Premolar Endodontics
08/03/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
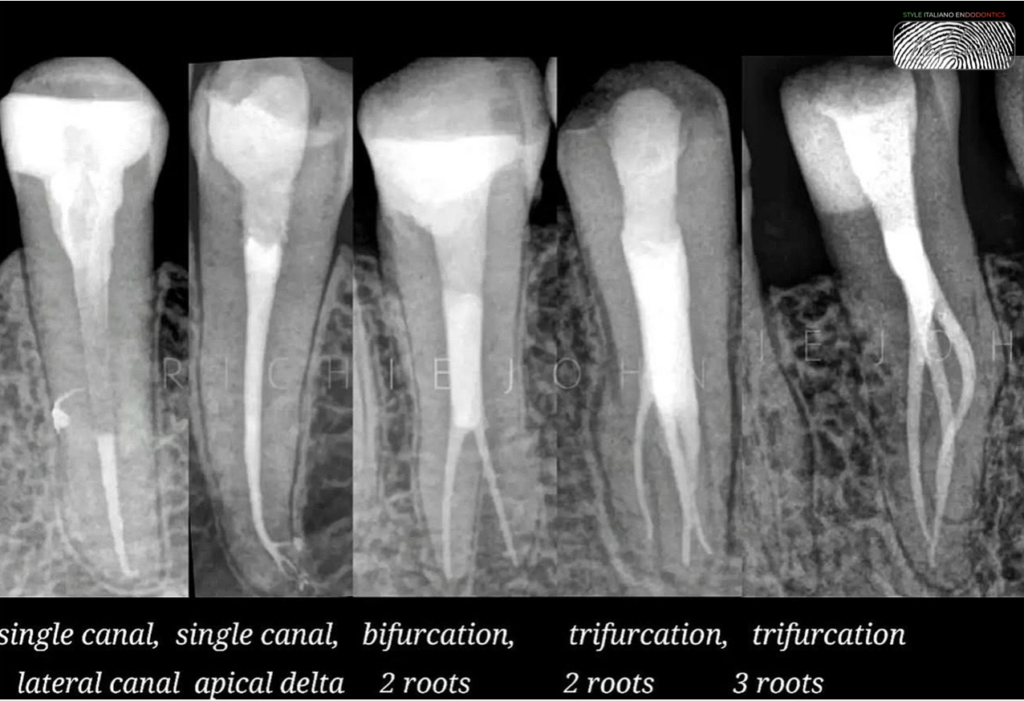
Premolars are often referred to as the "enigma" of endodontics due to their unique and variable anatomy and are notoriously challenging for seasoned endodontists due to their complex and unpredictable anatomy. Variations in root and canal morphology, including the ones with a single canal may have deep splits, fused roots or even three to four canals, making treatment planning and execution difficult. Moreover, premolars’ relatively small size demands precise technique and instrumentation. Mastering premolar endodontics requires extensive knowledge, technical skill and experience. Even the best of battle tested endodontists approach premolars with caution, recognizing the unique challenges they pose. These complexities require the clinician to be highly skilled and adaptable, using advanced techniques and technologies to successfully navigate these enigmatic teeth. Effective treatment of these enigmatic teeth necessitates a deep understanding of their anatomy and creative problem-solving capacity.

