Nonsurgical Repair of a Deep Root Perforation with MTA: Evaluation of Periradicular Healing at 1 Year
28/05/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Root perforations represent an unfortunate and challenging complication in endodontic therapy, often resulting from iatrogenic deviation during access cavity preparation, post-space formulation, or canal negotiation. A perforation creates an artificial communication between the root canal system and the surrounding periodontal tissues. If left unsealed, bacterial microleakage promptly ensues, leading to chronic inflammation of the periodontal ligament, localized bone destruction, and ultimately, a compromised long-term prognosis for the tooth.
Historically, repairing deep root perforations was surgically demanding and often yielded unpredictable outcomes due to the lack of biocompatible sealing materials. The introduction of Mineral Trioxide Aggregate (MTA) revolutionized the management of these defects. MTA is highly regarded as the gold standard for perforation repairs owing to its exceptional biocompatibility, structural sealing capabilities even in a moist environment, and its ability to actively induce cementogenesis and osteogenesis. Prompt intervention using MTA can effectively wall off the defect, arrest inflammatory bone resorption, and stimulate periradicular regeneration.
This case report documents the successful nonsurgical management of a mandibular premolar that sustained a deep root perforation during the clinical build-up and negotiation phase. Utilizing a biocompatible MTA plug to seal the defect, remarkable periradicular bone healing and clinical stability were achieved at the 1-year follow-up.
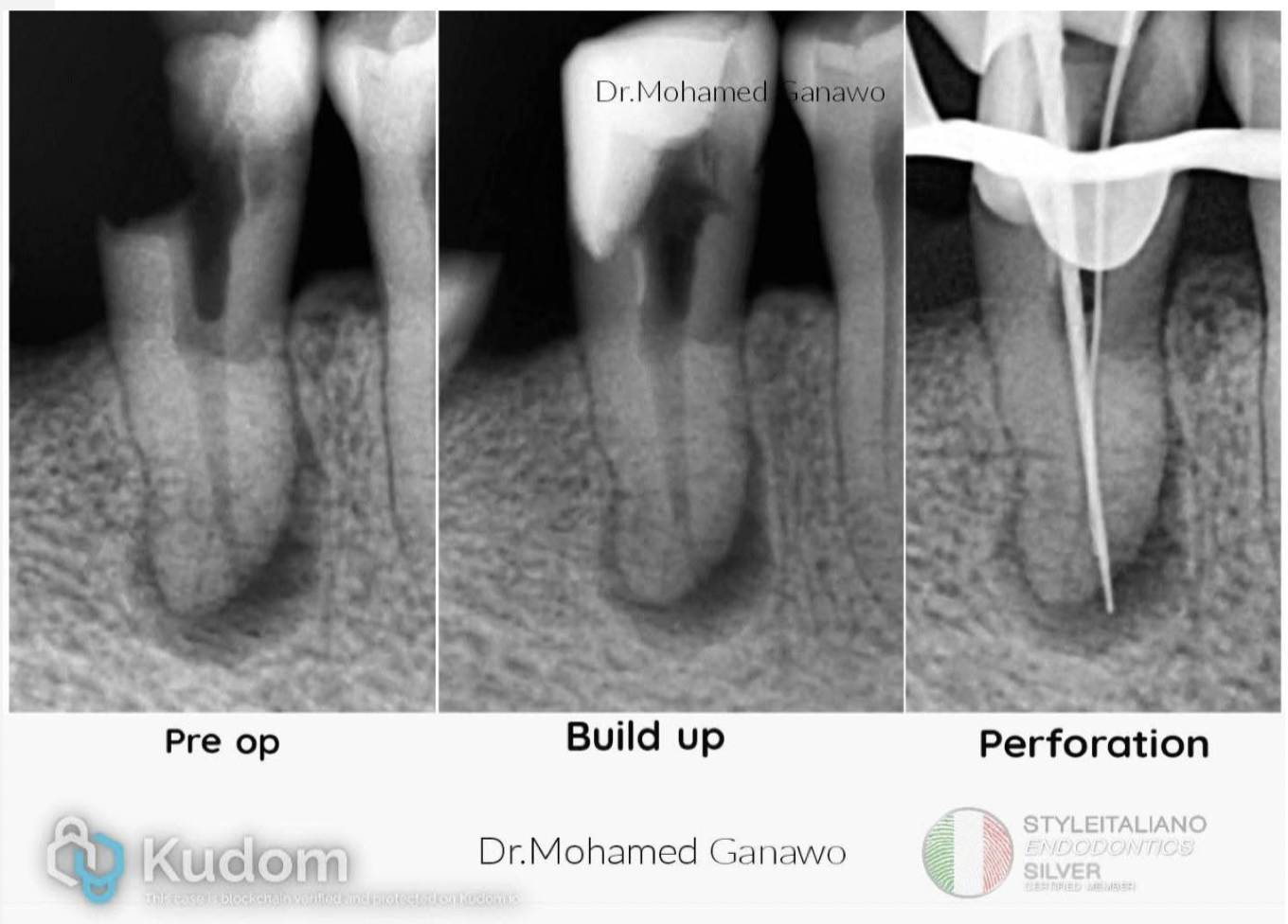
Fig. 1
Pre-op: Shows a mandibular premolar with extensive coronal loss, a wide/compromised pulp chamber, and a significant periapical/periradicular radiolucency indicating chronic inflammatory bone resorption.
