Non surgical management of full-crown restored with symptomatic apical periodontitis: A case report
02/09/2020
Alexandru Gliga
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The reason for performing a primary root canal treatment or a retreatment without dismantling a full crown coverage should be very well considered. It is doubtless that any coronal restoration should be removed before undertaking any orthograde endodontic procedure if infected dentine or coronal leakage is present (Gulabivala, Ng, 2014). Moreover, performing a root canal treatment and an endodontic access under these conditions should offer the clinician the certainty that the remaining tooth structure under the preserved restoration is sound.
Assuming that the upper mentioned aspect is under control, any root canal therapy carried out through a crown or a bridge constrains the clinician to inform the patient that the prosthetic restoration can be substantially affected and damaged and might require complete replacement after the endodontic procedure. Furthermore, the clinician should advise the patient that some details can only be evaluated intraoperative, thus the will of preserving any restoration can turn out to be unsustainable at any time.
The management of iatrogenic errors in situations like the one described is challenging and might bring unfavourable circumstances for the clinician, however undertaking endodontic procedures through restorations provoke the skills of any endodontist.
For preserving full crown restorations when performing endodontic treatments one should have in mind many aspects including the marginal adaptation, the dentine quality under the restoration, the remaining tooth structure after the infected dentine removal, the time when the restoration was placed, the age of the patient, the costs and implications for the restoration removal, the position of the restored tooth/teeth.
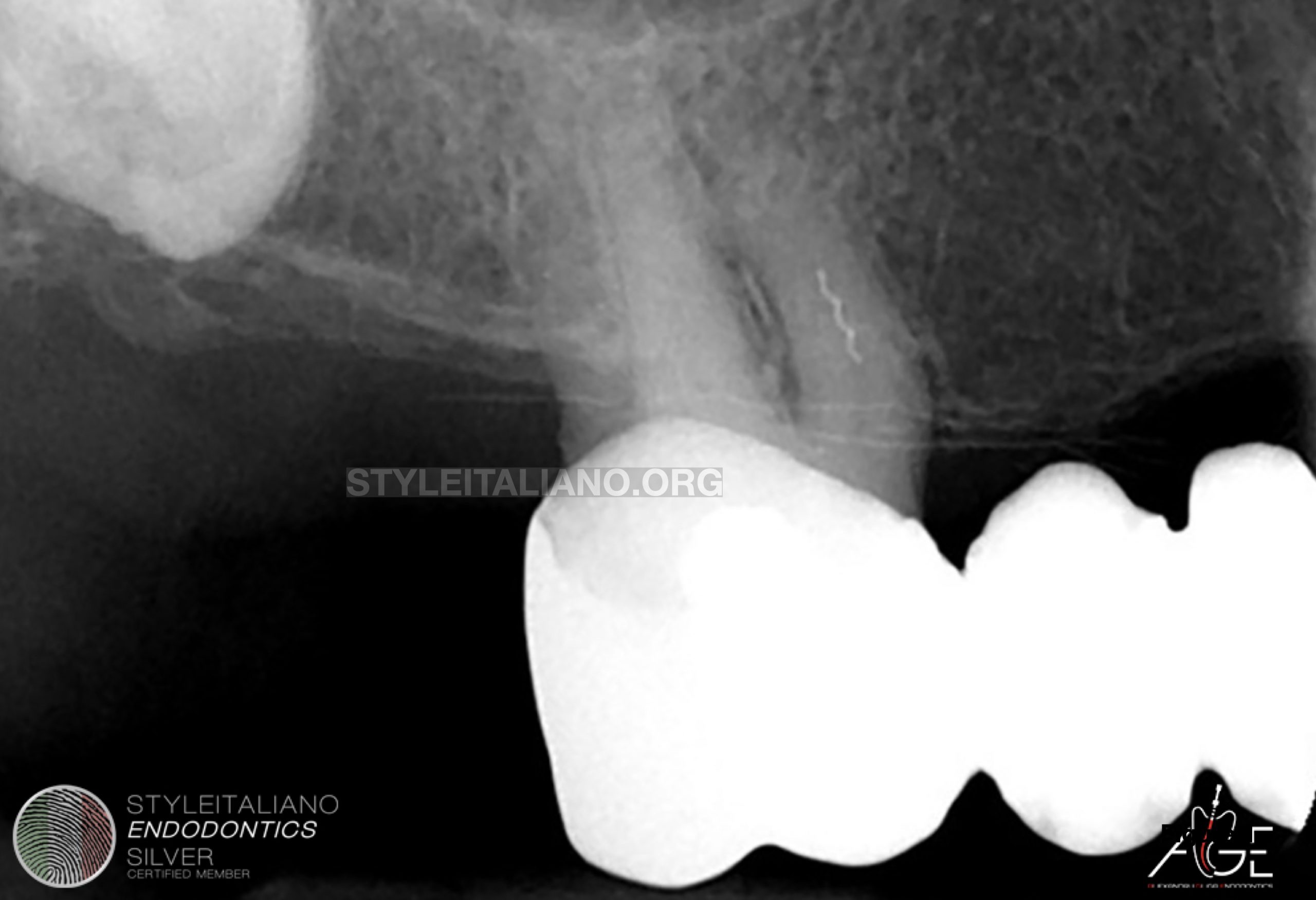
Fig. 1
The reason for performing a primary root canal treatment or a retreatment without dismantling a full crown coverage should be very well considered. It is doubtless that any coronal restoration should be removed before undertaking any orthograde endodontic procedure if infected dentine or coronal leakage is present (Gulabivala, Ng, 2014). Moreover, performing a root canal treatment and an endodontic access under these conditions should offer the clinician the certainty that the remaining tooth structure under the preserved restoration is sound.