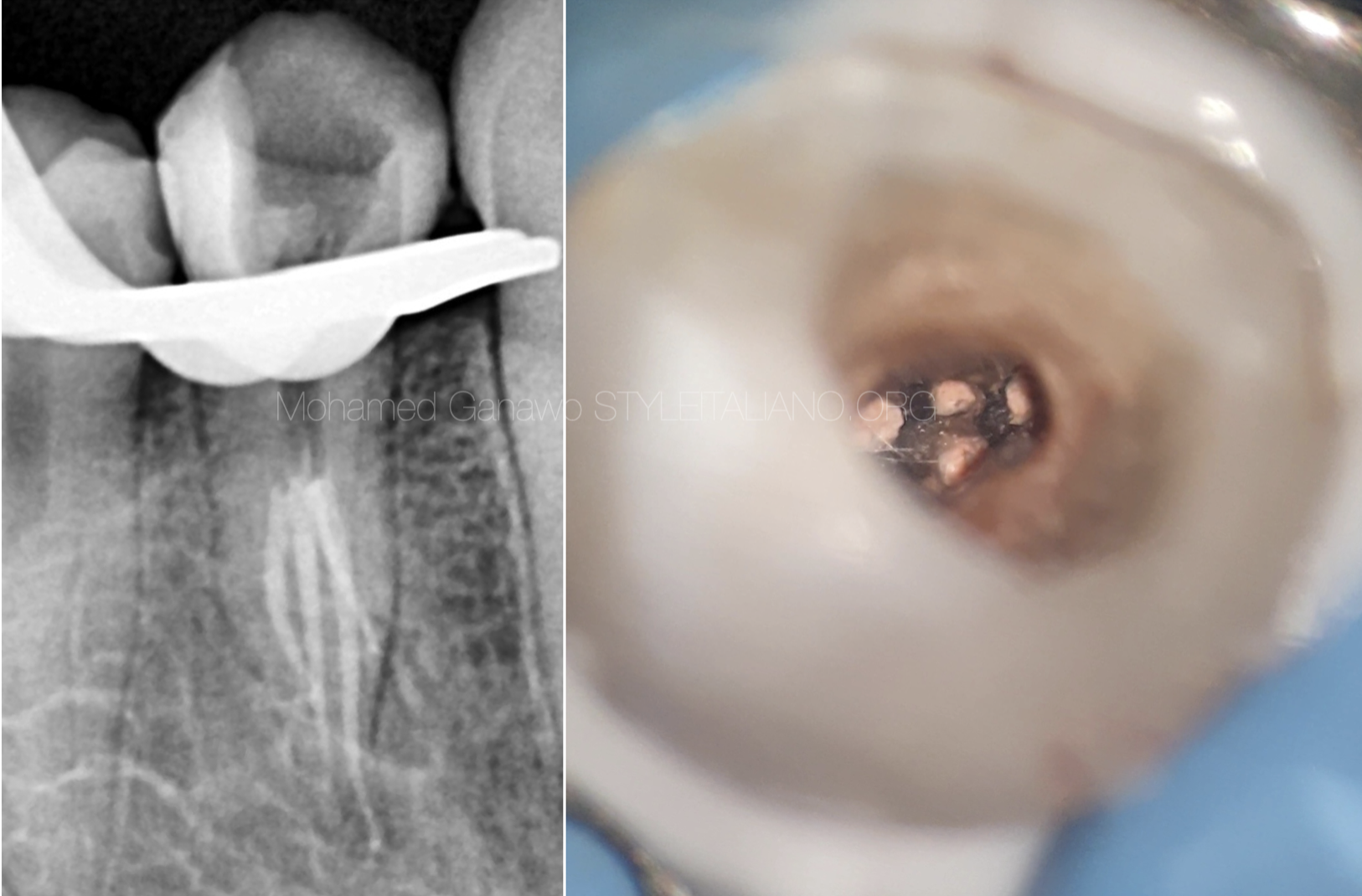
Fig. 1
Discussion:
Mandibular first premolars are typically single-rooted, occurring in approximately 97.1% of cases. While bifurcated roots are relatively uncommon at 2.7%, the presence of three roots is extremely rare, with an incidence of 0.2%.¹ A time-tested Washington study on endodontic treatment outcomes in mandibular premolars reported a notable failure rate of 11.45% specifically for mandibular first premolars.² The roots and/or root canals of these teeth often divide in the middle to apical thirds, making it challenging to detect these anatomical variations. ³ The third root, often smaller and more distally located, can be easily missed during endodontic treatment. This tricky distal canal orifice extends into the axial wall of a tooth rather than being present on the pulpal floor due to a dentinal shelf and quite naturally has an acute angle of entry into the canal, creating difficulty for the clinician to locate or to catheterize the canal. A Dental Operating Microscope and a narrow Field Of View(5x5) Cone Beam Computed Tomography scan are important tools aiding the treatment of such complexity.
