Retreament Lower First Molar With Acute Abcess
01/06/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Root canal treatment removes infected pulp tissue to eliminate harmful bacteria and prevent future infection inside the root canals. Proper shaping and cleaning of the canals are essential before they are sealed with a three-dimensional filling. Demand for root canal treatment has increased in recent years because preserving natural teeth is now preferred over extraction.(1)
Even when an adequate standard of treatment is performed, failures may occur, owing to the anatomical characteristics of the root canal system and to the presence of peculiar noxious factors within the inflamed tissue (2). The persistence of micro-organisms in the root canal system may induce an inflammatory and immune response in the periradicular (periapical) tissues, resulting in local bone destruction. Furthermore, contamination of the periradicular tissues and of the filling material by micro-organisms may initiate a foreign body reaction, thereby impairing tissue healing. Large cross-sectional studies have reported that the prevalence of apical periodontitis and other posttreatment periradicular disease can exceed 30% of all root-filled teeth , suggesting a considerable need for treatment of this condition.(3,4)

Fig. 1
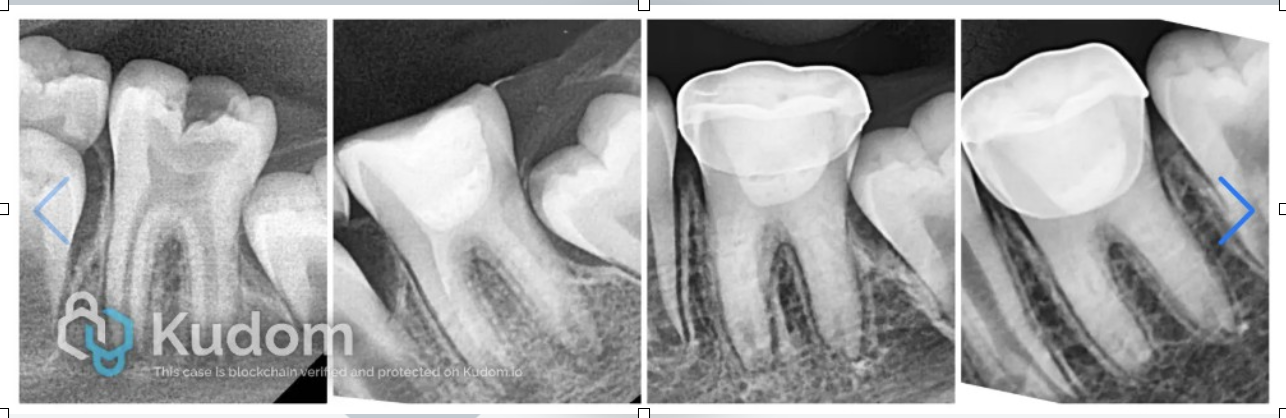
A 45-year-old patient presented with swelling & severe pain associated with the mandibular right first regain. Clinical examination revealed broken old composite restoration for lower right first molar and severe pain with percussion .
Periodontal Examination : Slight Mobility With Normal Probing Depth
Radiographic Examination revealed previous poor rct from 2 years & large periapical lesion
Diagnosis : Failed Endodontic Treatement With Secondary Symptomatic Apical Periodontits ( Acute Phenix Abcess ) .
