Regeneration endodontics
08/07/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Dental trauma is a common cause of pulp necrosis in immature permanent teeth, often resulting in interrupted root development characterized by thin dentinal walls, a short root, and a wide-open apex. Regenerative endodontic procedures (REPs) have emerged as a biologically based treatment approach that aims to disinfect the root canal system while promoting continued physiologic root maturation through the recruitment of stem cells, signaling molecules, and a suitable scaffold. Compared with traditional apexification using an apical plug, REPs offers the potential for increased root length, thickening of the dentinal walls, continued apical closure, and improved long-term tooth survival, resulting in a more favorable prognosis. Consequently, REPs represent a valuable treatment option for young patients with necrotic immature permanent teeth.

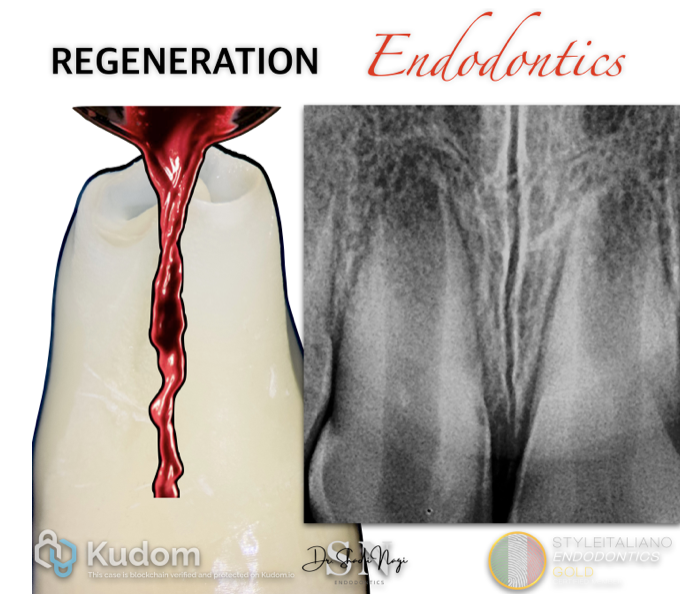
Fig. 1
A healthy 8-year-old patient presented to the clinic with a history of dental trauma following a bicycle accident, which resulted in an incisal fracture of tooth no 1.1. Several months after the injury, the patient developed recurrent swelling that had been managed with repeated courses of antibiotics prior to presentation.
Clinical examination, pulp sensibility testing, and radiographic assessment confirmed pulp necrosis associated with a periapical radiolucency in tooth no 1.1, while the adjacent tooth (1.2) responded positively to pulp sensibility testing. The affected tooth exhibited an immature root characterized by a wide-open apex, thin dentinal walls, and a short root.
Based on these findings, Regenerative Endodontic Treatment (RET) was selected instead of apexification with an apical plug. The primary objective was to promote continued root development by increasing root length and dentinal wall thickness while allowing physiologic apical maturation. A secondary objective was to regenerate functional pulp-like tissue and, if possible, restore tooth sensibility.
The indications of the American Association of Endodontists (AAE) follow:
Case Selection
- Necrotic pulp with an immature open apex, thin dentin walls and short root length.
- No need for a post/core restoration.
- Cooperative patient and parents.
- No contraindications or allergies to required medications.
Informed Consent
- Treatment requires at least two appointments .
- Intra canal antimicrobial medication will be used.
- Discuss possible risks: such as discoloration, persistent infection, pain, or treatment failure.
- Explain alternatives: apexification (MTA) apical plug , observation, or extraction if the tooth is non-restorable.