Case presentation- Dx: Symptomatic Irreversible pulpitis with Symptomatic apical periodontitis in relation to 44(fdi)
56-year-old male, ASA1 patient.
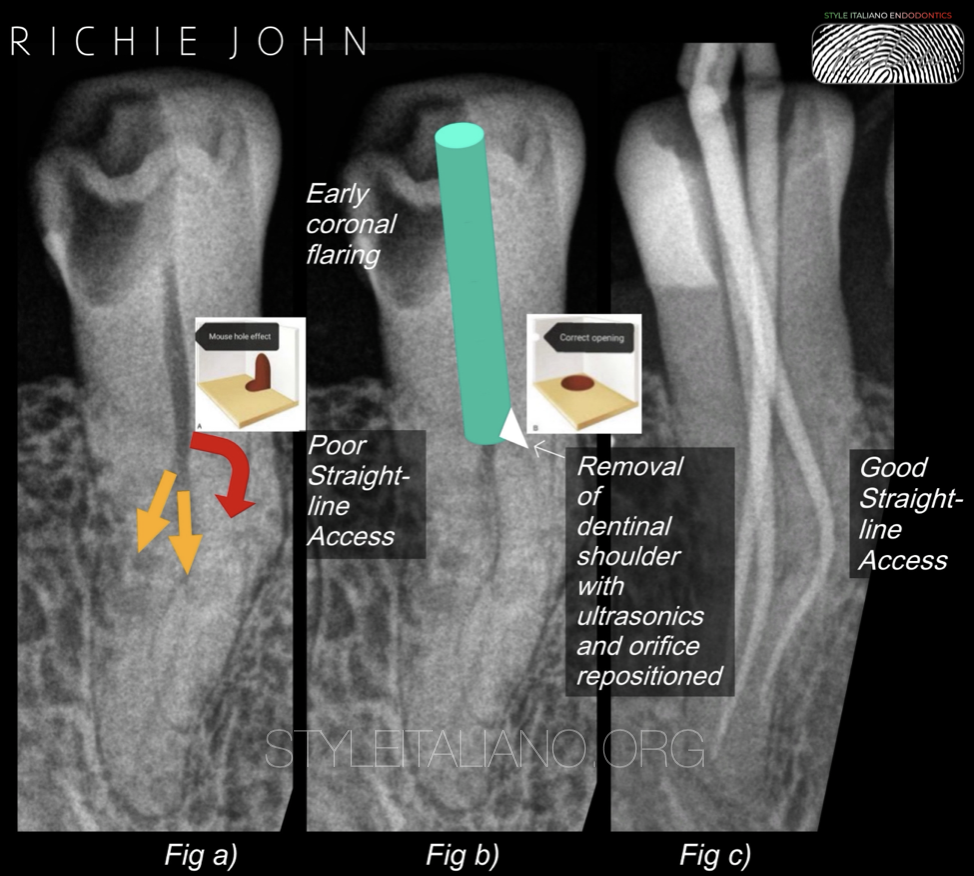
Fig. 2
Fig a) shows the third/distal canal marked as the arrow in red, with a very pronounced, acute angle of entry into the canal thereby significantly increasing the chances of this canal not being discovered during treatment whereas the buccal and lingual canals marked in yellow have a relatively straight-line access for negotiation and shaping.
