Real time detection of the working length: how many advantages does it bring to the dentist?
09/05/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Post-operative pain in endodontics has been widely associated with the extrusion of debris beyond the apical foramen.
During mechanical preparation, dentinal chips, pulp tissue remnants, bacteria, and irrigants may be inadvertently pushed into the periapical tissues. This extrusion can trigger an acute inflammatory response, leading to pain and discomfort after treatment.
The extent of this phenomenon depends on several factors, including instrumentation technique, file design, and irrigation protocols.
Studies have shown that aggressive or poorly controlled shaping increases the risk of apical extrusion. Conversely, crown-down approaches and modern rotary or reciprocating systems tend to reduce debris displacement.
The presence of pre-existing periapical inflammation may further exacerbate the patient’s perception of pain.
Limiting extrusion is essential not only for patient comfort but also for optimal healing, therefore operator skill and working length control are critical in minimizing this complication.
Overall, careful biomechanical preparation remains a key determinant of post-operative outcomes. The use of an endodontic motor with an integrated apex locator offers a significant clinical advantage because it allows continuous and real-time monitoring of the working length during instrumentation. This improves accuracy in maintaining preparation within the apical constriction, reducing the risk of over-instrumentation and debris extrusion.
Ultimately, this contributes to a more predictable treatment outcome and enhanced patient comfort.

Fig. 1
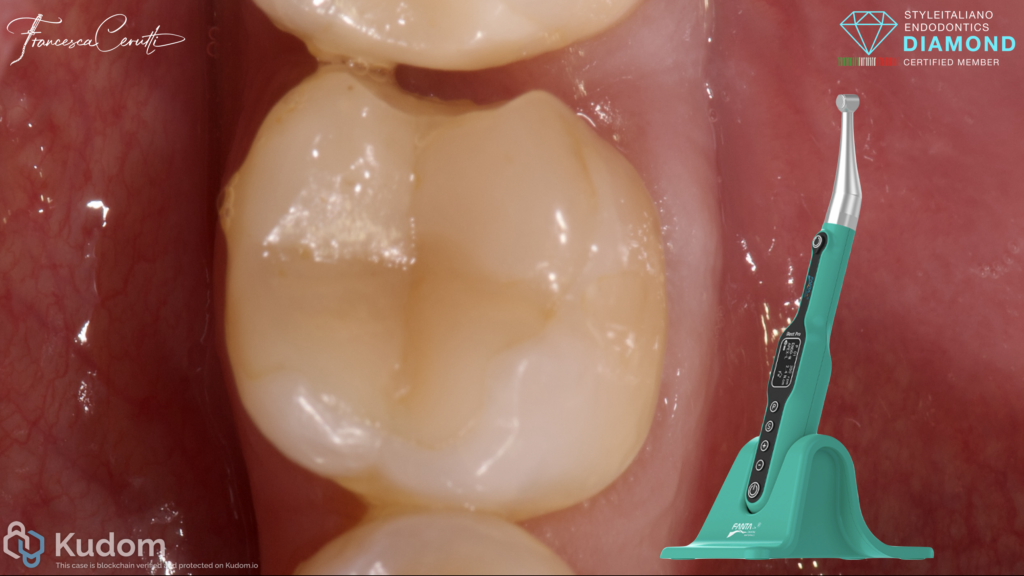
A patient came complaining about spontaneous, intense and non subsiding pain on the lower left semi-arch. He referred he suffered from food impaction in the last months and that he probably broke a restoration.