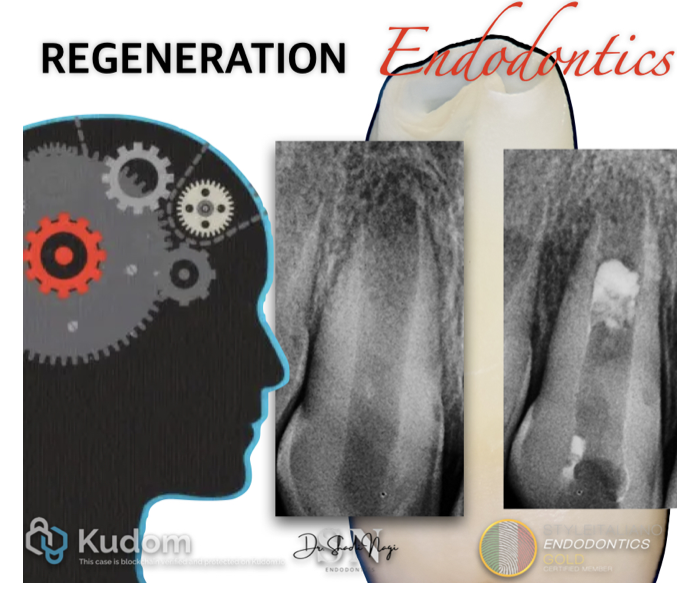
Fig. 2
First Visit Protocol
Follows the recommendations of the American Association of Endodontists (AAE)First Visit Protocol
After administration of local anesthesia and rubber dam isolation, the tooth no 1.1 was accessed with Minimal mechanical debridement or no mechanical instrumentation to preserve the integrity of the thin root canal walls. The canal was gently irrigated with 20 mL of 1.5% sodium hypochlorite (NaOCl), followed by irrigation with sterile saline and 17% EDTA solution to reduce the cytotoxic effects of NaOCl and promote the release of growth factors from dentin. The canal was then dried with sterile paper points.
An intracanal medicament was placed, consisting of either a low-concentration triple antibiotic paste (ciprofloxacin, metronidazole, and minocycline or an appropriate substitute for minocycline) or calcium hydroxide, depending on the clinical situation and esthetic considerations. The access cavity was temporarily sealed with a bacteria-tight restoration, and the patient was recalled after approximately 2–4 weeks (typically 3 weeks) for the second visit, provided the tooth was asymptomatic and clinical signs of infection had resolved.
Fig. 3
Calcium hydroxide (C-Root Cal - C-Root Company) was placed in the middle portion of the canal, away from the apical area, to avoid injury to the stem cells of the apical papilla (SCAP), thereby preserving their Regenerative potential.
Fig. 4
Second Visit Protocol
At the second appointment 2–4 weeks (typically 3 weeks), the tooth was assessed for the absence of clinical signs and symptoms of infection. Following rubber dam isolation and administration of local anesthesia without a vasoconstrictor, the canal was irrigated with 20 mL of 17% EDTA and dried with sterile paper points. Apical bleeding was induced by gently over-instrumenting 2 mm beyond the apical foramen to create an intracanal blood clot , which was allowed to form up to the level of the cementoenamel junction. A collagen matrix was placed over the blood clot, followed by a 3–4 mm layer of MTA.
But In this case, I intentionally placed the MTA in the middle third of the canal to preserve adequate space for a fiber post. This approach was selected because the tooth required post reinforcement, allowing placement of a fiber post to enhance retention and improve the longevity of the direct restoration.
The access cavity was then restored with glass ionomer and a permanent composite restoration.
Follow-up
Clinical and radiographic evaluations were performed at 6, 12, and 18 months. Treatment success was assessed by the absence of symptoms, healing of the periapical lesion, continued root development (increased root length and dentinal wall thickness), apical closure, and, when present, a positive response to pulp vitality testing.