Fig b) demonstrates an early coronal flaring using orifice openers or Gates Glidden drills sizes 1 to 3 till the level of trifurcation. The objective is to achieve a straight-line access to the third canal, if not, increasing the chances of rotary file separation. Irrigation is done with copious amounts of sodium hypochlorite, passive ultrasonication, saline rinse, stropko irrigator for drying and better visualization of the operating field. Utilizing diamond-coated ultrasonic tips, enables the operator to refine the access cavity and remove dentinal overhangs. These tips specifically facilitate repositioning of the canal orifice from the axial wall to the pulpal floor by removing the dentinal shoulder, thereby achieving our objective.
Fig c) elucidates the impression of a well shaped root canal system having a good straight line access with conform GP cones in place for radiographic confirmation, prior to obturation.
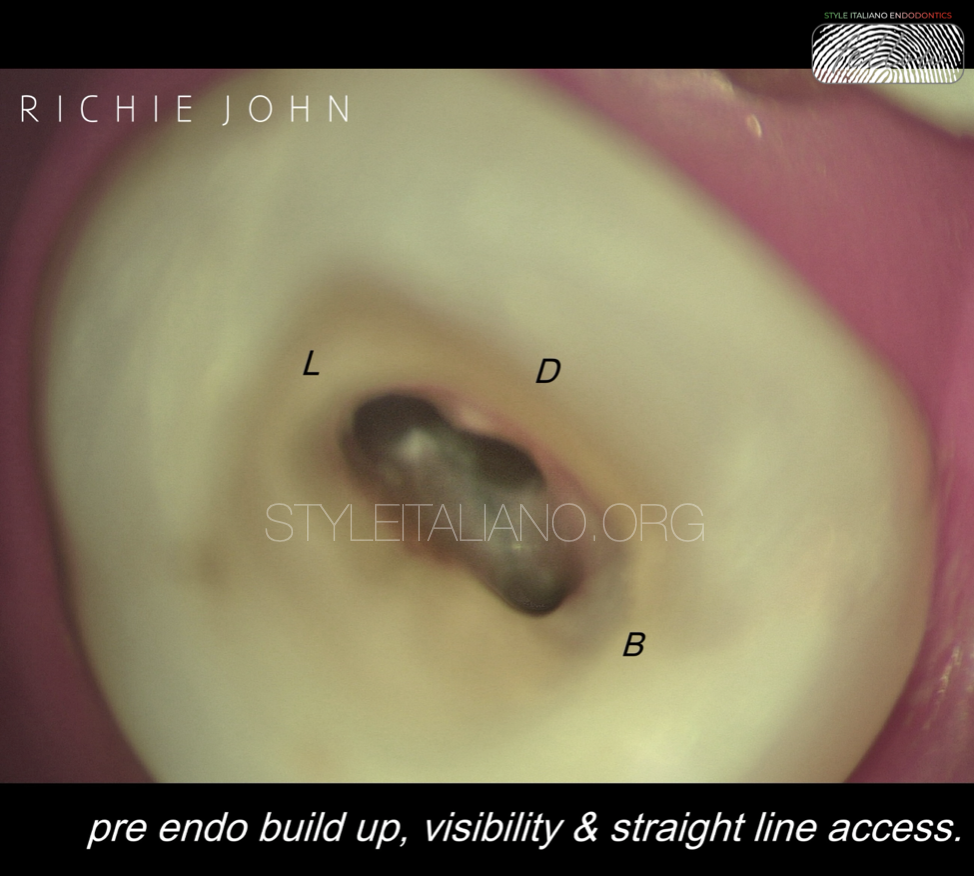
Fig. 3
Unimpeded visualization of all 3 canals can be appreciated in this intra-operative image taken under 8x magnification and coaxial illumination.
These canals were chemo mechanically prepared to a size 25.04 except the distal canal, which has been prepared to a size 20.04 due to its size, angle and radius of curvature and irrigation was done with a size 30.04 twin side vented, closed end flexible polypropylene needle.