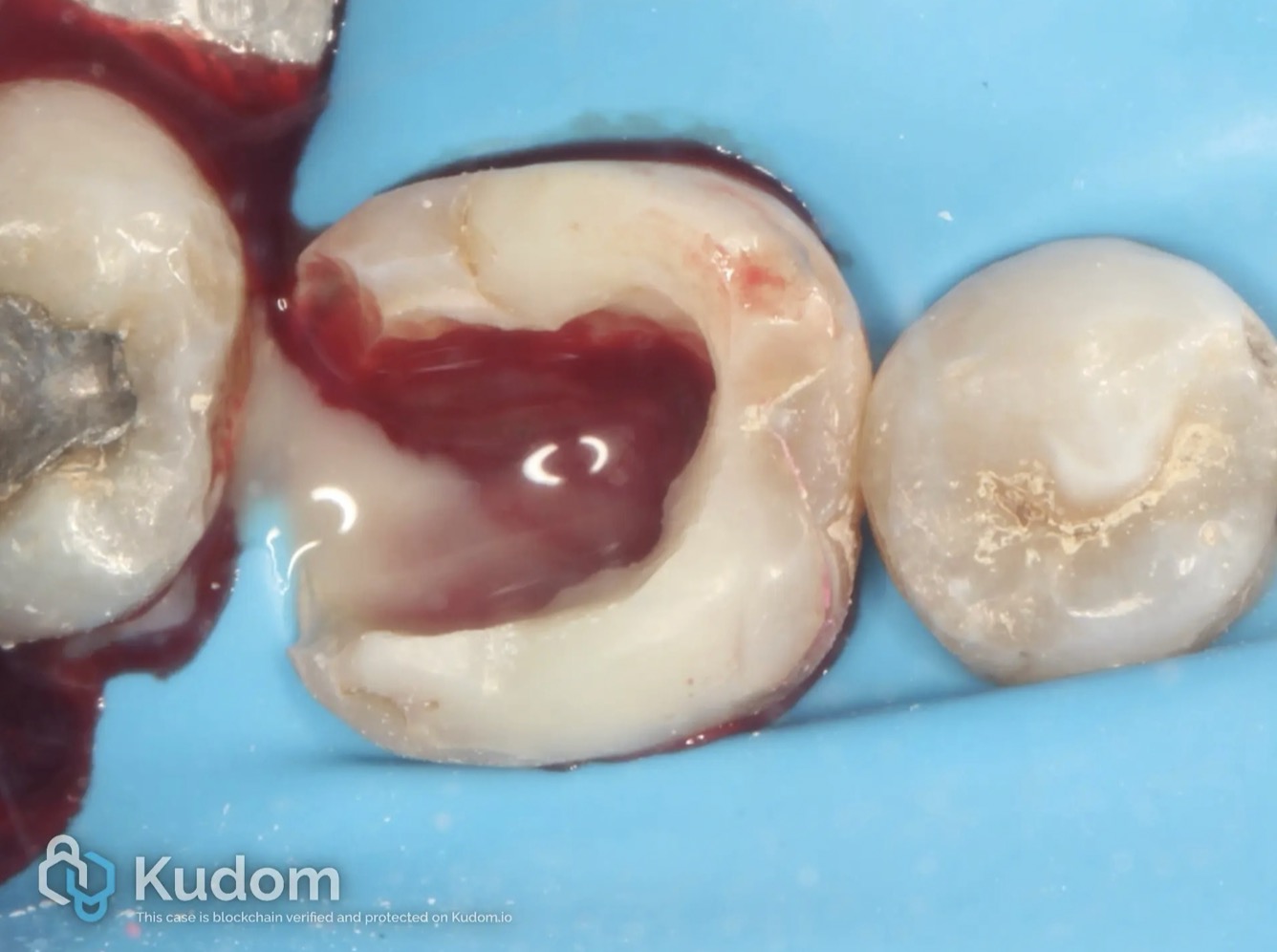
Fig. 2
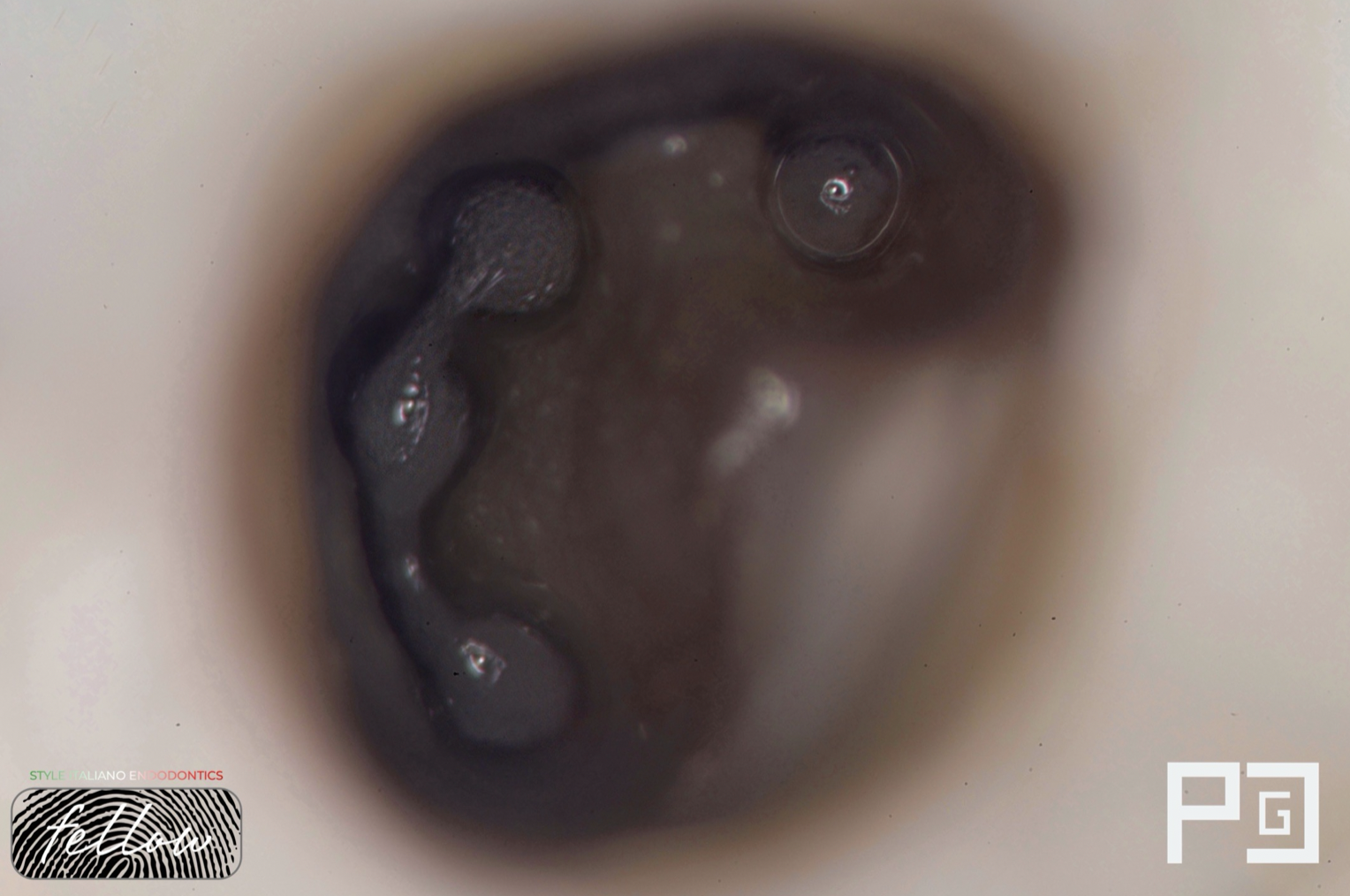
Complete isolation of the tooth was achieved using a rubber dam to maintain a sterile and dry operating field, minimizing the risk of microbial contamination during endodontic retreatment. The existing composite restoration and carious dentin were carefully removed to gain access to the pulp chamber. Previously placed gutta-percha was then retrieved from all canals using H-files.
Upon removal of the obturation material, the distal canal exhibited profuse purulent drainage, indicating the release of accumulated intracanal pressure secondary to persistent infection. Initial drainage consisted predominantly of pus, which gradually transitioned to a mixture of pus and blood, and finally to blood only. Copious irrigation with warm saline was performed until complete drainage was achieved.
Subsequently, thorough cleaning and shaping were carried out using the Plex-V rotary system up to size 35/.04 in all canals. Intracanal medication with calcium hydroxide was placed, followed by temporary coronal sealing.
