Retreatment and post-retained restoration in a central incisor
09/02/2026
Francesca Cerutti
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
When a tooth has undergone root canal treatment and has lost a large amount of coronal structure, the restorative challenge is not only to replace missing tissue, but to recover function in a biomechanically predictable way. In this context, the use of a fiber-reinforced endodontic post can be particularly advantageous, as it helps to retain the core restoration and to distribute functional stresses along the root in a manner more similar to natural dentin, reducing the risk of catastrophic root fractures often associated with rigid metallic posts. The elastic modulus of fiber posts, closer to that of dentin, favours a more homogeneous stress pattern within the residual tooth, supporting long-term survival when associated with adhesive luting procedures and cuspal coverage in severely compromised teeth. This article will describe a case of retreatment where there was the indication for fiber post placement.

Fig. 1
Pre operative situation:
The patient presented with two defective crowns, with secondary decay, that had been that way for several years.
Considering the extension of the decay, the time of the exposure of the root canal filling to the oral environment and the quality of the existing root canal treatments, the following treatment planning was formulated:
1) Removal of the existing crowns and positioning of a provisional crown on 1.1 and 2.1
2) Retreatment of 1,1. restoration with post, adjustment of the provisional crown
3) Retreatment of 2.1, restoration with post, adjustment of the provisional crown
4) Impression for definitive crowns
5) Luting
Video of the procedure:
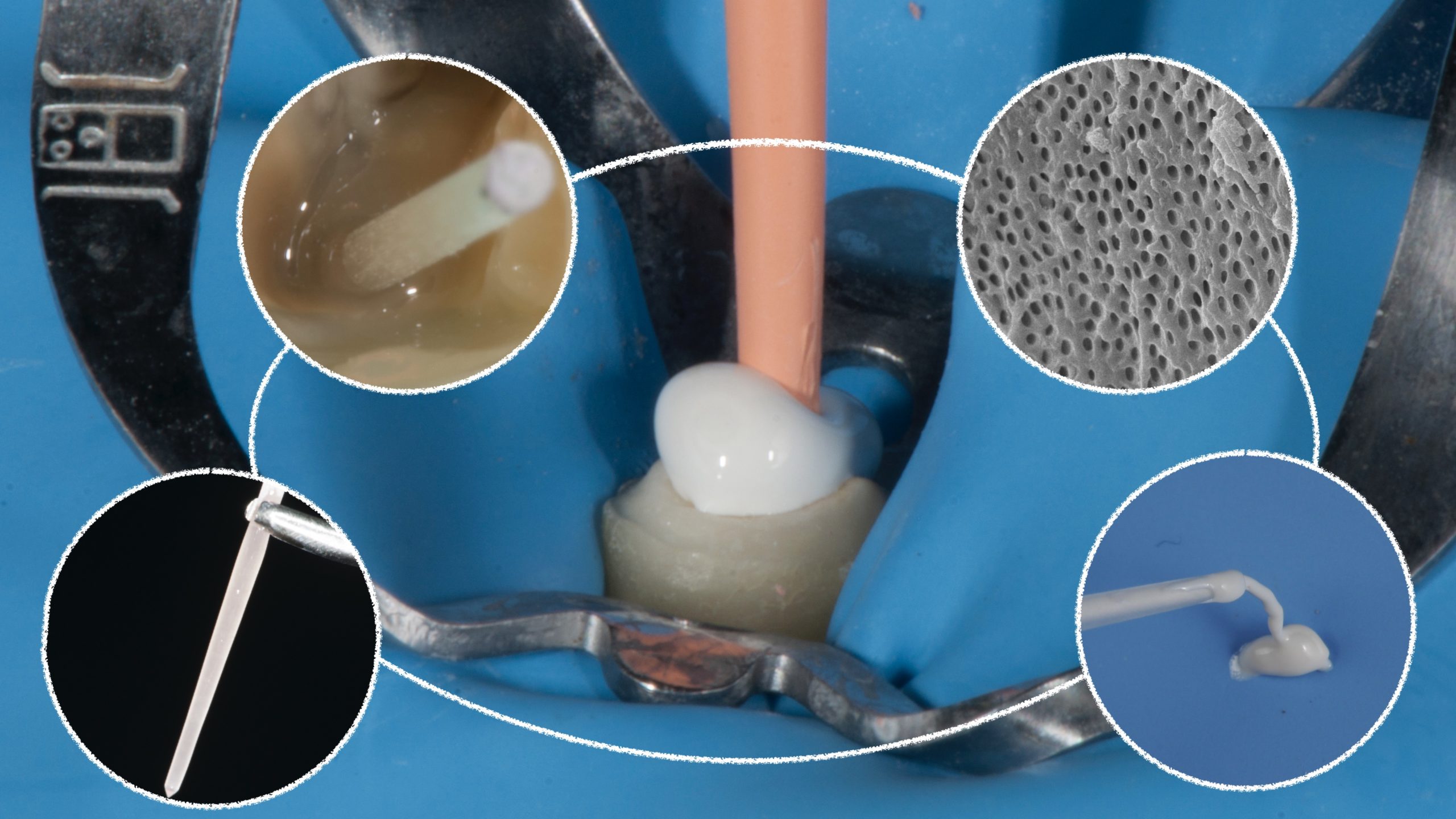
After removing the existing filling material, I shaped cleaned and filled the root canal system.