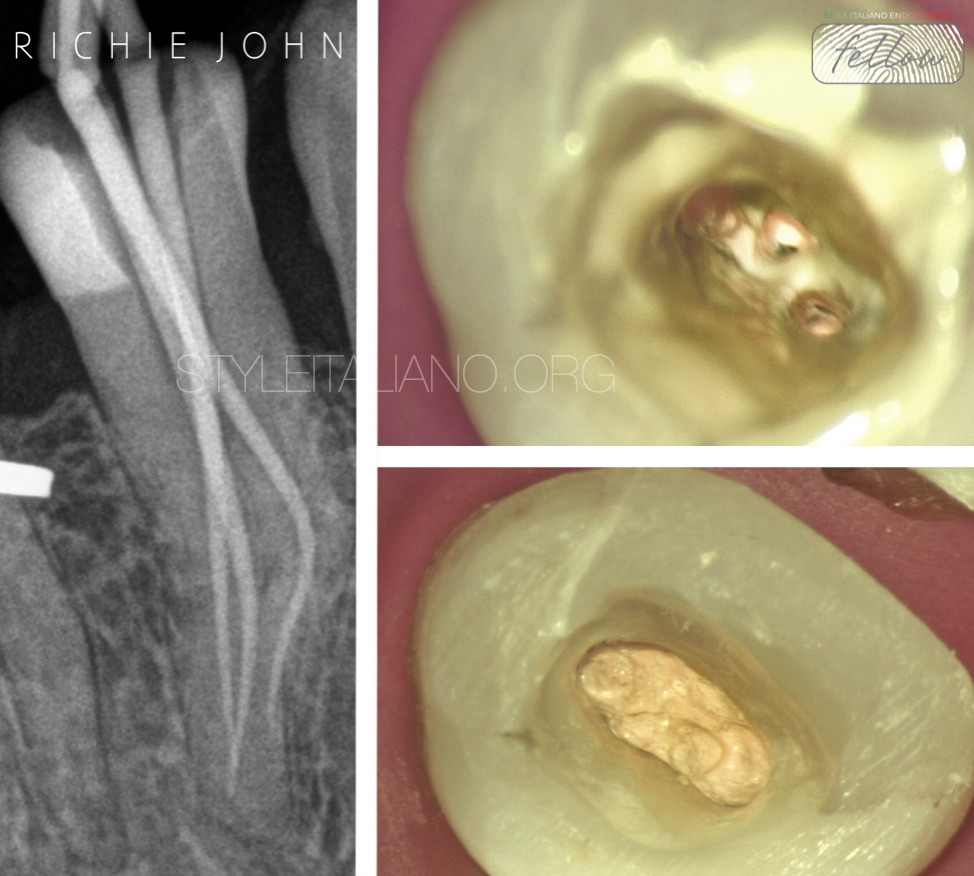
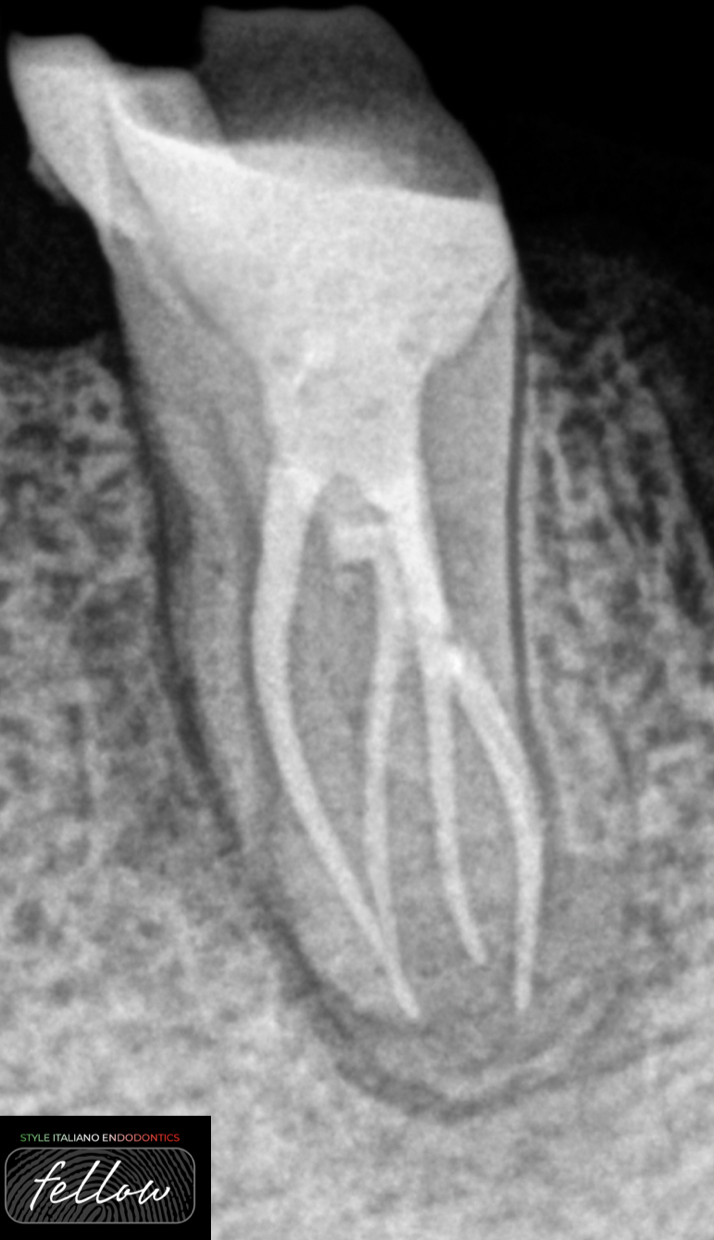
Fig. 4
Conform GP cones are placed and radiographically verified prior to obturation. Canals are now introduced with a sealer of choice and down-packed, backfilled.
