
Radix entomolaris: Management of vital pulp therapy failure
18/08/2020
Ahmed Shawky
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Vital pulp therapy (VPT) are those procedures carried out to maintain the dental pulp in a healthy condition, allowing to preserve its defensive function and sustaining its ability to form dentin in response to irritation. Despite the favorable outcomes of VPT, some complications might occur as a result of improper case selection or technical factors.
Recent studies reported successful outcomes of vital pulp therapy in mature teeth with irreversible pulpitis. A major concern in VPT in mature teeth is the incidence of pulp space obliteration, especially after full pulpotomy. This condition will present a drastic complication if the treated tooth developed apical periodontitis that would necessitates endodontic treatment. In the presence of complex anatomy, pulp space calcification might alter the internal anatomy making it extremely difficult to manage with a high possibility of incidence of intra-treatment mishaps.
The aim of this article is to present management of failed calcium hydroxide pulpotomy in a mature mandibular first molar having a Radix Entomolaris.

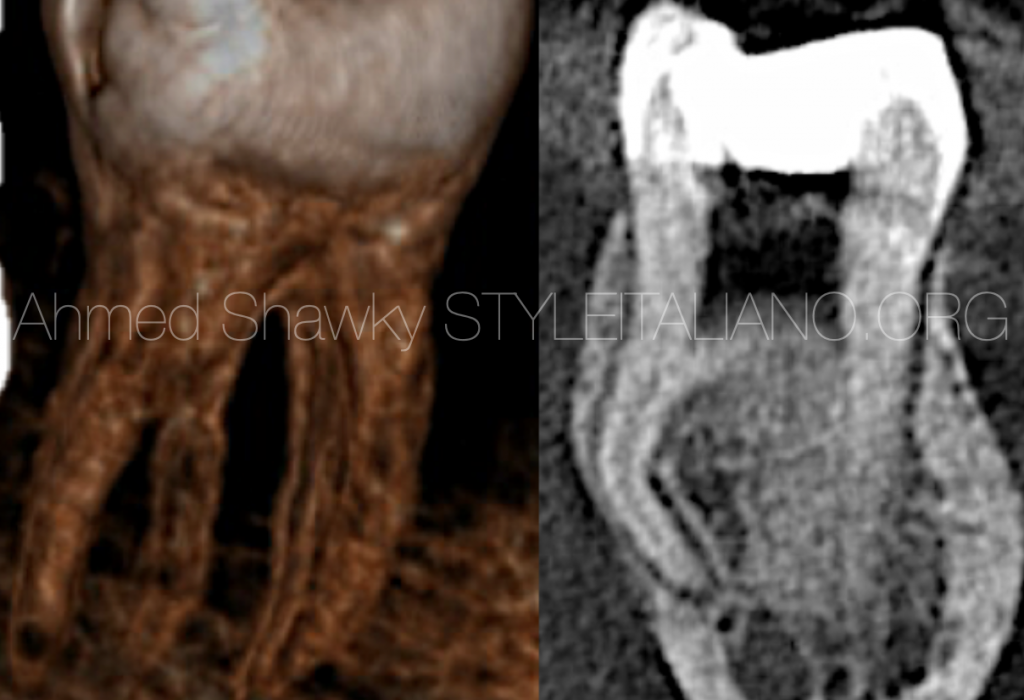
Fig. 1
An 11 years old male was referred from a pediatric dentist, complaining of symptomatic apical periodontitis in a mandibular first molar. The referring dentist provided the history of calcium hydroxide pulpotomy in this mature molar 2 months earlier without proper tooth isolation.
Radiographic examination revealed the presence of a Radix Entomolaris (RE) and partial obliteration in the pulp space.
Access preparation was performed in the first visit under complete isolation. Negotiation of anatomy was not possible except in the DB root due to calcification. Therefore, a small field of view CBCT scan, with high resolution was requested.
CBCT navigation revealed;
- Calcified mesial canal orifices
- The presence of a RE with calcified orifice and sharp mid root curvature
- The presence of a very thin mesial root with a middle mesial anatomy in the form of a fin configuration.
- Presence of a well developed apical periodontitis under all roots and a lateral radiolucency on the mesial side of the mesial root.
