Restore the Natural: A complex horizontal fragment reattachment
13/01/2017
Massimo Giovarruscio
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
A common trauma of anterior teeth is a coronal fracture. In according with the other article of Fabio Gorni on the same topic, also In this case we report a new conservative approach of a complex double reattachment associated to root canal therapy followed by fixing the fragments with a post. Due to the young patient age, the only conservative approach can solve succesfully the treatment. Revascularization is becoming very popular in treating teeth with wide canal and open apex but retsoring teeth using the fragments requires a quick, easy and aesthetic procedures.
This case shows a complex situation as the fracture of teeth is on the gum level. It causes a difficult reattachment especiallt because the dentist tried to reattach the fragments. Previously adhesive procedures altered the fragments fitting. Tips and tricks are showed to make this procedure as simple as possible.

Fig. 1
An 11 years old patient comes in emergency after a dramatic accident on both 11 and 21. The fracture involves enamel;dentin and pulp due to the high horizontal fracture on both teeth at the gum level
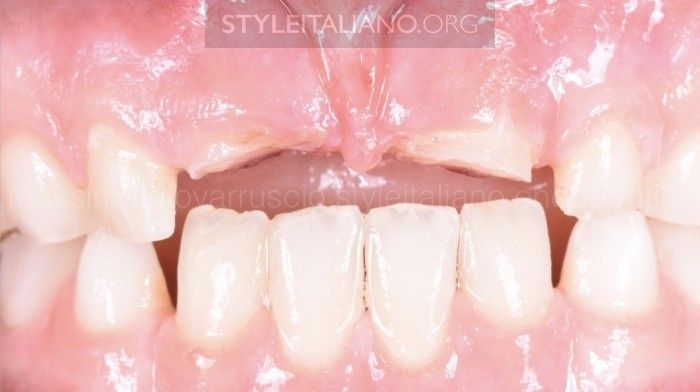
Fig. 2
According to the treatment guidelines described in the litterature, this patient has a complicated crown fracture

Fig. 3
Dramatichorizontal fracture with pulp canal exposure on both teeth

Fig. 4
The PA shows a wide canal on 11 and 21 as an immature teeth and the fracture at gum level

Fig. 5
The patient's father is a dentist and he could keep fragments. The father tried to reattach the fragments using composte with no success due to the deep farcture. With complicated crown fractures, the best option is to reattach this fragment, by using a bonding agent and composite resin and without any preparation of the tooth or the fragment. But in this case a RCT is higly recommended to perform a post restoration.The provided fragments were stored in distilled water during the clinical procedures

Fig. 6
The gingival gum has been cut using electrosurgical tip to obtain a proper fitting of the clamps

Fig. 7
After rubber dam isolation, the RCT on 11 and 21 has been performed using MTA material due to the open apex

Fig. 8
The fragments were put in purified water 0.9% NAOCl and then they were cleaned with 0,2% chlorhexidine. After that the fragments were been cleaned using burs polishing tips and paste to remove completely the previously composite material

Fig. 9
The fragmenst are now clean and ready for the adhesive procedures

Fig. 10
Fortunately the young patient had a gum shield where the fragments were fitting very well

Fig. 11
Using the gum shield, it was easy the reposition of the fragments and it was possible to reattach the fragments

Fig. 12
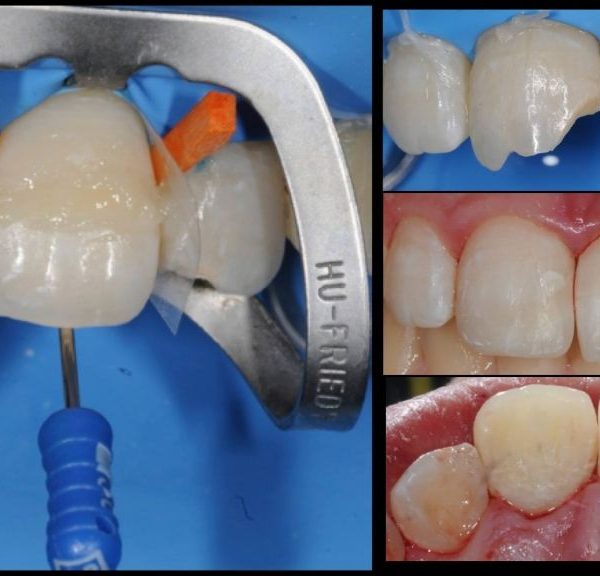
At this point the fragment is prepared using a carbide bur to make enough space to fit a glass fibre post

Fig. 13
A carbide bur has been used to avoid potential fracture of the fragment as the cutting is more efficient then a diamond bur. It is extremely important to evaluate the size of the post by taking into account the depth of the canal and the intra-coronal space. In this case a Medium glass fibre pos (HFO, Micerium) has been selected and then reduced and modified with a diamond burs to be fit passively on the fragment

Fig. 14
TRY-IN PROCEDURE: This step is the more important step of all procedure. The fragment with the post has been tryed to chech the marginal fitting. It is necessary to try the perfect fitting of the pos into the canal and the post into the fragmen without any interference

