Optimizing Endodontic Outcomes through Selective Root Retreatment
04/02/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
In field of endodontic retreatment, the traditional dichotomy between non-selective nonsurgical methods and selective surgical interventions has been redefined by advances in CBCT imaging. This technological leap has facilitated the development of a contemporary method that amalgamates the conservative nature of nonsurgical techniques with the precision of surgical selectivity. This novel, minimally invasive approach allows for the targeted treatment of endodontic failures, providing a refined alternative to conventional practices.
A 42-year-old male presented with enduring discomfort in tooth #46, citing a history of endodontic treatment two years prior. Clinical examination revealed tenderness on percussion and mastication, though gingival tissues exhibited normal characteristics. Radiographic assessment showed apical periodontitis adjacent to a fiber post-reinforced distal root. Small field CBCT imaging of the lower right quadrant was conducted, unveiling an auxiliary disto-lingual canal, branching from the principal one in the mid-root region, associated with localized periapical pathology. Therapeutic options discussed included complete non-surgical retreatment, apical surgery, and conservative non-surgical intervention targeting the affected root only. The patient elected the least invasive option, non-surgical selective retreatment, addressing the identified pathology while preserving the remaining tooth structure.

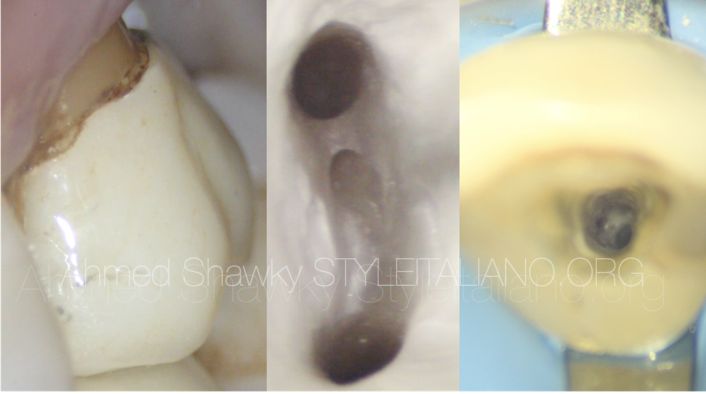
Fig. 1
Pre operative periapical radiograph:
Large composite restoration supported by a fiber post in the distal root.
Periapical pathology associated with the distal root.
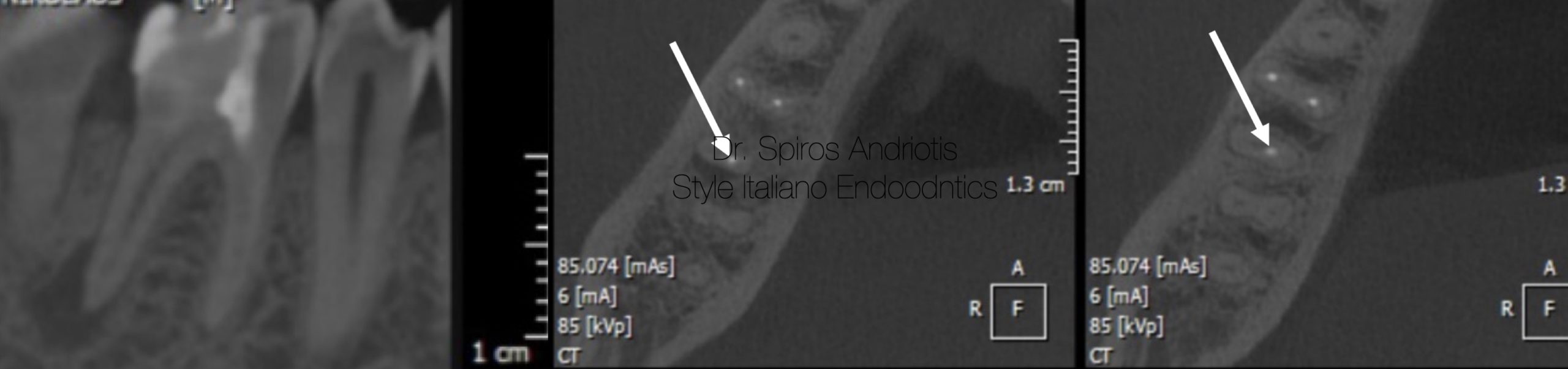
Fig. 2
CBCT reveiling the presence of a second lingual canal in the distal root and an isolated periapical pathology associated with the same root.