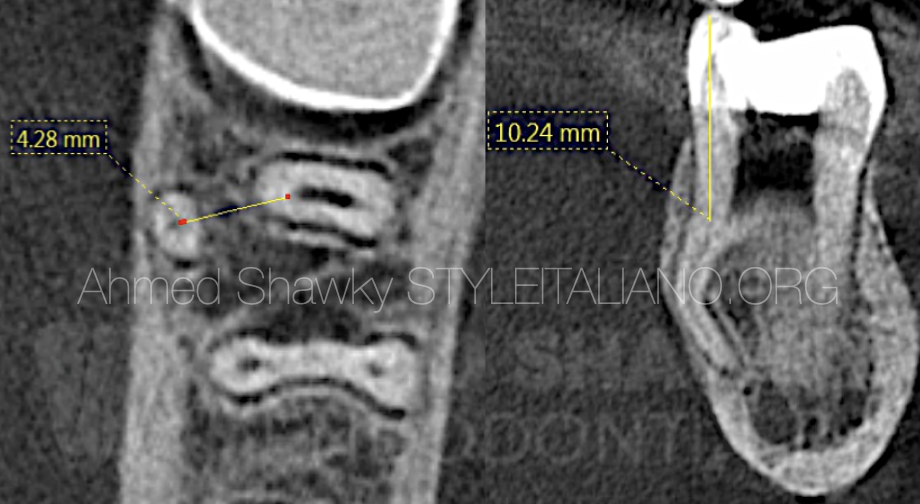
Fig. 2
CBCT Assessment and treatment planning
Navigation of the axial and coronal views revealed that the patent part of the root canal was more than 10mm apical to the respective coronal reference point. This will necessitate deep troughing using adapted ultrasonic tips.
Evaluation of the RE revealed an inter-orifice distance of more than 4mm from the main distal root components in the lingual direction. This location of the RE will need deep troughing with ultrasonics almost beyond the lingual contour of the tooth.
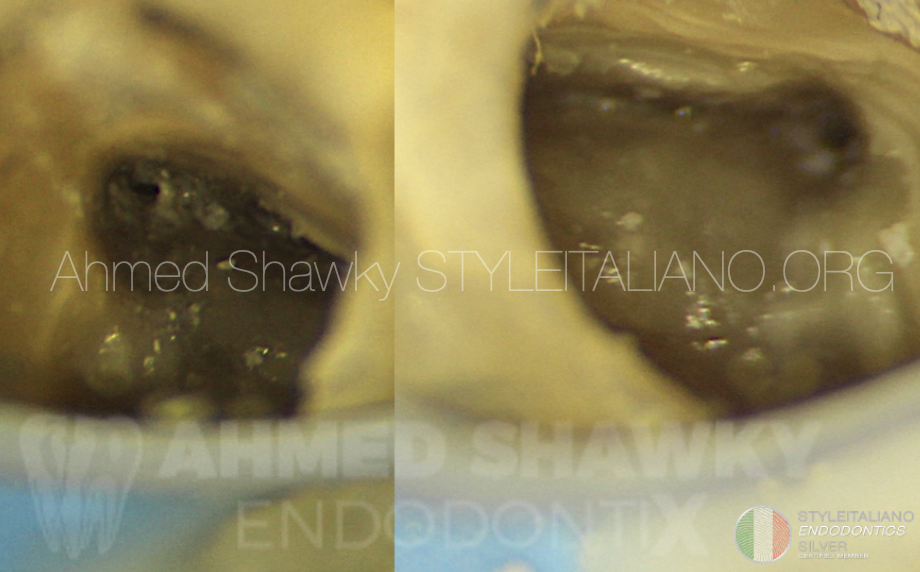
Fig. 3
Ultrasonic deep troughing:
A long .03 tapered ultrasonic tip is thinned using a metal polisher to reduce the taper and making it readily bendable and adaptable to the predetermined troughing sites. Deep troughing is made under high magnification until the orifices were clearly discernible.
Patency was confirmed using an apex locator and a #10 catheterization file.
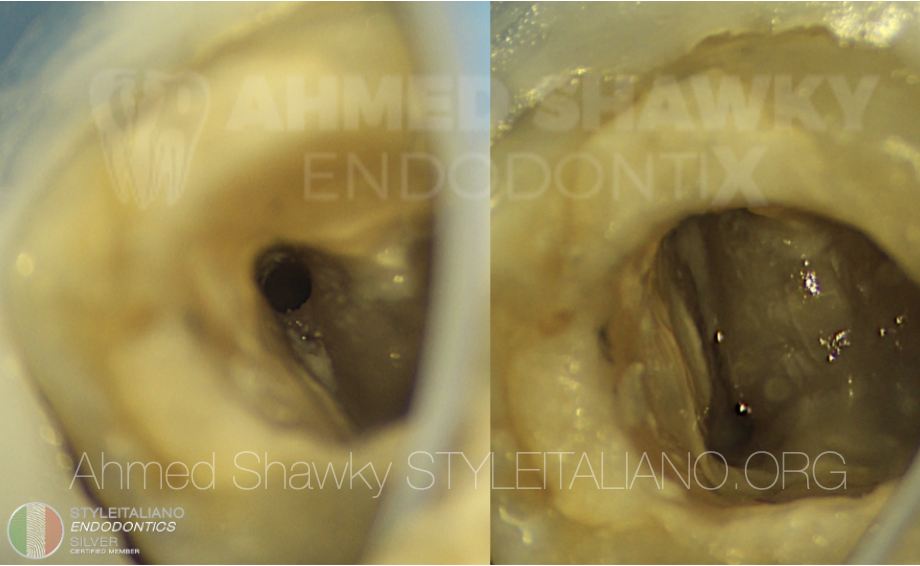
Fig. 4
Shaping and cleaning of the mesial system:
The mesial root canals were shaped in a step-down manner using regressive tapered instruments to minimize dentin removal in the mesial root. Step-wise ultrasonic activation of sodium hypochlorite and EDTA was done interchangeably to reach the middle mesial fin as much as possible and in the same time facilitate shaping of the narrow root canals.