Fig. 15
The fragmens adaptation is imperfect due to the loss of enamel and dentine but we decided that the best treatment plan was to reattach the fragment

Fig. 16
The fragment was etched with 35% phosphoric acid for 15 seconds and rinsed

Fig. 17
Fragments and fibre posts cemented permanently with dual-curing composite

Fig. 18
The fragments are put on a stick to handle it easily. Both fragments are ready to be treated for adhesion

Fig. 19
The fragment and the bonded fibre post were etched with 35% phosphoric acid for 15 seconds and rinsed

Fig. 20
An etch and rinse procedure has been performed. The first step is to sandblast the surface and after we use an 37% orthophosphoric acid on enamel and dentin;for 15 seconds and rinsed

Fig. 21
Many layers of primer agent are used on the the tooth and the fragments and after are carefully dried. The surface are then brushed with the bonding agent and light cured for 1 minute

Fig. 22
TRY-IN PROCEDURE. Before using the composite material to fit the reattachments, both fragments were been tried again to double check their fitting

Fig. 23
A dual composite resin was placed into the canal over the entire fractured surface, and the fragments were positioned and properly adjusted.After the dual composite completed the self curing, the restoration was light cured; in a soft mode for 20 seconds and then for 1minute for buccal and palatal sides with glycerin gel to avoid the inhibited layer.Finishing and polishing was performed using brush and diamond paste

Fig. 24
Result after rubber dam removal, finishing and polishing procedures. We have to wait for the rehydratation of both fragments

Fig. 25
Post Op X-Ray shows a nice MTA apical plug and good fitting of the posts and the fragments on the teeth
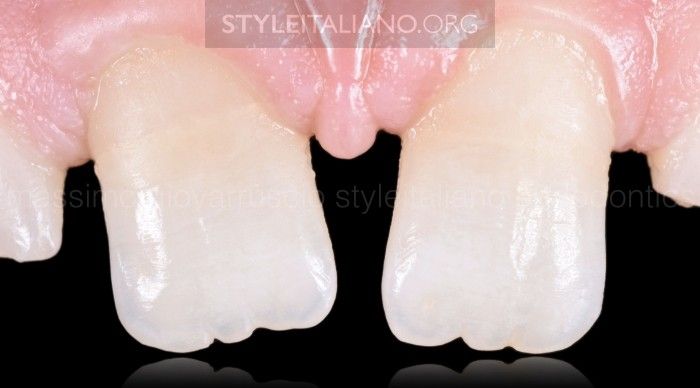
Fig. 26
Review after 4 months. Preparations can also be performed after bonding to improve esthetics by grinding the buccal fracture line and masking it with composite. The final result after 8 months review is showing a good adaptation and great aesthetic result
Conclusions
If the original tooth fragment is retained following fracture, the natural tooth structures can be reattached using adhesive protocols to ensure reliable strength, durability, and aesthetic.
The limitations are only a possible fragment de-bonding or an incomplete fragment rehydration that can result in a color mis-match.
Bibliography
Mangani F., Putignano A., Cerutti R. Guidelines for Adhesive Dentistry: The key to success. --QuintessencePub. 2009). Burkhardt, R., Preiss, A., Joss, A. & Lang, N. P. (2008) Influence of suture tension to the tearing characteristics of the soft tissues: an in vitro experiment. Clinical Oral Implants Research 19, 314?319.
Flores MT., Andreasen JO & Coll. Guidelines for the evaluation and managment of traumatic dental
injuries. Sent Traumat 2001; 17:193-196.
Garcia-Godoy F. A classification for traumatic injuries to primary and permanent teeth. J. Pedodont.
1968; 5. 295-29.
Farik B, Musksgaard EC, Andreasen JO, & Kreiborg S (1999) Drying and rewetting anterior crown fragments prior to bonding Endodontics and Dental Traumatology 15(3) 113-116
Maia EAV, Baratieri LN, Andrada MAC, Monteiro S Jr, & Arau ?jo EM (2003) Tooth fragmente reattachment: Fun- damentals of the technique and two case reports Quin- tessence International 34(2) 99-107.
Simonsen RJ (1982) Restoration of a fractured central incisor using original tooth fragment Journal of the American Dental Association 105(4) 646-648
?lvares I, Sensi LG, Arau ?jo EM Jr, & Arau ?jo E (2007) Silicone index: An alternative approach for tooth frag- ment reattachment Journal of Esthetic and Restorative Dentistry 19(5) 240-246
Terry DA (2003) Adhesive reattachment of a tooth fragment: The biological restoration Practical Periodon- tics and Aesthetic Dentistry 15(5) 403-409.
Rappelli G, Massaccesi C, & Putignano A (2002) Clinical procedures for the immediate reattachment of a tooth fragment Dental Traumatology 18(5) 281-284.
Dietschi D, Jacoby T, Dietschi JM, & Schatz JP (2000) Treatment of traumatic injuries in the front teeth: Restorative aspects in crown fractures Practical Peri- odontics and Aesthetic Dentistry 12(8) 751-758.
Grandini R, Pagni L, Pagavino G, De Fraia E. Using the ?coronal fragment for the repair of anterior
tooth fracture. Quintessence Int Dent Dig 1985;10:839?45 and 925?33.