Build up: Represents the pre-endodontic coronal restoration phase, where a temporary or structural wall was built up to facilitate isolation and contain irrigants.
Perforation: Highlights the clinical complication where a scouting instrument or file deviated from the main canal path, exiting through the lateral/apical wall of the root and creating an iatrogenic perforation directly into the periradicular lesion.
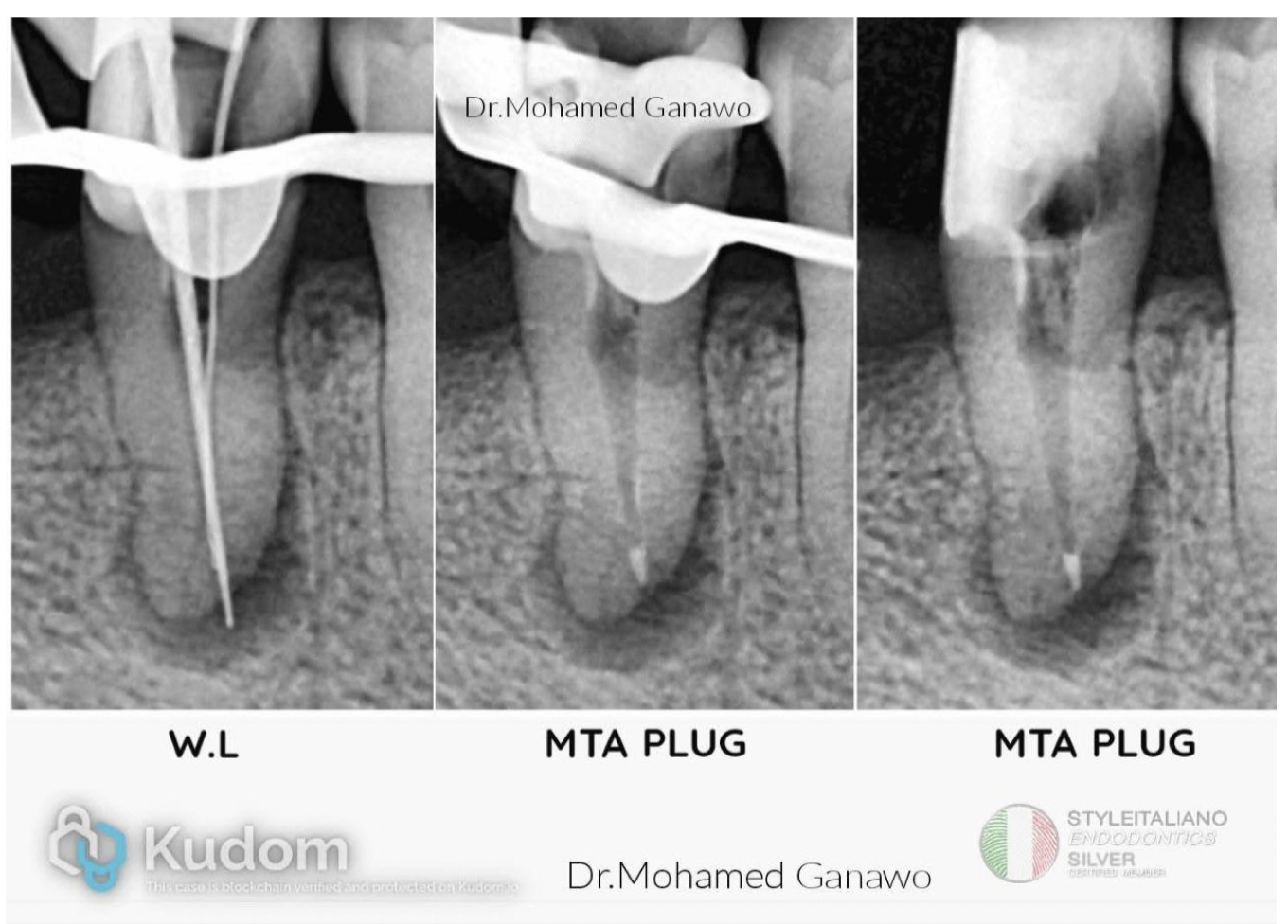
Fig. 2
W.L (Working Length): Shows the initial negotiation of the perforation site under rubber dam isolation. The scouting instrument passes through the artificial lateral path to establish the operational depth directly at the site of the defect.