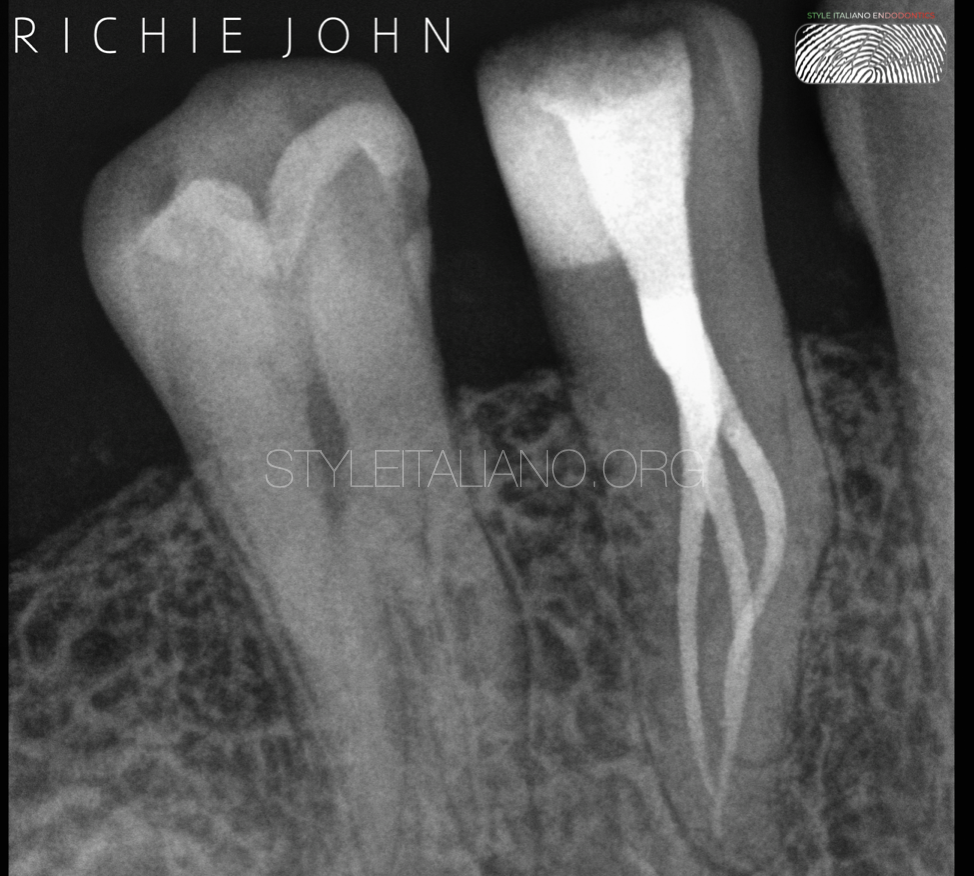
Fig. 5
Post operative radiograph showcasing a minimally invasive approach by preserving as much peri cervical dentine as possible and respecting the anatomy of the root canal system.