Fig. 5
Management of the radix entomolaris:
A modified ultrasonic tip was pre-bent in a lingual direction at the predetermined depth obtained from CBCT scan. Troughing was done under high magnification at an arbitrarily predetermined distance from the main distal canals, until a catch could be obtained with a DG16 explorer and a #8 catheterization file. Mechanical glide path was performed without the use of any manual files. Working length of RE was established at the final step of instrumentation.
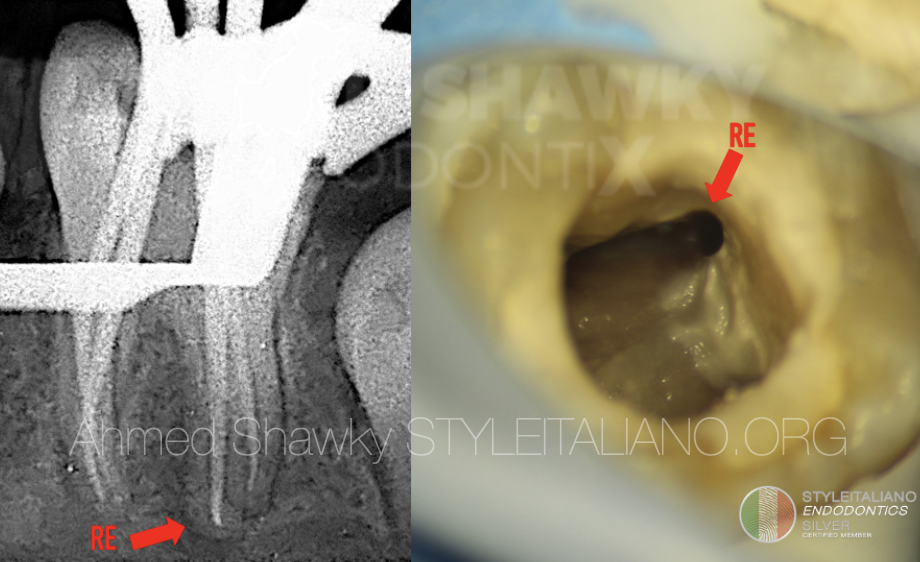
Fig. 6
Instrumentation of the radix entomolaris:
Mechanical glide path was performed without the use of any manual files. Working length of RE was established at the final step of instrumentation. Cone fit and gauging was confirmed radiographically.
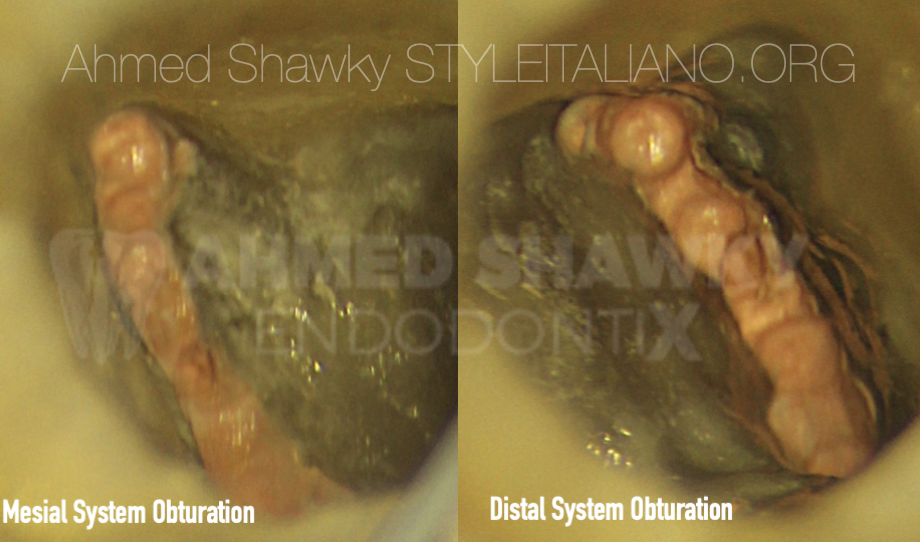
Fig. 7
Bioceramic sealer and warm gutta percha:
Obturation of the root canal system was done using warm gutta percha and a heat-compatible Bioceramic sealer. It has to be noted that careful adjustment of the heat pluggers setting and depth should be done so as not to cause alteration in the physical and chemical properties of the Bioceramic material.