MTA PLUG : Documents the precise delivery and adaptation of the Mineral Trioxide Aggregate (MTA) into the perforation site under isolated conditions, creating an immediate, dense, biocompatible seal.
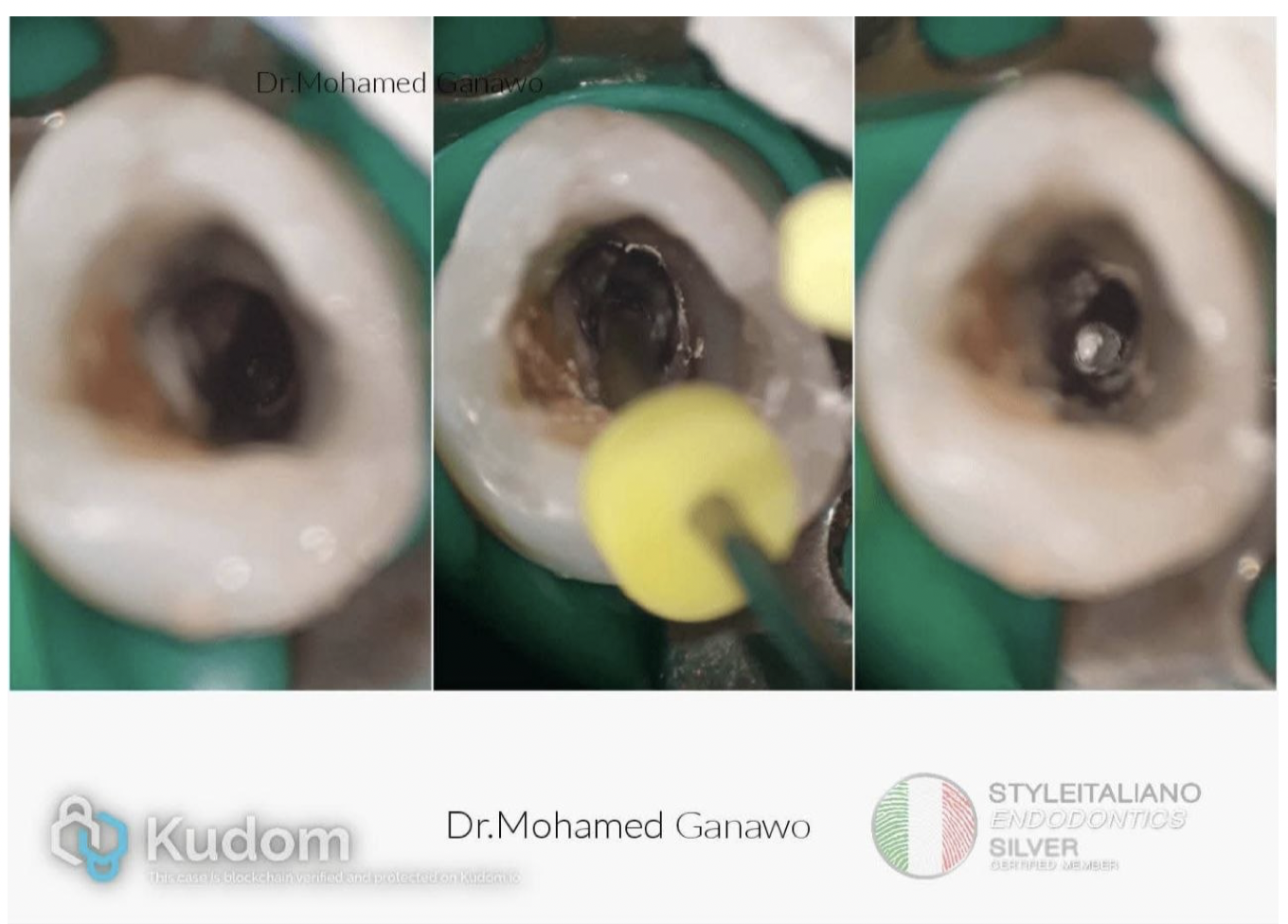
Fig. 3
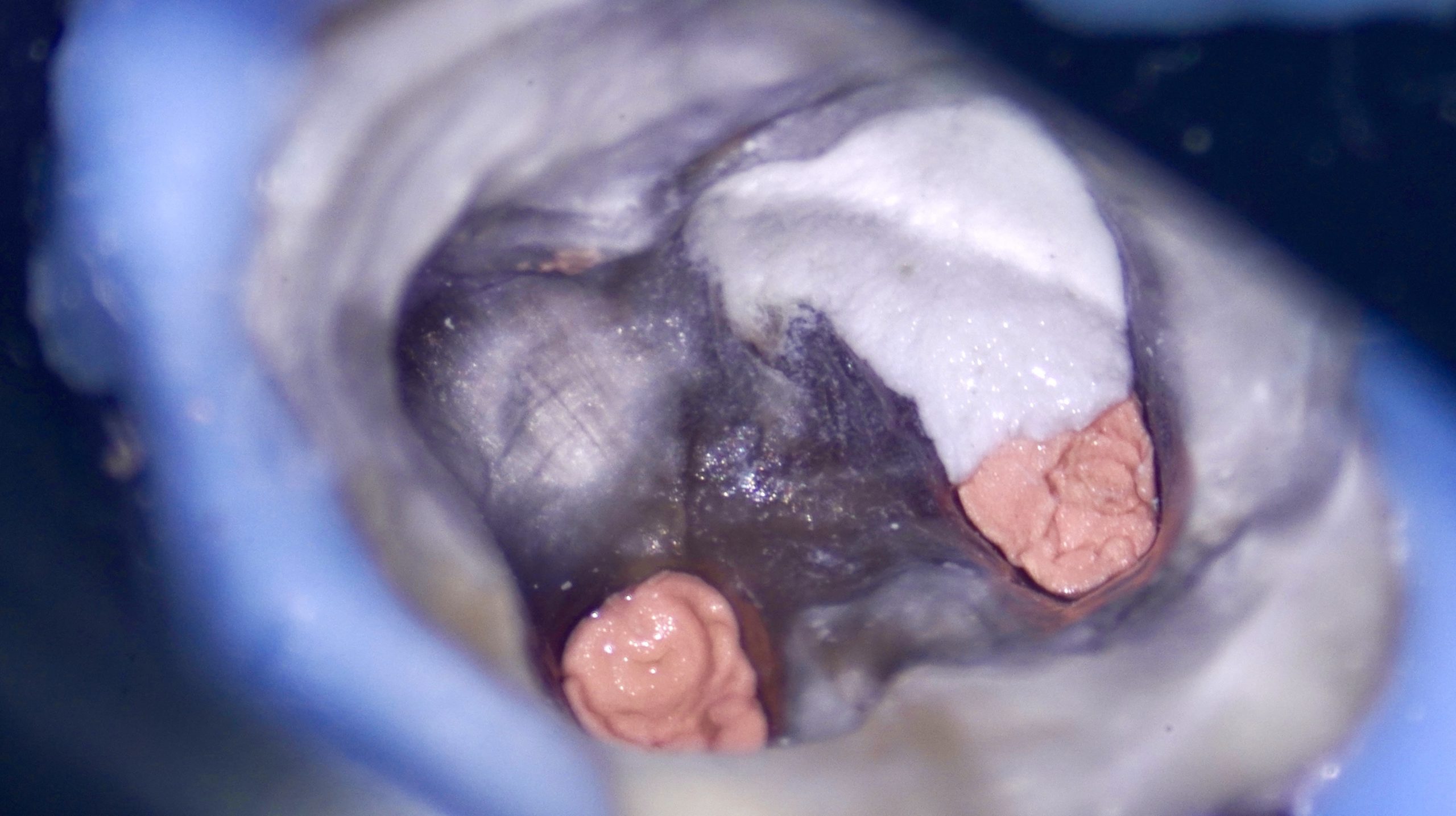
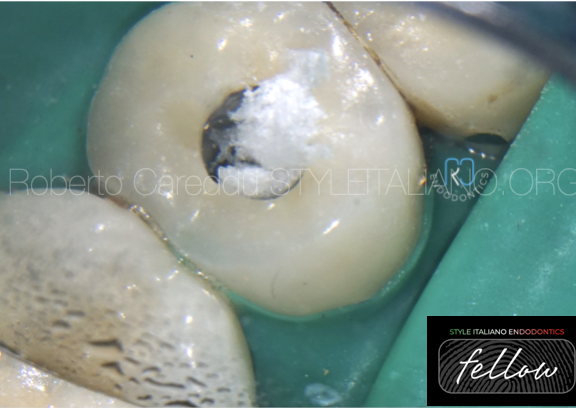
Left Image : Shows the internal view of the access cavity under rubber dam isolation after coronal build-up. The deep root perforation defect is visible at the floor/lateral wall of the canal space, presenting a direct communication with the periradicular tissues.
Middle Image : Documents the precise introduction and compacting of the MTA into the defect using a specialized endodontic carrier or plugger under high magnification.
Right Image (The Seal): Shows the final, dense white MTA plug cleanly adapted and sealed over the perforation site, isolating the internal root canal system from the surrounding periodontium before final obturation..
