Radix Entomolaris - Case series and clinical considerations
26/05/2017
Filippo Cardinali
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Many of the difficulties found in root canal treatment are due to variations in root canal morphology (1). Root canal morphology is limitless in its variability and clinicians must be aware that anatomic variations constitute a formidable challenge to endodontic success (2). First reported by Carabelli in 1884 (4), this extra root, that is generally shorter than the disto-buccal root and is usually curved, was named by Bolk “radix entomolaris” (5). The relevant literature revealed an incidence of <5% in Caucasian, African, Eurasian and Indian populations, whereas in those with Mongoloid traits, such as Chinese, Eskimo and Native American populations, the RE occurs with a frequency of 5% and even up to 40% (6-10).
De Moore et al. (6) classified RE based on the curvature of the root or root canal in bucco-lingual orientation, Carlson and Alexandersen (10) classified four types of RE (A, B, C, and AC), based on the location of the cervical portion of the root and this helps in identification of separate and non separate RE; Song et al. (11) have suggested a new classification based on morphologic characteristics assessed from cross-sectional computed tomography technique (Img. 1).
Extra roots as the Radix Entomolaris in mandibular molars, are an additional challenge, which begins at case assessment and involves all operative stages; that’s why an early detection of the presence of any anatomical variations is essential to let the clinician choose the best operative strategy in terms of access cavity design, root canal opening localization, canal shaping, filling and restorative techniques (12). Thus, an awareness and understanding of root canal anatomy is essential to carry out a safe shaping respectful of the original endodontic anatomy for improving the predictability of root canal treatment.
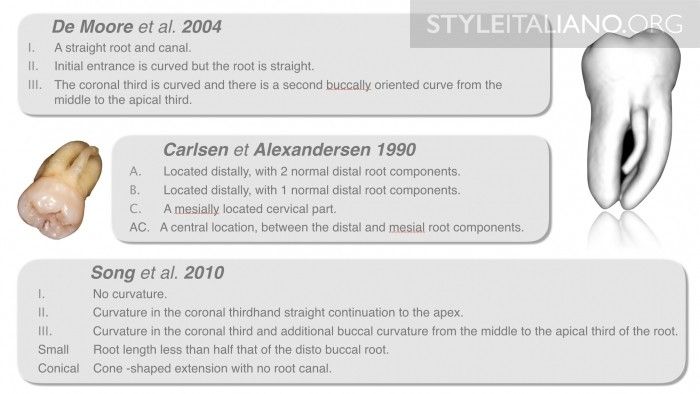
Fig. 1
The table shows the classification of Radix Entomolaris

Fig. 2
Preoperative detection of RE: Rx examination It is very easy to detect thanks a CBCT scan, though, most of the time, clinicians should try to intercept the presence of the RE by analyzing a bi-dimensional exam in the first place. As the (separate) DL root is usually situated in the same BL plane as the DB root, a superimposition of the two roots may appear on the preoperative radiograph, which may result in difficulty identifying this additional root: the clinician has to look very carefully for the presence of another PDL close to the distal root. A preoperative angled radiograph is useful to avoid the superimposition of the 2 distal roots and clearly see the Radix entomolaris.