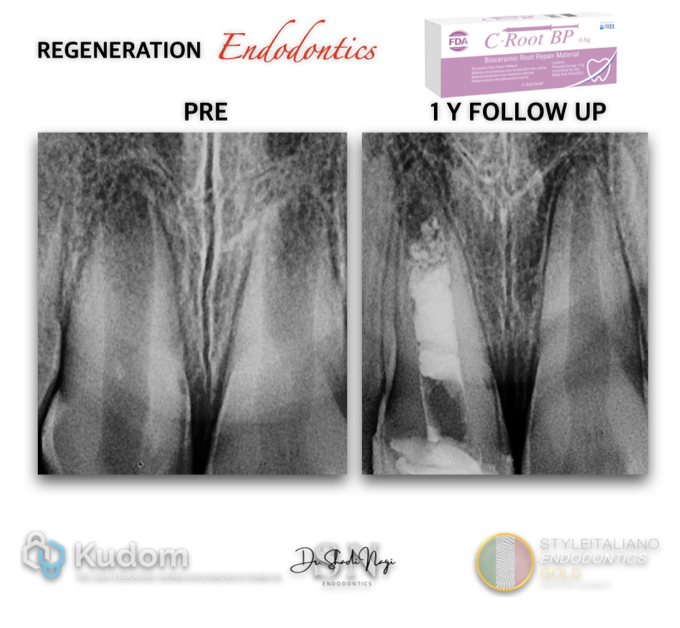
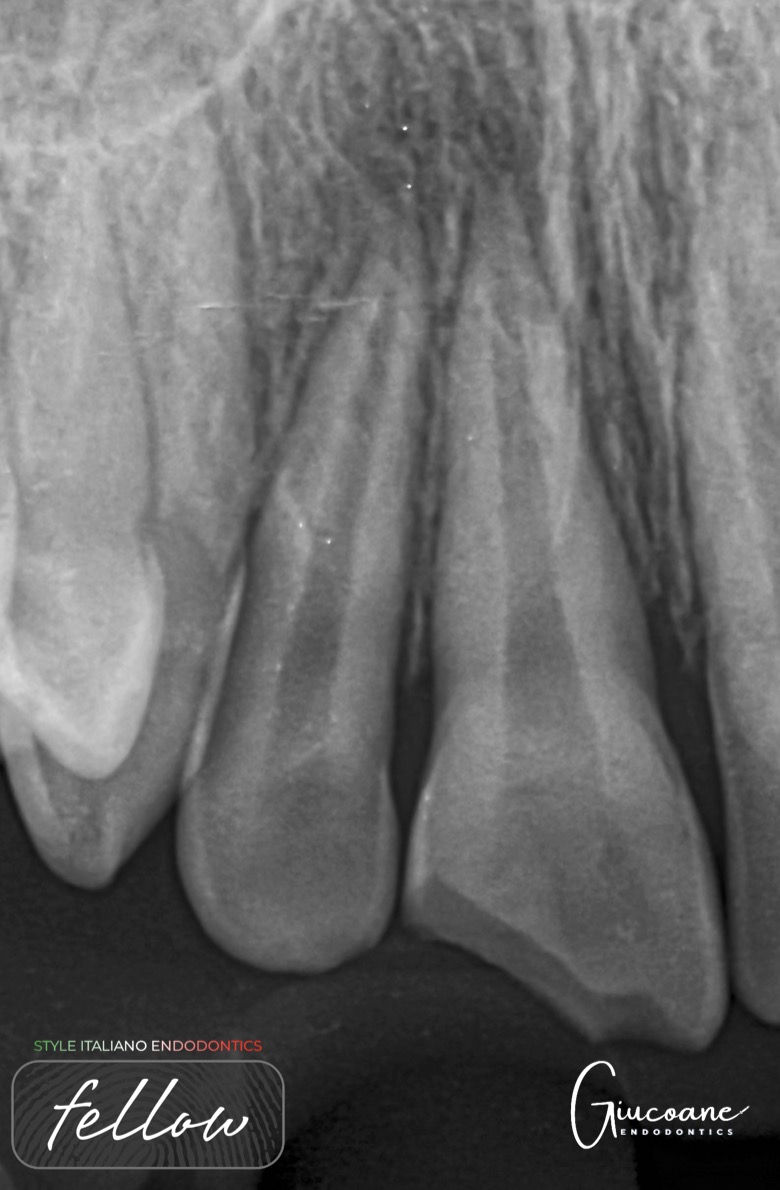
Fig. 5
At the 12-month follow-up, both the Regenerated tooth no 1.1 and the vital tooth no 1.2 exhibited continued root development, increased dentinal wall thickness, apical closure, and positive responses to both cold and electric pulp tests.