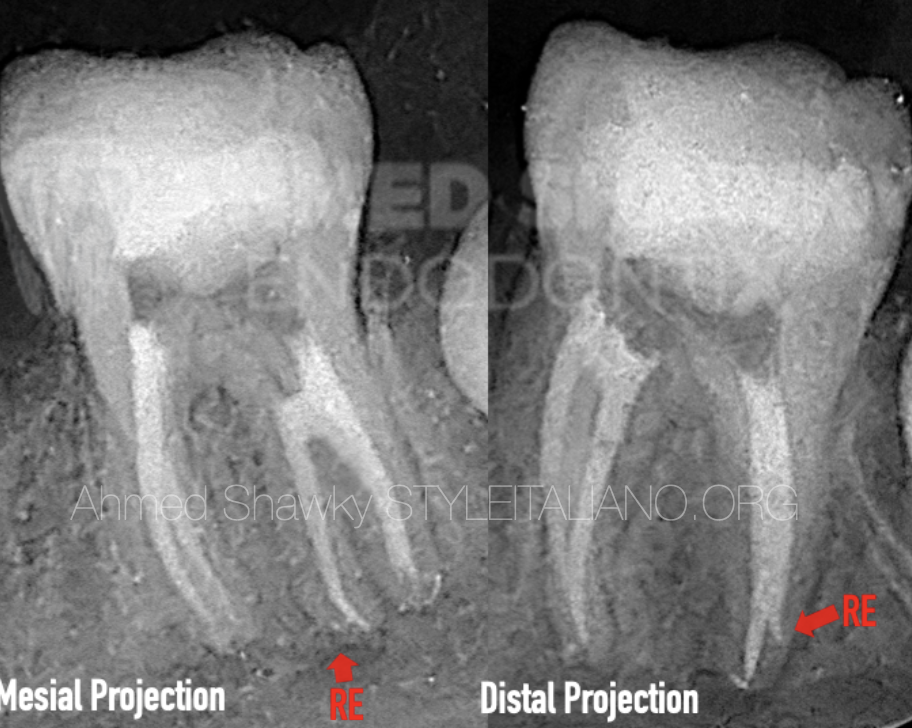
Fig. 8
Post-operative data:
Mesial and distal shifted projections were used to obtain the post-operative image. Mesial projection revealed complex apical anatomy of the DB root. This image also shows the extremely deep troughing that was made to negotiate the RE.
The mesial projection showed that the coronal isthmus was adequately cleaned and obturated. The patient reported resolution of symptoms of apical periodontitis with 72 hours from obturation.
Conclusions
- The success in VPT is strongly dependent upon proper case selection, strict field isolation and proper selection of the inductive/sealing material
- In case of pulp space calcification, proper planning using CBCT is essential wether in the pre-treatment or intra-treatment phase to avoid incidence of aggressive procedural accidents.
- The use of high magnification and illumination during management of pulp space calcification is essential. The blind use of ultrasonics or their use with low magnification should be discontinued especially with calcified root canal systems.
- Radix entomolaris is a challenging anatomy in mandibular first molars. In most cases, the RE is severely curved with difficult access due to its distolingual position
Bibliography
1- European Society of Endodontology position statement: Management of deep caries and the exposed pulp. International Endodontic Journal, 52, 923–934, 2019
2-Vital pulp therapy of mature permanent teeth with irreversible pulpitis from the perspective of pulp biology. Aust Endod J 2020; 46: 154–165
3- The Radix Entomolaris and Paramolaris: Clinical Approach in Endodontics. J Endod 2007;33:58–63
4- Root Canal Morphology of Permanent Three- rooted Mandibular First Molars—Part I: Pulp Floor and Root Canal System J Endod 2010;36:990–994
5- The Radix Entomolaris and Paramolaris: A Micro–Computed Tomographic Study of 3-rooted Mandibular First Molars. http://dx.doi.org/10.1016/j.joen.2014.03.012