After that, I used a dedicated bur to refine the post space. In a minimally invasive mindset, we do not adapt the root to the post but, vice versa, we choose the post that best adapts to the root. The use of the bur is intended to remove the remnants of gutta percha or sealer that can jeopardize the adhesion of the luting composite to the radicular dentine.
I chose the largest post (HiRem Post, Overfibers) that passively fit into the post space: this leaves small room for the luting composite (preventing problems of excessive shrinkage of the material during the process of conversion to polymer) and avoids transmitting stresses to the root.
The best practice in case of luting post suggests to cut the post to the desired length before luting it, in order to avoid the exposure of the post to the oral environment (situation that happens when the post is too long and it is not covered by composite) and to avoid contamination of the operative field when the post is cut after being cemented.
I used a self adhesive-dual curing composite (OverCem, Overfibers) in order to reduce operative times and to achieve optimal results in this phase.
After that, I restored the tooth with composite and adapted the provisional crown.
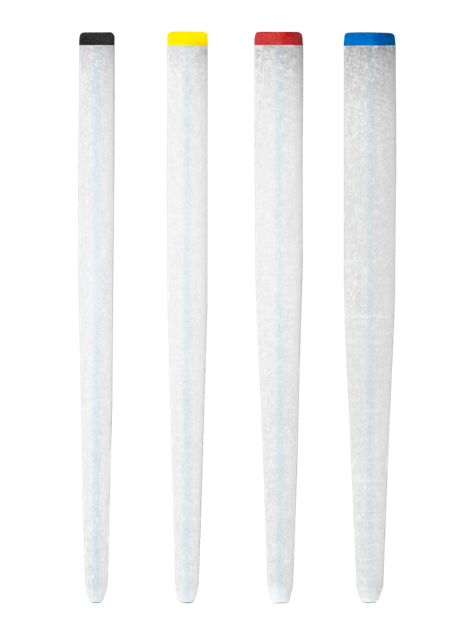
Fig. 2
HiRem Post
Hi-Rem Post is a glass fiber reinforced composite post designed to offer high mechanical performance and predictable retreatability. Its reinforced composite structure provides elevated flexural strength (around 1500 MPa) and a high, well-balanced elastic modulus (about 60 GPa), ensuring excellent resistance under masticatory load and suitability even for crownless teeth. The post is clearly radiopaque, with a radiopacity comparable to more than 2 mm of aluminum, allowing easy identification and radiographic control during and after cementation. The surface shows a very high intrinsic roughness, significantly greater than many competing posts, which enhances micromechanical retention and allows strong and reliable bonding to adhesive resin cements without additional surface pretreatments
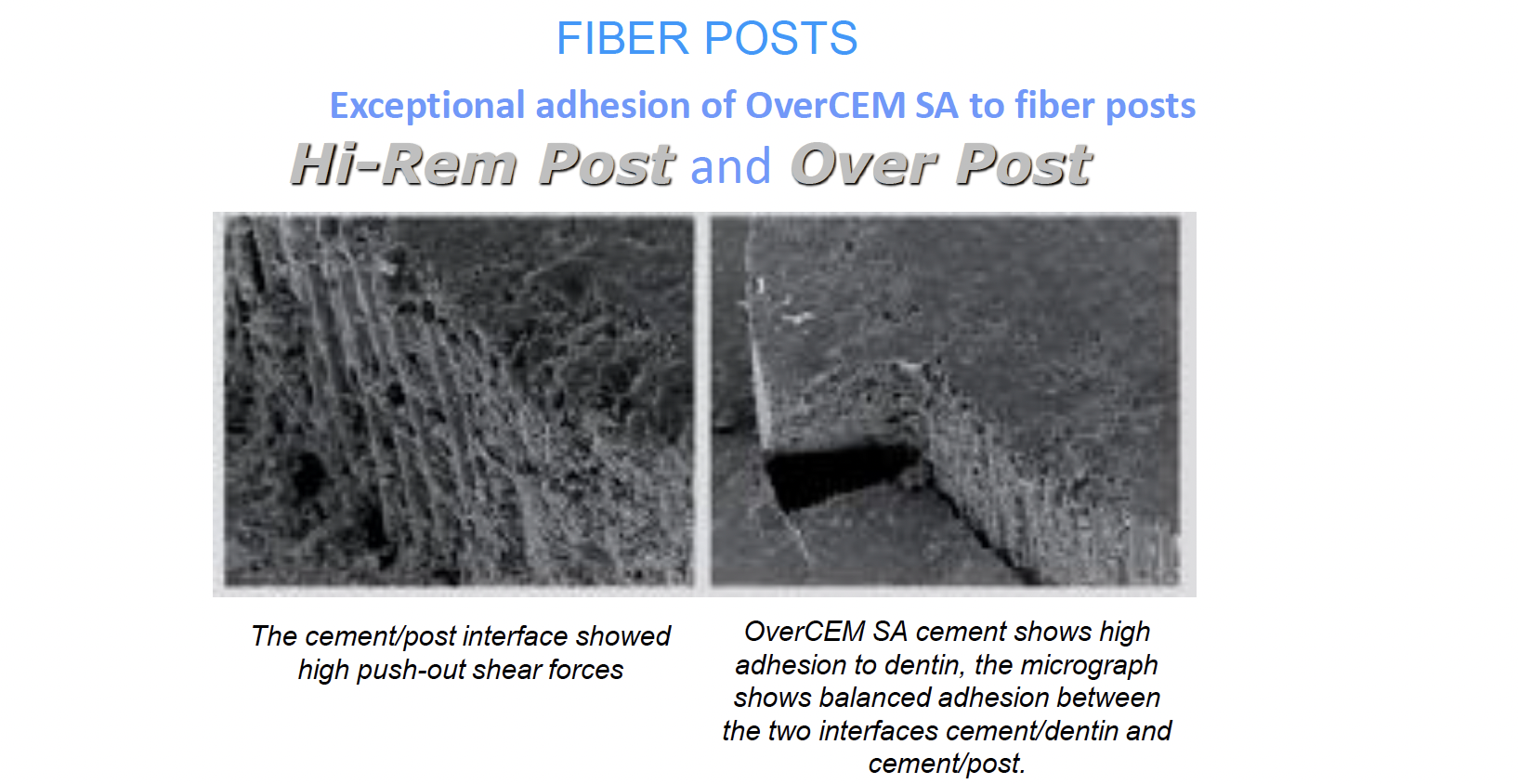
Fig. 3
OverCEM SA
OverCEM SA is a dual-curing self-adhesive resin cement of the latest generation, formulated to simplify luting procedures while maintaining high adhesive performance. Thanks to the combination of 10-MDP and 4-META adhesive monomers, it reaches exceptional adhesion levels to dental tissues, zirconia, metals and other restorative materials, positioning it among the best self-adhesive cements in terms of adhesion and flexural strength. The cement incorporates its adhesion promoters, so separate etching, primer and adhesive are not required, reducing operative steps and sensitivity to technique. Its formulation with a low content of hydrophilic monomers increases long-term stability, chromatic stability and biocompatibility, and the small T-Mixer tips reduce cement waste by about 30% compared with conventional mixing tips, ensuring efficient and controlled application