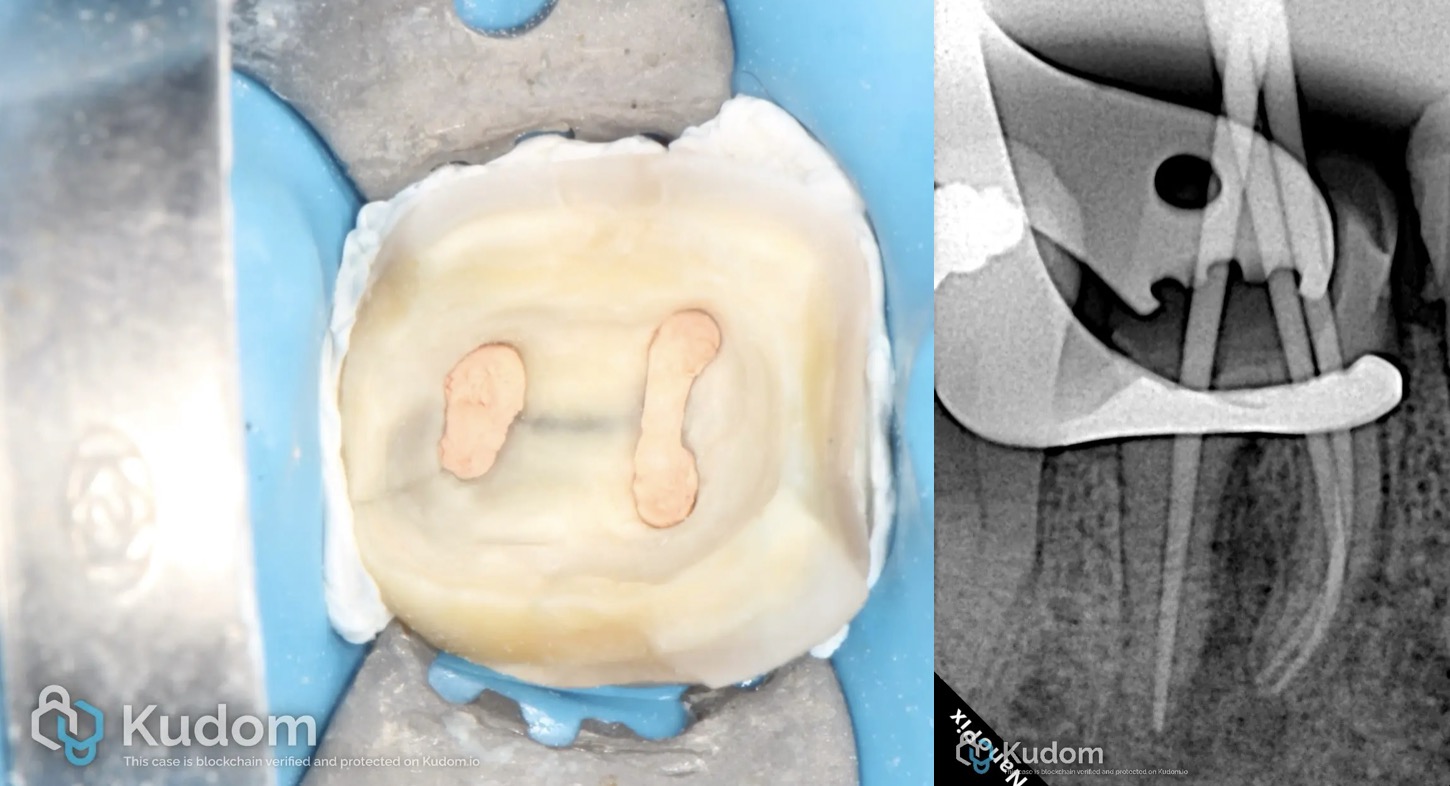
Fig. 3
At the second treatment visit, the patient was asymptomatic, indicating successful resolution of the acute infection following intracanal medication. After removal of the temporary restoration and calcium hydroxide dressing, copious irrigation with sodium hypochlorite was performed to ensure optimal canal disinfection and removal of residual debris.
Master cone radiographic verification was subsequently carried out to confirm appropriate working length and canal adaptation prior to obturation. Final obturation of the root canal system was then completed, achieving a dense and well-adapted three-dimensional seal of all canals.

Fig. 4
The red arrow indicates an area of concern of crack within the remaining tooth structure; however, no displacement or structural separation was observed. Careful clinical evaluation confirmed the integrity of the tooth structure with no evidence of fracture propagation or instability.
To reinforce the weakened tooth structure and enhance its long-term resistance to functional loading, EverX flowable composite was placed as an internal reinforcing core. This approach was used to improve fracture resistance and provide a strong supportive foundation for the final restoration.