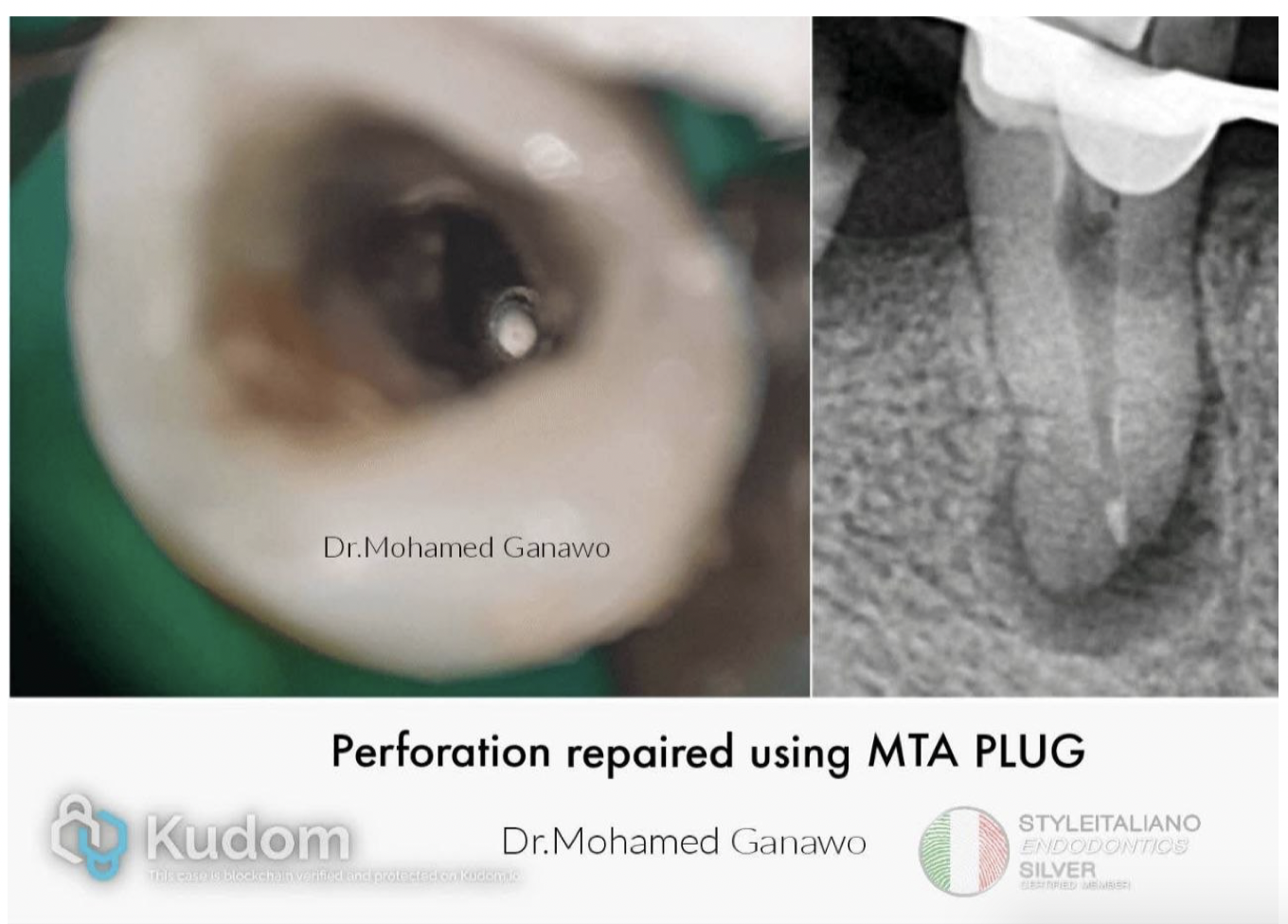
Fig. 4
Left Image (Clinical View): An intraoral, high-magnification microscopic view looking down into the access cavity. It shows the bright white, dense MTA plug completely sealing off the lateral perforation defect, restoring the structural integrity of the root wall before the true canal path is obturated.
Right Image (Radiographic View): The corresponding periapical radiograph confirming the exact position of the radiopaque MTA plug. It demonstrates a precise, three-dimensional adaptation of the material against the lateral/apical boundary of the defect, safely isolating the periradicular tissues from the main root canal system.

Fig. 5
W.L : Shows the initial negotiation and working length determination of the actual, main root canal system. Notice the already placed, radiopaque MTA plug sitting laterally/apically right next to the file, safely sealing off the previous perforation defect.