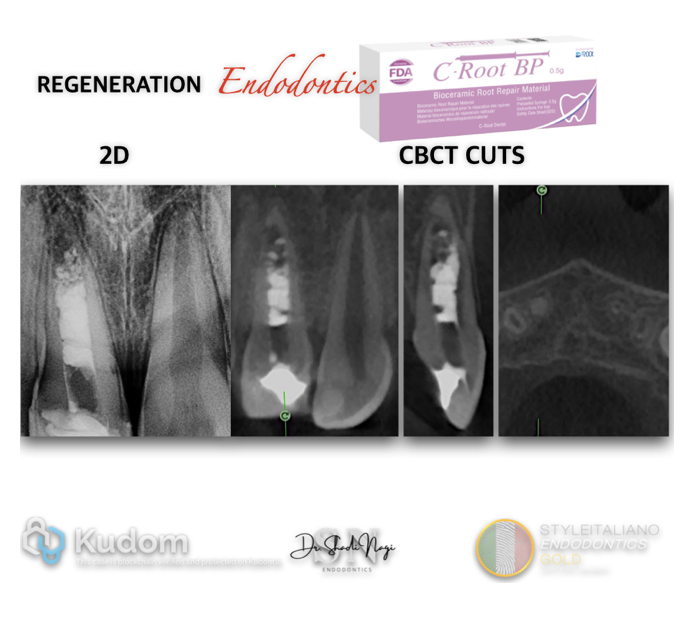
Fig. 6
The follow up post operative radiograph 2D VS 3D
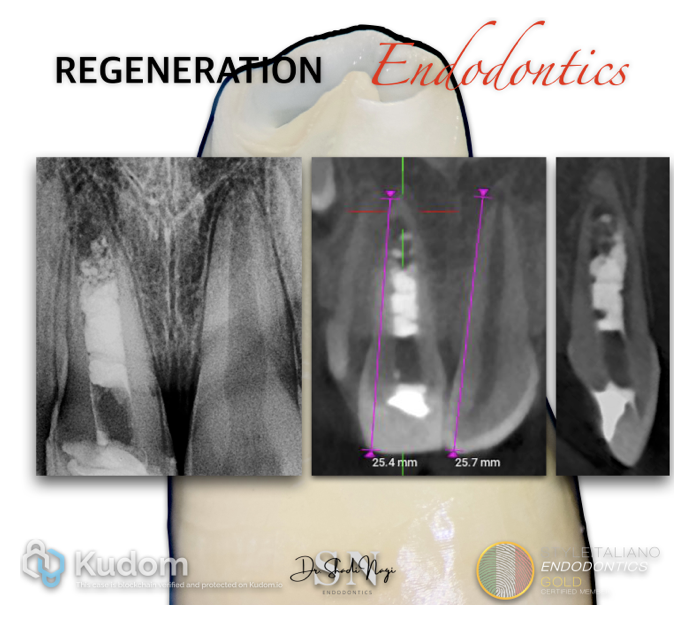
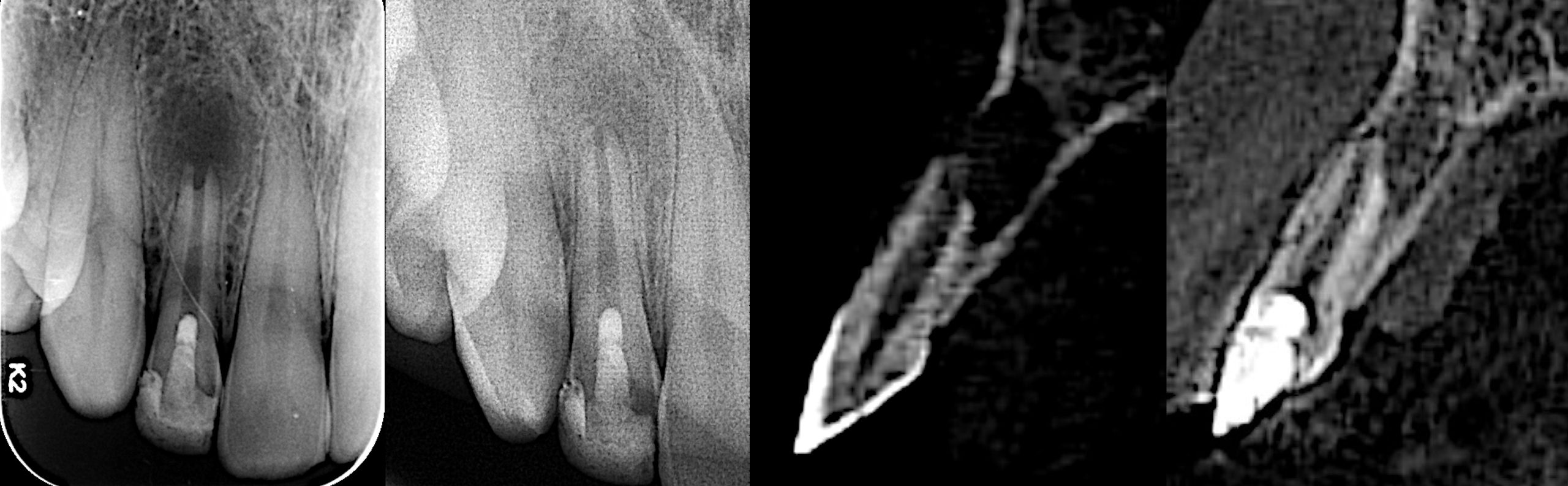
Fig. 7
Follow-up 2D and 3D radiographic assessment demonstrated continued root maturation of the previously necrotic central incisor 1.1 treated with regenerative endodontic therapy. The treated tooth showed a slightly shorter root length than the adjacent vital central incisor 1.2 , emphasizing the effectiveness of a proper regenerative protocol in achieving intentional physiologic root maturation.
Conclusions
Regenerative endodontic procedures (REPs) represent a predictable, biologically based treatment option for immature permanent teeth with pulp necrosis following trauma. In the present case, successful clinical and radiographic outcomes were achieved, including healing of the periapical lesion, continued root maturation, increased dentinal wall thickness, apical closure, and recovery of pulp sensibility.
However, complete root maturation is not essential outcome for successful treatment. Clinical success can be achieved through the resolution of infection and periapical healing, even without significant root lengthening, dentinal wall thickening, apical closure, or recovery of pulp sensibility. Therefore, the primary goal of REPs is the elimination of disease and preservation of the tooth, while continued root development and pulp sensibility are considered desirable, but not mandatory, outcomes.
Careful case selection and thorough discussion with parents or guardians regarding all available treatment options, expected outcomes, and the evidence-based success rates of REPs are essential for informed decision-making and optimal patient care.
Bibliography
- Murray PE, Garcia-Godoy F, Hargreaves KM.
Regenerative Endodontics: A Review of Current Status and a Call for Action.
Journal of Endodontics. 2007;33(4):377–390. - Galler KM, Krastl G, Simon S, et al.
European Society of Endodontology Position Statement: Revitalization Procedures.
International Endodontic Journal. 2016;49(8):717–723.
- American Association of Endodontists (AAE).
Clinical Considerations for a Regenerative Endodontic Procedure. (2022 Update)
Official Guideline: - Wei X, Yang M, Yue L, et al.
Expert Consensus on Regenerative Endodontic Procedures.
International Journal of Oral Science. 2022;14:55.
- Kontakiotis EG, Filippatos CG, Tzanetakis GN, Agrafioti A.
Regenerative Endodontic Therapy: A Data Analysis of Clinical Protocols.
Journal of Endodontics. 2015;41(2):146–154.