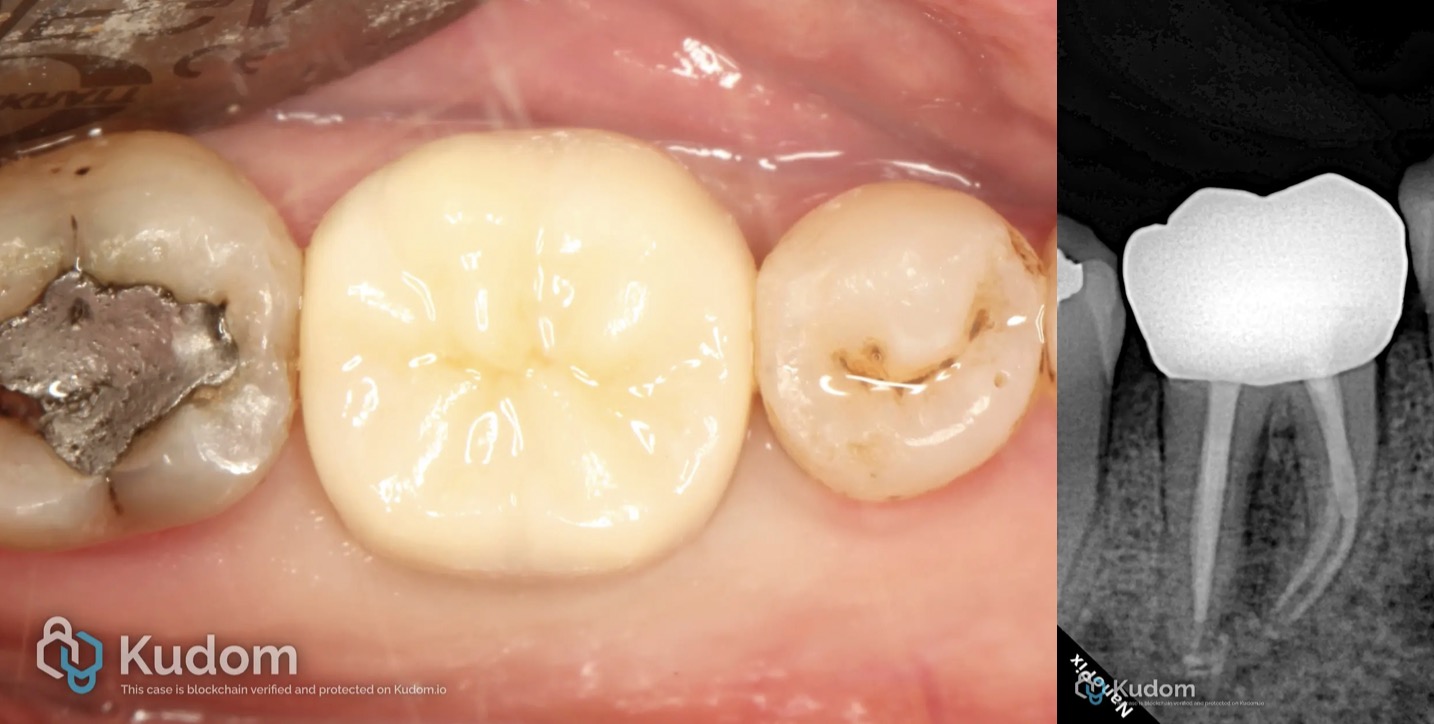
Fig. 5
Definitive monolithic zirconia crown after cementation demonstrating excellent marginal integrity, anatomical form, shade compatibility, and soft tissue response

Fig. 6
Conclusions
This case highlights the importance of nonsurgical endodontic retreatment in the management of failed root canal therapy associated with periapical abscess formation. Proper canal disinfection, reshaping, and obturation contributed to the resolution of symptoms and healing of the periapical tissues. The use of a definitive zirconia crown provided adequate coronal seal and functional rehabilitation. Careful follow-up demonstrated favorable clinical and radiographic outcomes. Successful retreatment can preserve the natural tooth and restore long-term function and esthetics..