Fig. 2
The lack of contact between the teeth due to the broken restoration probably led to the food impaction and secondary decay.
After administering the anesthesia, I isolated the tooth with rubber dam.
Fig. 3
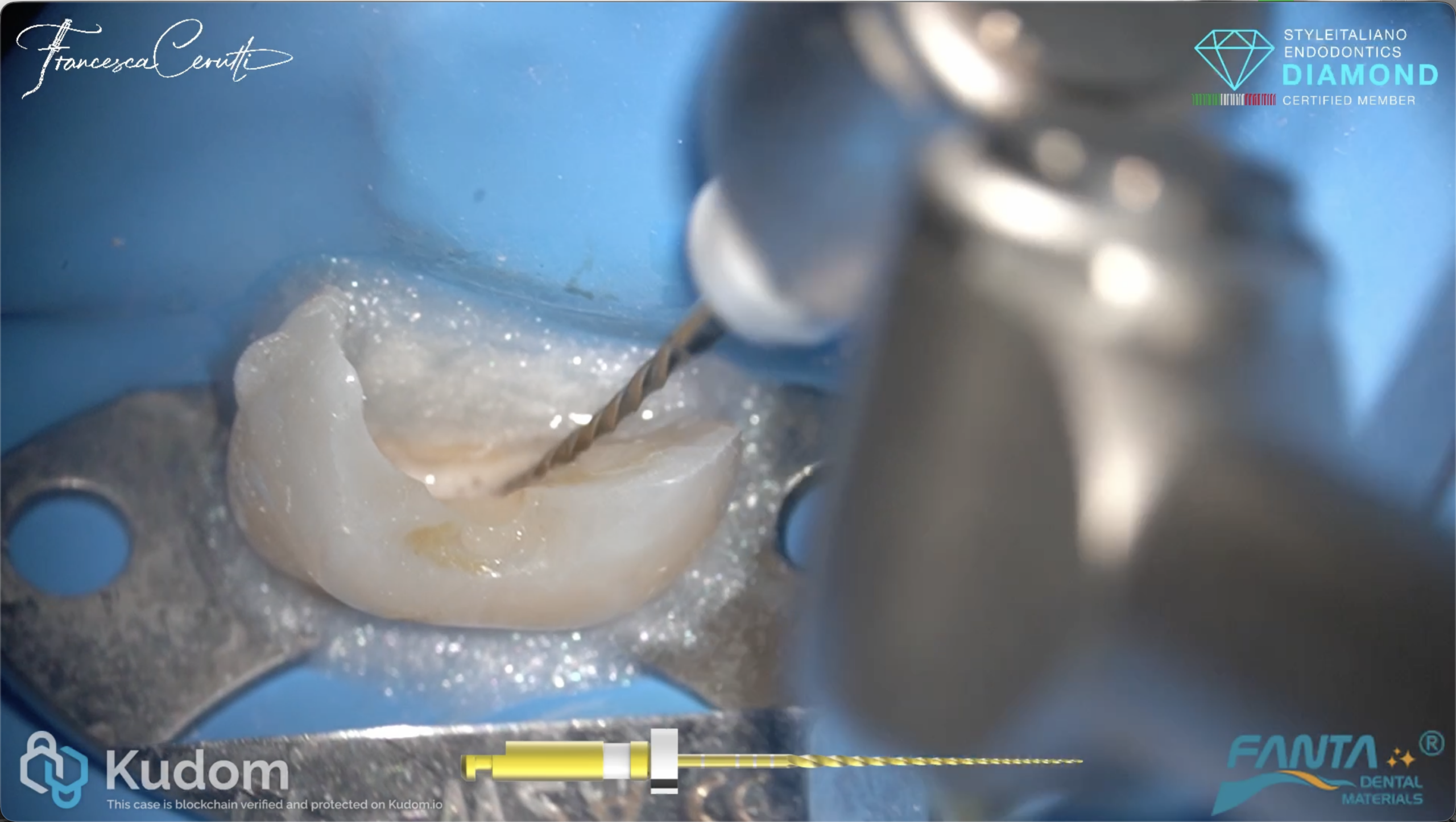
The tooth had 5 root canals. I shaped with rotary files, leaving the manuals only to confirm the working length radiographically for insurance reasons.
iRoot Pro allows the operator to be fully in control of the shaping phase of the root canal system. The motor is fully customizable, so one can select the type of motion, speed, torque, etc.
I personally always use it enabling the apex locator function, in order to speed up my work and to reduce to the maximum the extrusion of debris and the chance to overextend the shaping.
It is compatible with most of the files on the market and it is extremely light-weight.

Fig. 4
I shaped the root canals and then dedicated myself to the cleaning step.