Fig. 6
About the author:
Richie John
Qualifications and Affiliations
• Bachelor of Dental Surgery (BDS): Vinayaka Missions University, India
• Master's Fellowship in Micro Endodontics (MFM): Saveetha University, India
• Key Opinion Leader: Imag Medical, Orodeka India
• Fellow: Style Italiano Endodontics Congress
Professional Overview
Experienced General Dentist with over a decade of practice with advanced training in Microscope Assisted Endodontics. Lectures across the nation and has a visiting practice based in Kerala, India.
Areas of Expertise
• Endodontic treatments with high difficulty index
• Complex anatomies and curvatures
• Surgical and non-surgical endodontic retreatment
Academic Contributions
• Delivered lectures on advanced endodontic techniques across various dental institutions and conferences globally.
• Conducted workshops on microscope-assisted endodontics, endodontic retreatment, and management of complex endodontic cases.
• Pubmed indexed case report articles.
Conclusions
Mandibular first premolars may present with such aberrant anatomy and clinicians must be prepared to encounter such anatomical variations and the success of nonsurgical endodontic treatment hinges on a comprehensive understanding of root canal anatomy, precise radiographic interpretation, and diligent clinical inspection. Additionally, careful modification of the access opening, augmented by adequate magnification and pre operative cbct is crucial for an optimal outcome.
Bibliography
1. Rotstein Ingle J I Ingle’s Ingle’s Endodontics7th Edn.PMPH USA2019
2. J I Ingle L K Bakland Ingle’s endodontics 55th Edn.Decker Inc2002
3.B M Cleghorn W H Christie C C S Dong The Root and Root Canal Morphology of the Human Mandibular First Premolar: A Literature ReviewJ Endod200733550916
4. Sashi Nallapati, Three Canal Mandibular First and Second Premolars: A Treatment Approach. A Case Report, Journal of Endodontics,
Volume 31, Issue 6, 2005, Pages 474-476, ISSN 0099-2399, https://doi.org/10.1097/01.don.0000157986.69173.a6.
5. Saravanan, Poorni & Karumaran, Chellasamy & Indira, Rajamani. (2010). Mandibular rst premolar with two roots and three canals. Australian endodontic journal : the journal of the Australian Society of Endodontology Inc. 36. 32-4. https://doi.org/10.1111/j.1747-4477.2009.00170.x.
6. Albuquerque, Denzil, Kottoor, Jojo, Hammo, Mohammad, Endodontic and Clinical Considerations in the Management of Variable Anatomy in Mandibular Premolars: A Literature Review, BioMed Research International, 2014, 512574, 11 pages, 2014. https://doi.org/10.1155/2014/512574
7. Van der Vyver, PJ, Vorster, M, & Jonker, CH. (2020). Mandibular first and second premolars with challenging root canal anatomy - Part 1: Review of the literature. South African Dental Journal , 75(3), 126-129. https://doi.org/10.17159/2519-0105/2020/v75no3a2