Assuming that the upper mentioned aspect is under control, any root canal therapy carried out through a crown or a bridge constrains the clinician to inform the patient that the prosthetic restoration can be substantially affected and damaged and might require complete replacement after the endodontic procedure. Furthermore, the clinician should advise the patient that some details can only be evaluated intraoperative, thus the will of preserving any restoration can turn out to be unsustainable at any time.
The management of iatrogenic errors in situations like the one described is challenging and might bring unfavourable circumstances for the clinician, however undertaking endodontic procedures through restorations provoke the skills of any endodontist.
For preserving full crown restorations when performing endodontic treatments one should have in mind many aspects including the marginal adaptation, the dentine quality under the restoration, the remaining tooth structure after the infected dentine removal, the time when the restoration was placed, the age of the patient, the costs and implications for the restoration removal, the position of the restored tooth/teeth.
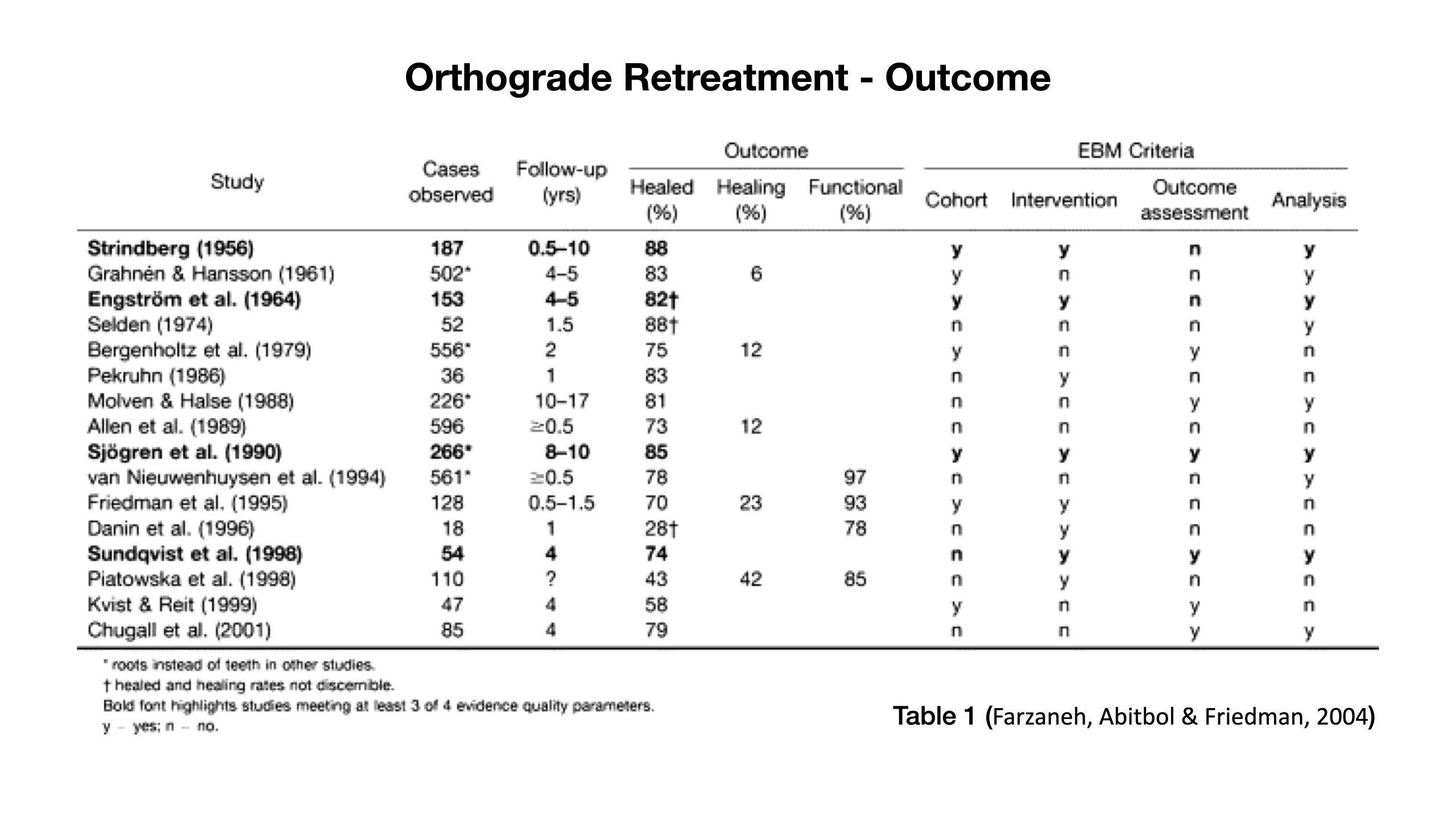
Fig. 2
Table 1 (Farzaneh, Abitbol & Friedman, 2004)

Fig. 3