Conclusions
The combination of OverCem and HiRem Post offers to the clinician a powerful tool to restore quickly and effectively endodontically treated teeth.
Bibliography
1. Ambica K, Mahendran K, Talwar S, Verma M, Padmini G, Periasamy R. Comparative evaluation of fracture resistance under static and fatigue loading of endodontically treated teeth restored with carbon fiber posts, glass fiber posts, and an experimental dentin post system: an in vitro study. J Endod. 2013;39(1):96-100.
2. Cerutti F, Acquaviva PA, Gagliani M, Ferrari M, Mangani F, Depero LE, et al. Degree of conversion of dual-cure resins light-cured through glass-fiber posts. American journal of dentistry. 2011;24:8-12.
3. Figueiredo FE, Martins-Filho PR, Faria ESAL. Do metal post-retained restorations result in more root fractures than fiber post-retained restorations? A systematic review and meta-analysis. J Endod. 2015;41(3):309-16.
4. Sorrentino R, Di Mauro MI, Ferrari M, Leone R, Zarone F. Complications of endodontically treated teeth restored with fiber posts and single crowns or fixed dental prostheses-a systematic review. Clin Oral Investig. 2016;20(7):1449-57.
5. Jurema ALB, Filgueiras AT, Santos KA, Bresciani E, Caneppele TMF. Effect of intraradicular fiber post on the fracture resistance of endodontically treated and restored anterior teeth: A systematic review and meta-analysis. J Prosthet Dent. 2022 Jul;128(1):13-24. doi: 10.1016/j.prosdent.2020.12.013. Epub 2021 Feb 3. PMID: 33546858.
6. Tsintsadze N, Margvelashvili-Malament M, Natto ZS, Ferrari M. Comparing survival rates of endodontically treated teeth restored either with glass-fiber-reinforced or metal posts: A systematic review and meta-analyses. J Prosthet Dent. 2024 Apr;131(4):567-578. doi: 10.1016/j.prosdent.2022.01.003. Epub 2022 Apr 13. PMID: 35430048.
7. Van Landuyt KL, Wouters E, Zicari F, Debels E, Naert I, Van Meerbeek B, Peumans M. Randomized controlled trial comparing glass-fiber versus metal posts in single-crowned teeth: 15 Year follow-up. J Dent. 2025 May;156:105694. doi: 10.1016/j.jdent.2025.105694. Epub 2025 Mar 15. PMID: 40096878.
8. Nadler AM, da Silva EJ, Lins-Filho PC, Dias MF, Guimarães RP, da Silva CH, Silva SS, Gomes AS. Influence of different adhesion strategies on glass fiber post retention. J Clin Exp Dent. 2023 Aug 1;15(8):e649-e657. doi: 10.4317/jced.60452. PMID: 37674597; PMCID: PMC10478191.