Fig. 3
The tooth was isolated with rubber dam while using a number #7 clasp. Liquid dam was placed as a supplementary insulation.
In our procedure to remove the fiber post, careful preparation with a Dentsply Endo Access bur FG2 allowed the ultrasonic tip for a clear access. A distal part of the composite restoration was removed as it it presented with secondary caries laying beneath. Using diamond coated ultrasonic tips we set our device to a low power to initiate gentle vibrations, systematically weakening the cement's hold on the post. Cooling was crucial; we intermittently applied water to dissipate heat, safeguarding the tooth's structure. Our attention to the tooth's response dictated short, deliberate intervals of work until gutta-percha material was visible.
The old obturation material was removed with a combination of a Gates Glidden number #1 bur and XP Endo Shaper.
The missed canal was identified and its working length was estimated using an apex locator. Shaping was done using the Reciproc sequence (vdw) up to the final 50/0.5 apical enlargement and taper respectfully. Irrigation was carried out using NaOCl 5% and activation with ultrasonic tips. EDTA 17% was injected in the canals for 3 minutes. Finally NaOCl 5% was injected for an extra 3 minutes. The canals were dried and a non setting calcium hydroxide based paste was placed and left in the canals for 20 days.
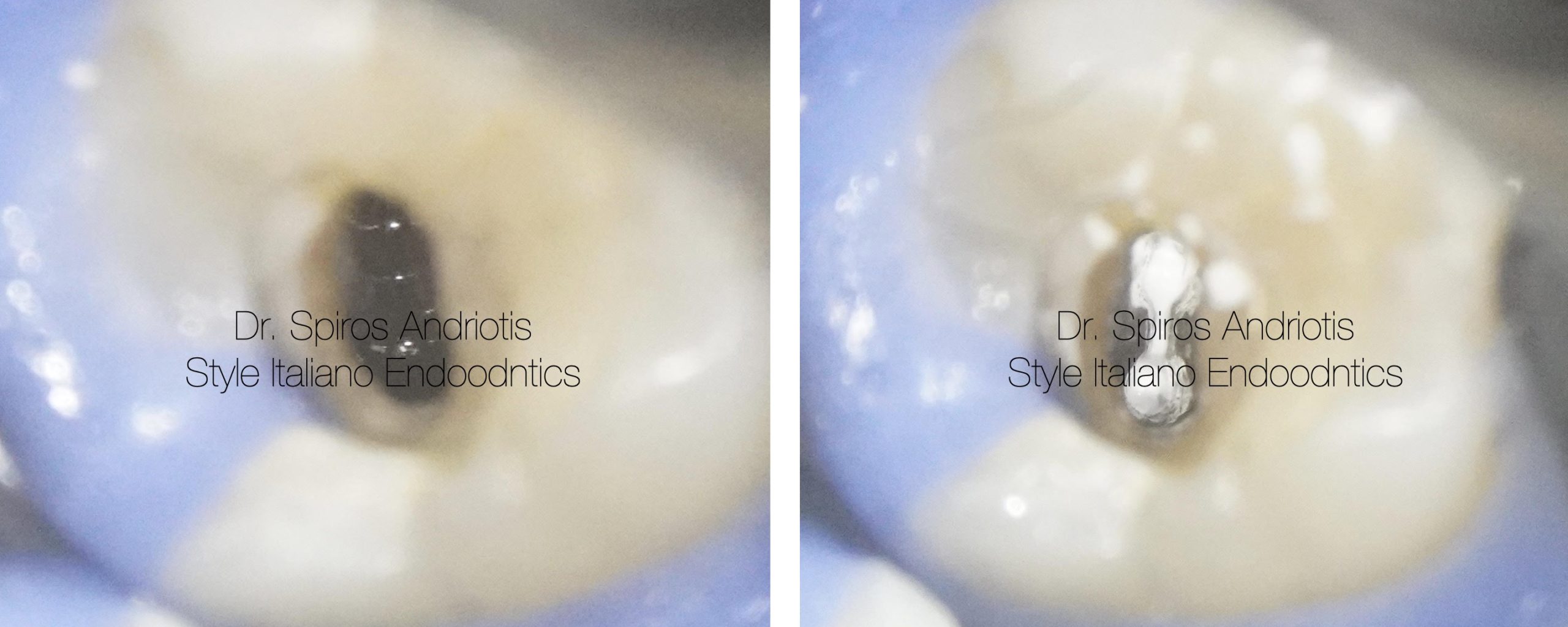
Fig. 4
During the second visit the patient reported that symptoms disappeared after 1 day.
The intermediate medication material was removed and the final irrigation protocol was applied:
NaOCl 5% (ultrasonic activation for 2 minutes)
EDTA 17% (3 minutes)
NaOCl 5% (3 minutes)
Saline rinse
The canals were dried with sterile paper points and obturated with a cold hydraulic condensation technique and bioceramic sealer.
The provisional restoration was completed, and the patient was referred back for prosthetic rehabilitation. Ongoing surveillance will be conducted, with a subsequent radiographic evaluation scheduled for six months post-treatment to assess the therapeutic results.

Fig. 5
Post operative radiograph with the final obturation of the distal canal, 20 days after the initial placement of non setting calcium hydroxide paste. Multiple portals of exit can be observed.

Fig. 6
Conclusions
Selective root retreatment emerges as a sophisticated approach, particularly when integrated with cone-beam computed tomography (CBCT). This technique diverges from traditional, broad-spectrum retreatment, focusing instead on individualized care for each root based on its unique periapical health status. By leveraging CBCT's unparalleled diagnostic capabilities, dentists are empowered to precisely identify and treat only the affected roots, thus preserving the integrity of unaffected areas. This precision-driven approach not only embodies the essence of minimally invasive endodontics but also significantly elevates the standard of patient care through targeted, efficient treatment modalities.
Bibliography
- Selective Root Retreatment: A Novel Approach William J. Nudera, DDS, MS Published: April 21, 2015 (VOLUME 41, ISSUE 8) Journal of Endodontics
- Outcome of selective root canal retreatment-A retrospective study João Filipe Brochado Martins, Olavo Guerreiro Viegas, Roberto Cristescu , Patrícia Diogo , Hagay Shemesh Published: 2022 Nov 27. National Library of Medicine