The 76 years old patient was referred by her general dental practitioner for endodontic evaluation and retreatment. She complained about biting tenderness associated with tooth 16 that persisted for the last 2 months.
The patient hoped for keeping the restoration if there was any chance for she was not determined to change anything at her age but to manage her discomfort and regain functionality.
Considering the presented situation, the decision was to try to conserve the bridge, completing the root canal retreatment through the crown restoration.
The access was performed, the infected dentine has been completely removed, the separated file was retrieved using U-file (Mani) and a fiber post was placed inside the palatal canal and the tooth was coronally sealed with composite.

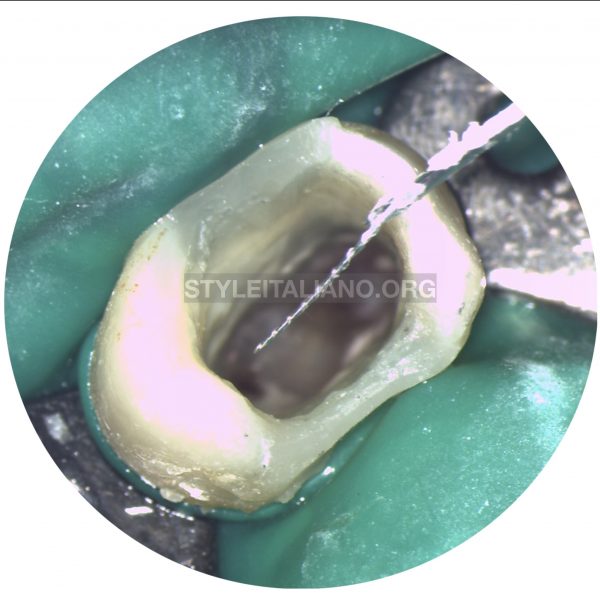
Fig. 4
Detail of the access
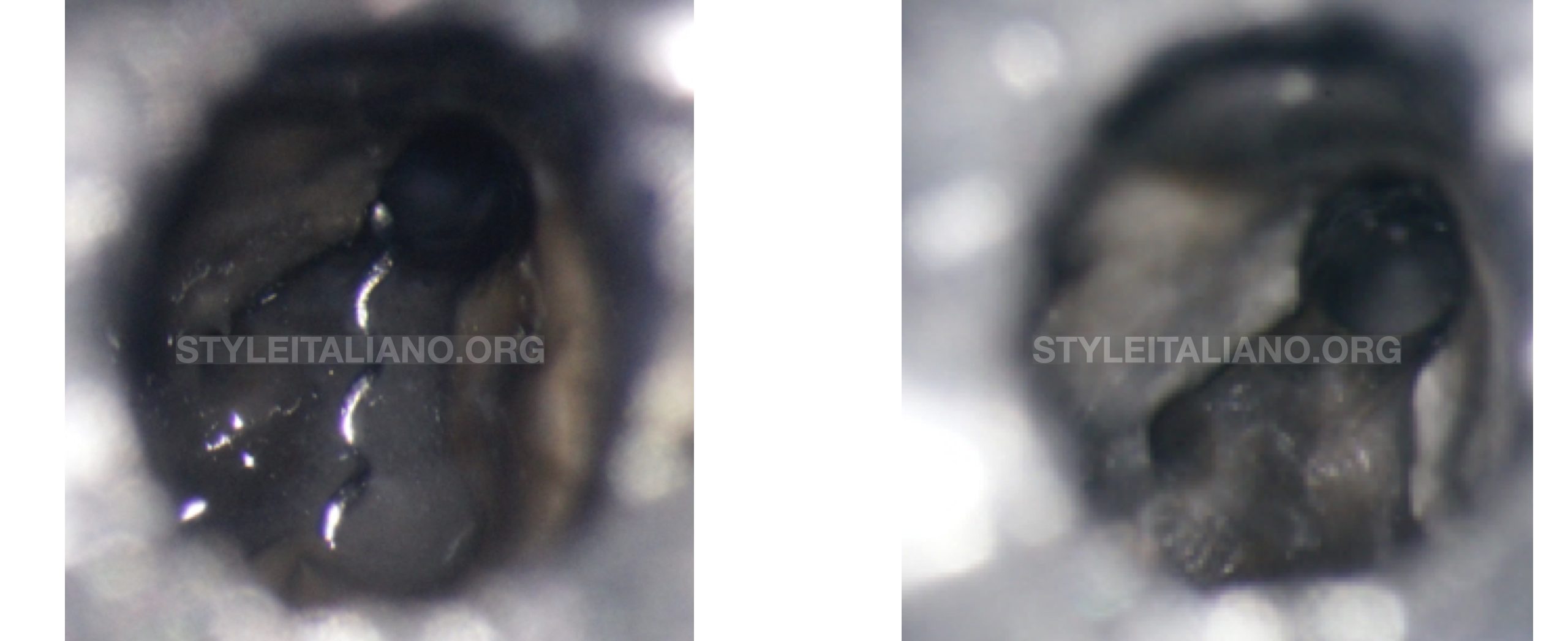
Fig. 5
Separated lentulo was removed from inside the MB1 canal.
The canals were negotiated in reciproc technique with m-wire used also for the final preparation of the DB and MB1 canal.
For the final shaping of the palatal canal #40 rotary was used.

Fig. 6
Detail of the separated Lentulo
Fig. 7
Vertical warm condensation technique was performed to obturate the canals.

Fig. 8
The fiber post was placed inside the palatal canal and the tooth was sealed with composite.
