
Navigate the curve: the Rising protocol
15/04/2025
Mohamad Zaafrany
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Shaping narrow and curved canals remains one of the most complex challenges in endodontics, particularly when dealing with coronal and multiplanar curvatures.
These anatomical variations increase the risk of procedural errors such as ledging, transportation, or even file separation.
Effective canal preparation in such scenarios demands well planned treatment approach and instruments that combine flexibility, strength, and safety.
In this case, we explore the management of a particularly difficult root canal system using the new RISING rotary system by Fanta Dental. Thanks to its innovative variable cross-section design, safe non-cutting tip, and advanced variable heat treatment.

Fig. 1
Preoperative radiograph
preoperative diagnostic imaging of the referred case of maxillary molar. The periapical radiograph and corresponding CBCT section clearly reveal the presence of deep distal caries as the primary reason for endodontic intervention. Notably, the imaging also highlights the complex canal anatomy, characterized by narrow and significantly curved root canals specially evident in the distal root.

Fig. 2
Illustrative drawing shows the multiplanar curvature of the distal root canal

Fig. 3
Preflaring is a critical initial step in preparation of such canals, as it allows for the removal of coronal interferences and dentin triangles that can obstruct access to middle and apical third. By creating a smooth, tapered coronal preparation early on, that would reduce stress on shaping instruments and minimizes the risk of procedural errors such as ledging or transportation.
Preflaring done using RR file of size 17/10 in brushing motion to remove the marked yellow parts/

Fig. 4
Clinical photo after preendodontic build up to mesial and distal walls and enhanced accessibility to the canals after preflaring using RR.
Trials done to locate MB2 but it was just a short isthmus however it was not evident in the CBCT but there was some sort of clinical representation

Fig. 5
Following coronal preflaring, a manual glide path was established using a size 10 K-file in a watch-winding motion to ensure safe negotiation of the canal anatomy. This was followed by the use of the RISING system's 13/03 file as a mechanical glide path, which smoothly followed the path to the apex with minimal resistance. In the distal canal, apical preparation was safely completed at size 25/04, avoiding unnecessary enlargement to reduce the risk of procedural errors in the narrow, curved anatomy.
For the mesiobuccal (MB) canal, enlargement was done to size 30/04.
The system’s transitional 28/05 file can be a valuable intermediate step before final shaping with the 30/04 file, specially in cases with multiplanar curves. It also aids in the smoother placement of the gutta-percha master cone if needed.
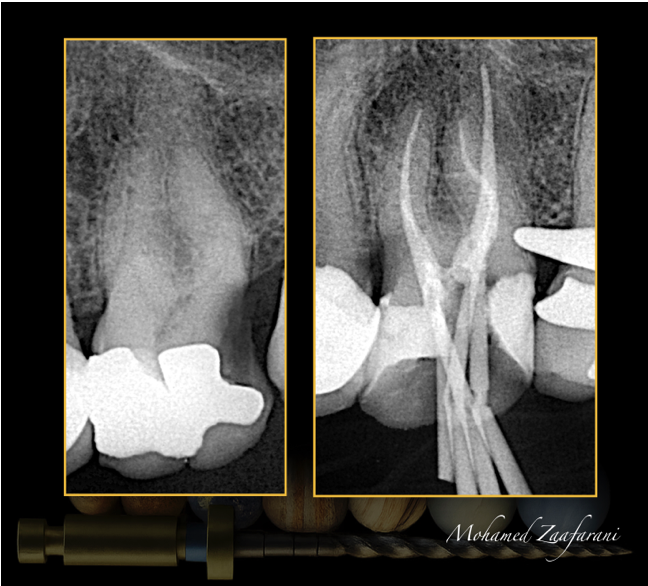
Fig. 6
Master cone fit radiographic image that shows proper shaping of the canals.
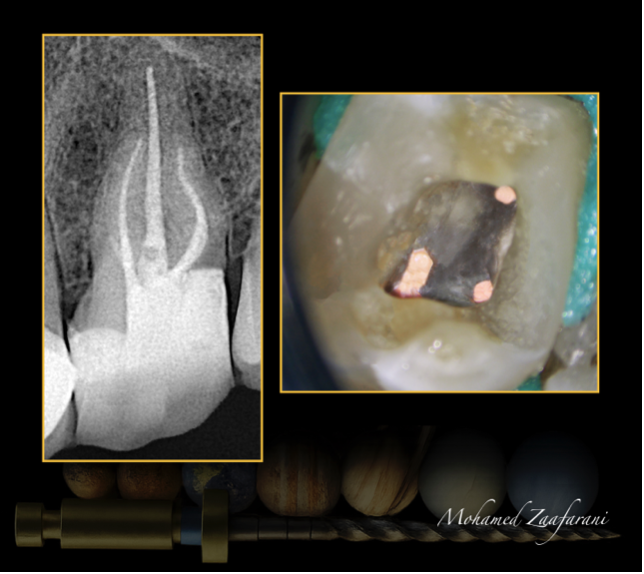
Fig. 7
Irrigation & Activation
-Sodium hypochlorite (5.25%) between each file.
-Sodium hypochlorite (5.25%) and EDTA 17% for Final flush with along with Sonic and ultrasonic activation to enhance irrigation penetration.
Obturation
•Technique: Modified heat technique with gutta percha and Bioceramic sealer.
Final radiographic image and clinical photo.
Conclusions
In conclusion, the RISING rotary system demonstrated excellent clinical performance in negotiating and shaping anatomically complex canals, including those with early coronal and multiplanar curvatures.
Its variable cross-sectional design, enhanced flexibility through variable heat treatment, and non-cutting tip collectively contributed to maintaining canal morphology while minimizing iatrogenic risks. This case demonstrate the critical role of strategic preflaring, glide path establishment, and instrument sequencing in achieving biologically respectful and mechanically sound canal shaping.
Bibliography
Scarfe WC, Levin MD, Gane D, Farman AG. Use of cone beam computed tomography in endodontics. Int J Dent. 2009;2009:634567. doi: 10.1155/2009/634567. Epub 2010 Mar 31. PMID: 20379362; PMCID: PMC2850139.
Krasner P, Rankow HJ. Anatomy of the pulp chamber floor. JOE 2004; 30(1):5.
The endodontic Glidepath: "Secret to rotary safety”. John D West Dent Today 2010 Sep;29(9):86, 88, 90-3.
Shen Y, Qian W, Abtin H, Gao Y, Haapasalo M (2011) Fatigue testing of controlled memory wire nickel-titanium rotary instruments J Endod 2011 Jul;37(7):997-1001. doi: 10.1016/j.joen.2011.03.023.
Manual versus mechanical endodontic glide path. John D West Dent Today 2011 Jan;30(1):136, 138, 140
Influence of Negotiation, Glide Path, and Preflaring Procedures on Root Canal Shaping—Terminology, Basic Concepts, and a Systematic Review. February 2020 Journal of Endodontics DOI:10.1016/j.joen.2020.01.023