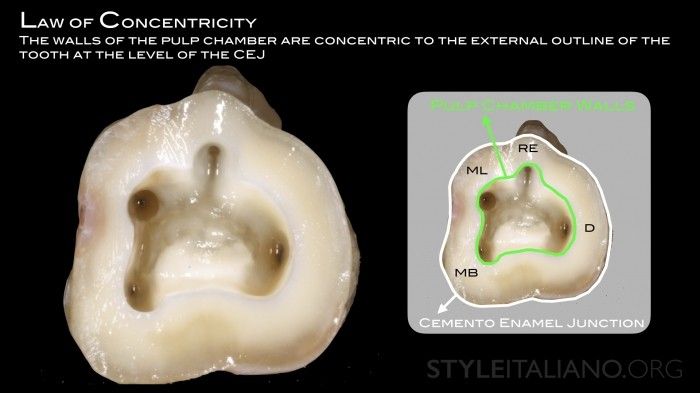
Fig. 3
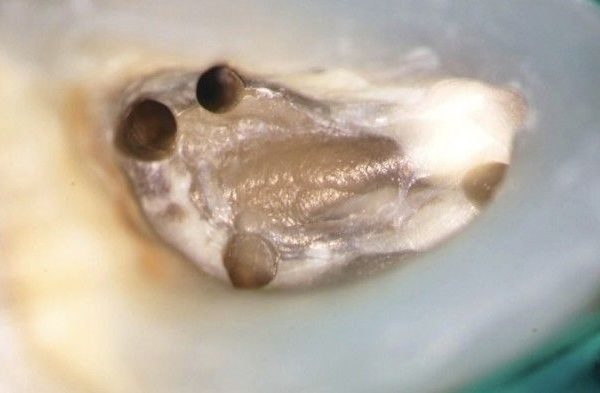
Preoperative detection of RE: clinical examination At a clinical examination, the probing to the level of the CEJ could be useful to diagnose the presence of the RE. According Krasner and Rankow (13), the walls of the pulp chamber are concentric to the external outline of the tooth at the level of the CEJ; so, if there is a bulge of the CEJ in disto-lingual for the presence of the RE, the pulp chamber also will extend in that direction. Application of Krasner and Rankow Laws eases the creation of a proper access that facilitates the orifice localization of the RE.
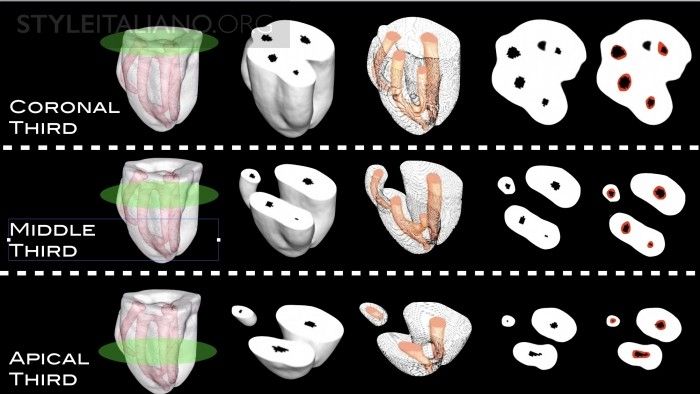
Fig. 4
RE & Shaping. The Radix Entomolaris is a challenge under a shaping point of view: it is thin and curved, so that a very careful shaping procedure is required in order to avoid iatrogenic damage, such as stripping, internal/external transportation, ledge and apical foramen transportation. In this case, a step-down technique has been used: the superimposition of tooth sections at the same level before (black spot) and after shaping (red spot), shows how the rotary file worked in the center of the canal.
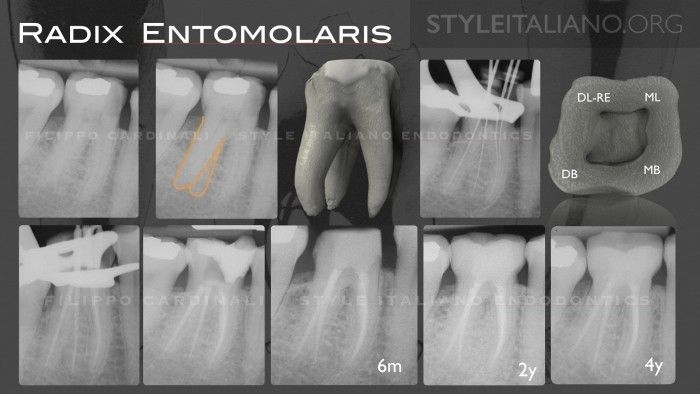
Fig. 5
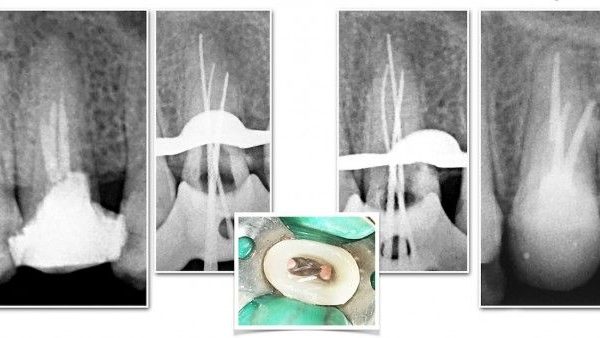
Clinical case n 1. Female 62 years-old. The presence of RE has been diagnosed at Rx examination. Intraoperative Rxs are useful to better understand the anatomy of the RE. Follow-up at 2 and 4 years.