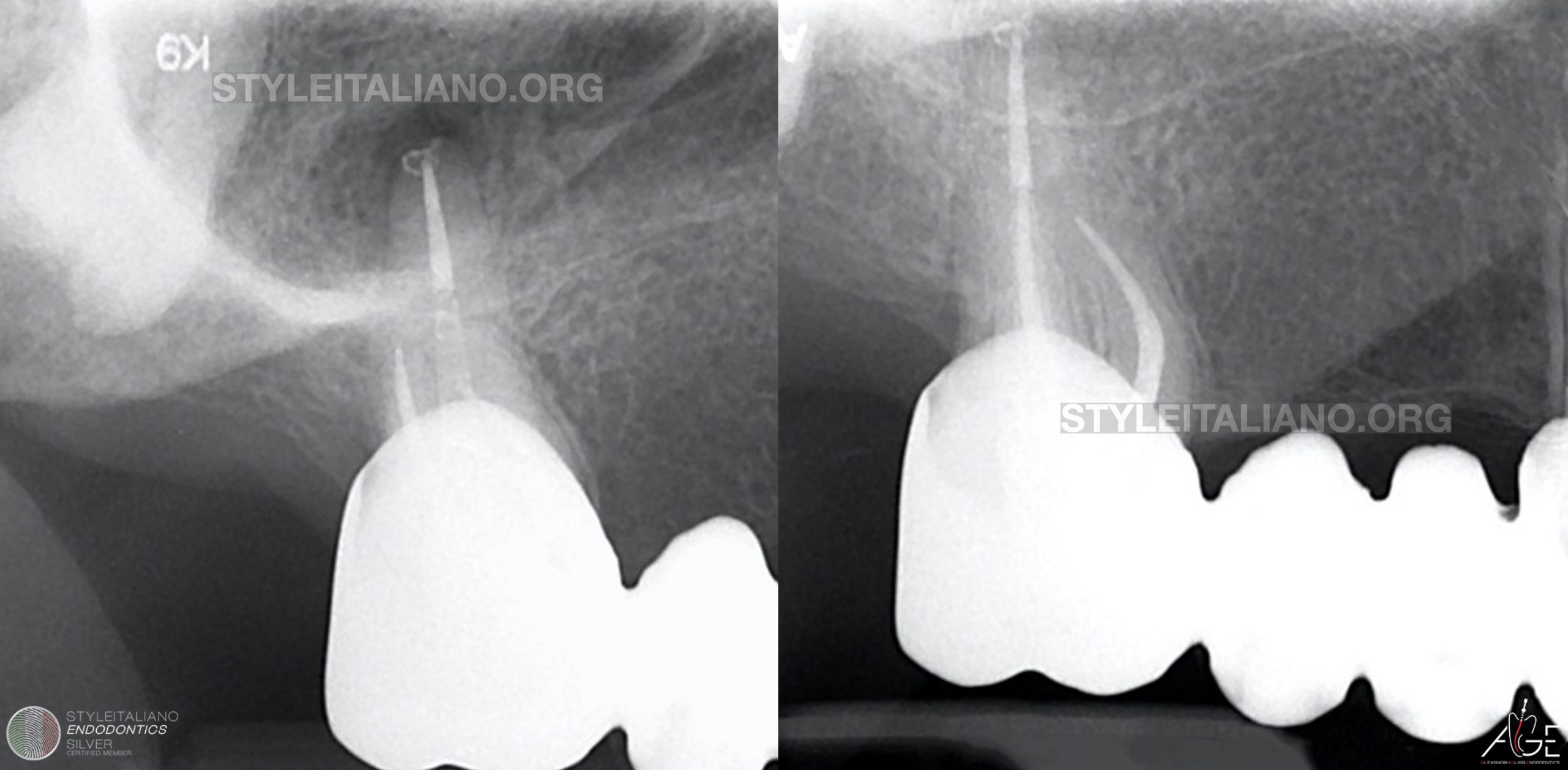
Fig. 9
Post operative Xrays
Conclusions
Altogether, a correct assessment followed by a sustainable approach and coherent intraoperative decision can give on to a successful and less invasive treatment. Conserving old restorations or even dentine might sometimes bring challenges and complications for clinicians, hence this approach has to be logic, useful and motivated with less heroic and egocentric reasoning.
Even though retrograde endodontic treatment is very common in situations like the one described, the outcome of orthograde endodontic therapy represents a major decision factor for the first clinician choice.
Bibliography
Farzaneh, M., Abitbol, S. & Friedman, S. 2004, Treatment Outcome in Endodontics: The Toronto Study. Phases I and II: Orthograde Retreatment.
Gulabivala, K. & Ng, Y. 2014, Endodontics, Mosby, London.