Fig. 5
I filled the root canal system with hydraulic sealer and gutta percha
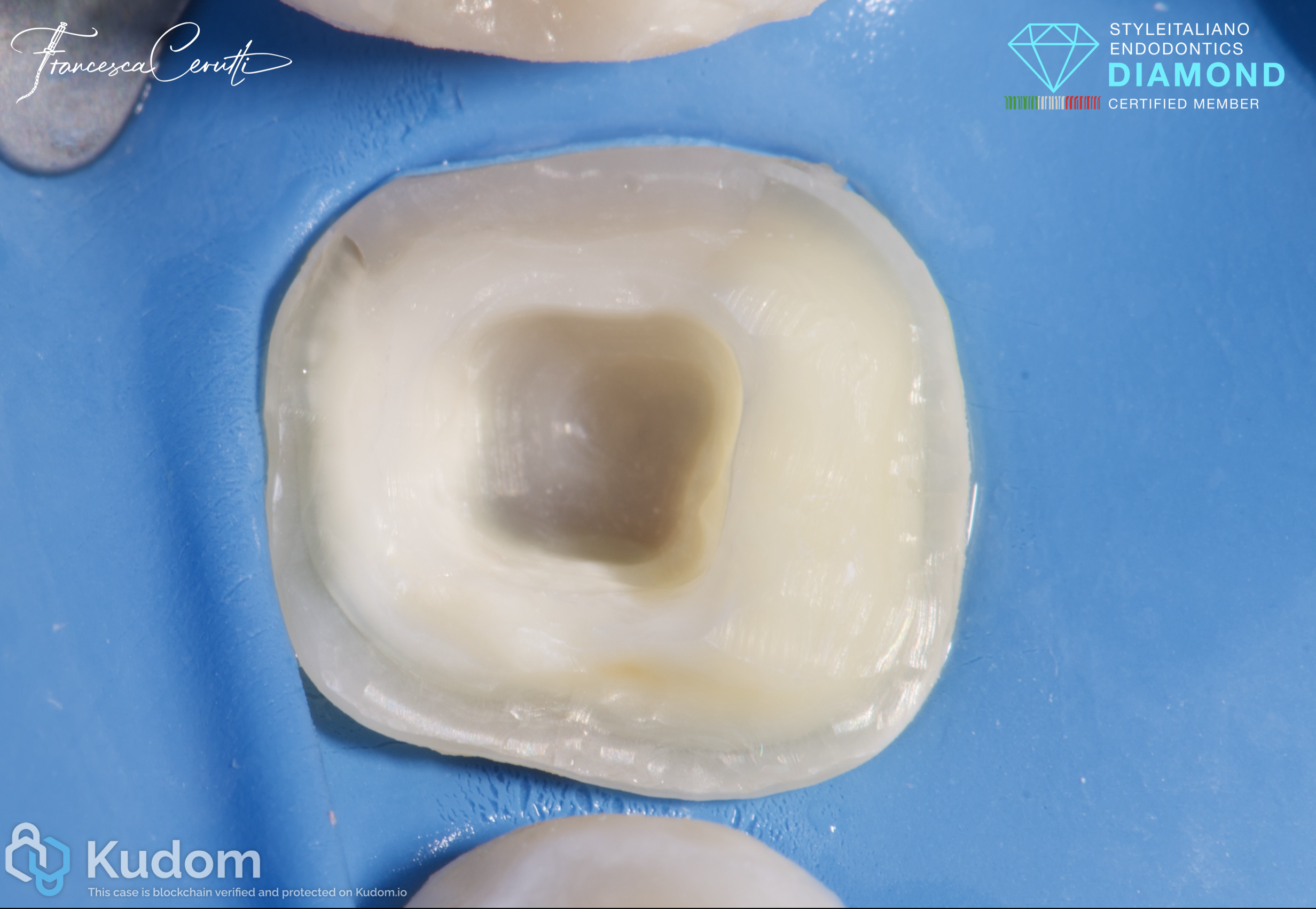
Fig. 6
I immediately sealed the cavity with composite and prepared for an endocrown. Subsequently, I scanned and put a temporary restoration.

Fig. 7
Immediate post operative X-ray

Fig. 8
The endocrown before luting

Fig. 9
After removing the rubber dam

Fig. 10
Post operative X-ray. The patient reported zero pain between the appointments, the tooth was asymptomatic and in function.
Conclusions
Using a device like iRoot Pro, that allows to shape smoothly while always keeping the working length under control, allows reducing the post operative pain after root canal treatment.
Bibliography
- Seltzer S, Naidorf IJ. Flare-ups in endodontics: I. Etiological factors. J Endod. 1985.
- Tanalp J, Güngör T. Apical extrusion of debris: a literature review of an inherent occurrence during root canal treatment. Int Endod J. 2014.
- Bürklein S, Schäfer E. Apically extruded debris with reciprocating single-file and full-sequence rotary instrumentation systems. J Endod. 2012.
- Caviedes-Bucheli J et al. The influence of two reciprocating single-file and two rotary-file systems on the apical extrusion of debris and its biological relationship with symptomatic apical periodontitis. Int Endod J. 2016.
- Ricucci D, Siqueira JF Jr. Apical limit of root canal instrumentation and obturation, part 1. Literature review. Int Endod J.1998.
- Tsesis I et al. Post-operative pain after endodontic treatment: a systematic review. Int Endod J. 2008.
- ElAyouti A et al. Influence of instrumentation length on apical extrusion of debris. J Endod. 2005.
- Gordon MPJ, Chandler NP. Electronic apex locators. Int Endod J. 2004.
- de Camargo EJ et al. Accuracy of electronic apex locators in detecting apical constriction: a systematic review. J Endod.2009.
- Ng YL, Mann V, Gulabivala K. Outcome of primary root canal treatment: systematic review. Int Endod J. 2007.