Fig. 6
Clinical case n 2. Male, 54 years-old. The presence of a RE has been diagnosed at clinical examination, thanks the probing at CEJ level. 2 years follow-up.

Fig. 7
Clinical case n 3. Male, 56 years old. The presence of RE has been diagnosed at Rx examination and confirmed at clinical examination, thanks the probing at CEJ level. Mesial angled Rx at 1 year follow-up and distal angled Rx at 3 years follow-up.
Conclusions
Clinicians should have thorough knowledge of the endodontic anatomy and its possible variations. The initial diagnosis of a Radix Entomolaris before root canal treatment is important to facilitate the endodontic procedure, and to avoid missed canals that lead to a failure of the therapy.
Bibliography
Soares JA, Leonardo RT. Root canal treatment of three-rooted maxillary first and second premolars-a case report. International Endodontic Journal 2003; 36: 705-710.
Slowey RR. Radiographic aids in the detection of extra root canals. Oral Surg Oral Med Oral Pathol 1974;37(5):762-72.
Carabelli G. Systematisches Handbuch der Zahnheilkunde. 2nd ed. Vienna. Braumuller und Seidel, 1884: 114.
Bolk L. Bemerküngen über Wurzelvariationen am menschilchen unteren Molaren. Zeitung fur Morphologie und Anthropologie 1915: 17, 605-10.
Gulabivala K, Aung TH, Alavi A, Ng YL. Root and canal morphology of Burmese mandibular molars. Int Endod J 2001;34:359-70.
De Moor RJ, Deroose CA, Calberson FL. The radix entomolaris in mandibular first molars: An endodontic challenge. Int Endod J 2004;37:789-99.
Tu MG, Tsai CC, Jou MJ, Chen WL, Chang YF, Chen SY, et al. Prevalence of three-rooted mandibular first molars among Taiwanese individuals. J Endod 2007;33:1163-6.
Chen G, Yao H, Tong C (2009a) Investigation of the root canal configuration of mandibular first molars in Taiwan Chinese population. International Endodontic Journal 42, 10449.
Huang RY, Cheng WC, Chen CJ, Lin CD, Lai TM, Shen EC, et al. Three-dimensional analysis of the root morphology of mandibular first molars with distolingual roots. Int Endod J 2010;43:478-84.
Carlsen O, Alexandersen V. Radix entomolaris: Identification and morphology. Scand J Dent Res 1990;98:363-73.
Song JS, Choi HJ, Jung IY, Jung HS, Kim SO (2010) The prevalence and morphologic classification of distolingual roots in the mandibular molars in a Korean population. Journal of Endodontics 36, 6537.
Cardinali F, Cerutti F, Cerutti A, Tosco E. Preoperative diagnosis of a third root canal in first and second maxillary premolars: a challenge for the clinician. ENDO (Lond Engl) 2009; 3(1): 51-57.
Krasner P, Rankow HJ. Anatomy of the pulp chamber floor. J Endodon 2004; 30(1):5.