review. Journal of Advanced Pharmacy Education & Research| Apr-Jun, 7(2).