W.L (Middle Image) : A second working length confirmation view from a slightly different angulation (shift) to verify that the instrument is entirely within the true anatomic canal space and safely bypassing the repaired defect.
Cone fit : Documents the trial fitting of the primary gutta-percha cone to the full working length of the main canal, confirming proper apical seating and preparation before final warm vertical or lateral obturation.

Fig. 6
Cone fit (First Three Images): These show multiple angles of the master gutta-percha cone fitted to the full working length of the true canal system. Taking these angled views ensures the cone successfully bypasses the repaired perforation defect and reaches the true anatomic apex without displacing the adjacent MTA plug.
Post op (Right Image): Documents the final, completed endodontic treatment. The true root canal has been completely obturated, the iatrogenic perforation is successfully sealed with the dense MTA mass, and a stable coronal build-up/restoration has been placed, completely sealing the tooth from oral
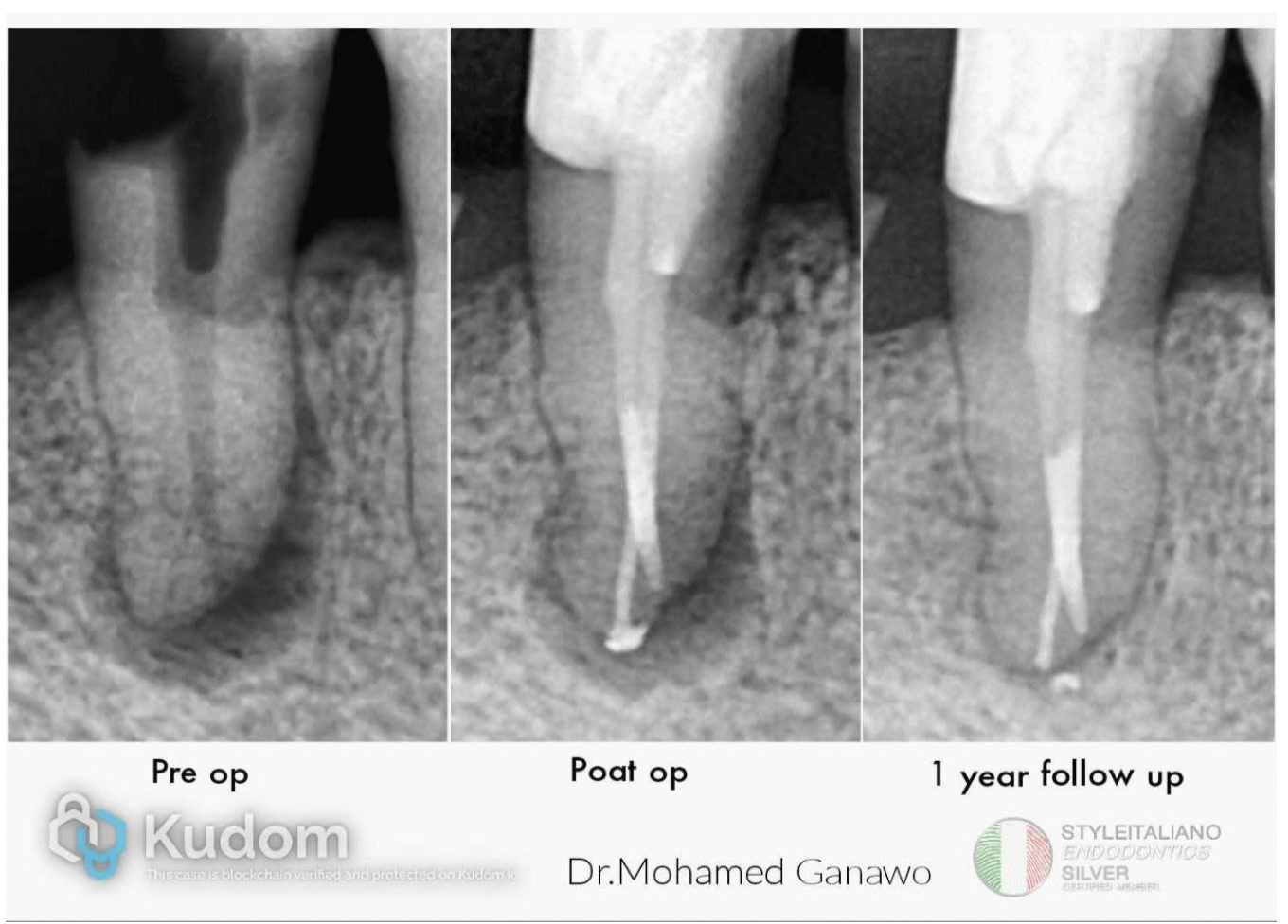
Fig. 7
1-Year Follow-up: The final image shows remarkable healing of the periapical radiolucency and stability of the MTA repair, indicating a successful biological response.
Conclusions
Accidental root perforations represent a severe threat to tooth retention, but their occurrence no longer dictates extraction. As demonstrated in this case, the successful management of an iatrogenic perforation depends heavily on immediate diagnosis, infection control, and the application of a biocompatible sealing material.
The use of MTA to repair the perforation defect provided an immediate, fluid-tight seal against the periodontal tissues. The 1-year clinical and radiographic follow-up clearly illustrates the resolution of the surrounding radiolucency and the regeneration of the periradicular bone structure. This case reinforces that MTA perforation repair is a highly predictable and reliable nonsurgical intervention that can successfully salvage severely compromised teeth and restore long-term function.
Bibliography
1.Main, C., Mirzayan, N., Shabahang, S., & Torabinejad, M. (2004). Repair of root perforations using mineral trioxide aggregate: a long-term study. Journal of Endodontics, 30(2), 80-83.
2.Mente, J., Leo, M., Panagidis, D., Saure, D., & Pfefferle, T. (2014). Treatment outcome of root perforation repair with mineral trioxide aggregate: a prospective cohort study. Journal of Endodontics, 40(9), 1360-1366.
3.Siew, S., & Pitt Ford, T. R. (2005). Evaluation of MTA as a perforation repair material. International Endodontic Journal, 38(4), 220-226.
3.Clauder, T., & Shin, S. J. (2006). Repair of perforations with mineral trioxide aggregate: report of four cases. Dental Traumatology, 22(4), 217-224.