Minimal Invasive Endodontics a “MUST” today
10/08/2023
José Aranguren
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Shaping procedure change so much in the last years, minimal invasive endodontics is a MUST in dentistry today, new materials lead us to work fast, secure and minimal invasive.

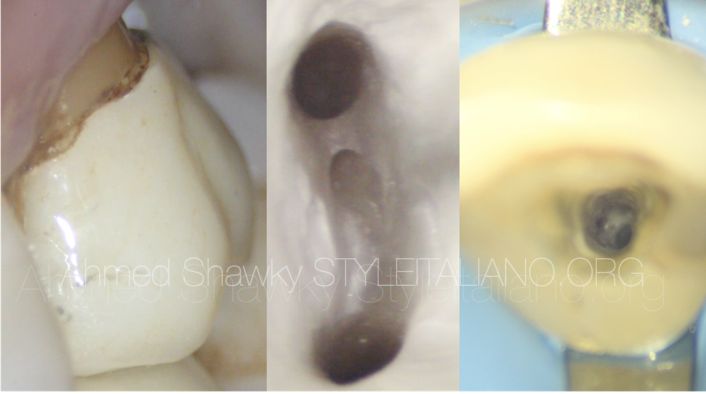
Fig. 1
A well-performed root canal treatment (RCT) increases the probability for the tooth to continue to function normally inside the mouth for a significant amount of time [1]. Today, the success rate of RCT is around 98% (2). After root canal treatment, the long-term success of a treated tooth depends on the amount of residual tissue, bacterial reduction and three-dimensional sealing of the canal system. The resistance and configuration of dentin through age and function are nowadays a key point of research in this field [2].
Endodontic philosophy today promotes a more conservative approach. There are many new technologies, materials, and processes have made it feasible. The importance of efficacy and a conservative therapeutic strategy cannot be underestimated [3]. This innovative type of root canal treatment known as minimally invasive endodontics (MIE), aims to minimize structural alterations after mechanical preparation of the canal system [2].
Perform root canal treatment properly to treat and prevent pulp diseases and apical periodontitis, while preserving as much dental tissue as possible, are part of the MIE method. This treatment is safe, accurate and provides more structural resistance to the tooth [4]. Endodontic procedures are now less invasive due to the development of new materials and technology, such as magnification, cone beam computed tomography (CBCT) and 3D designs of access guides [5].
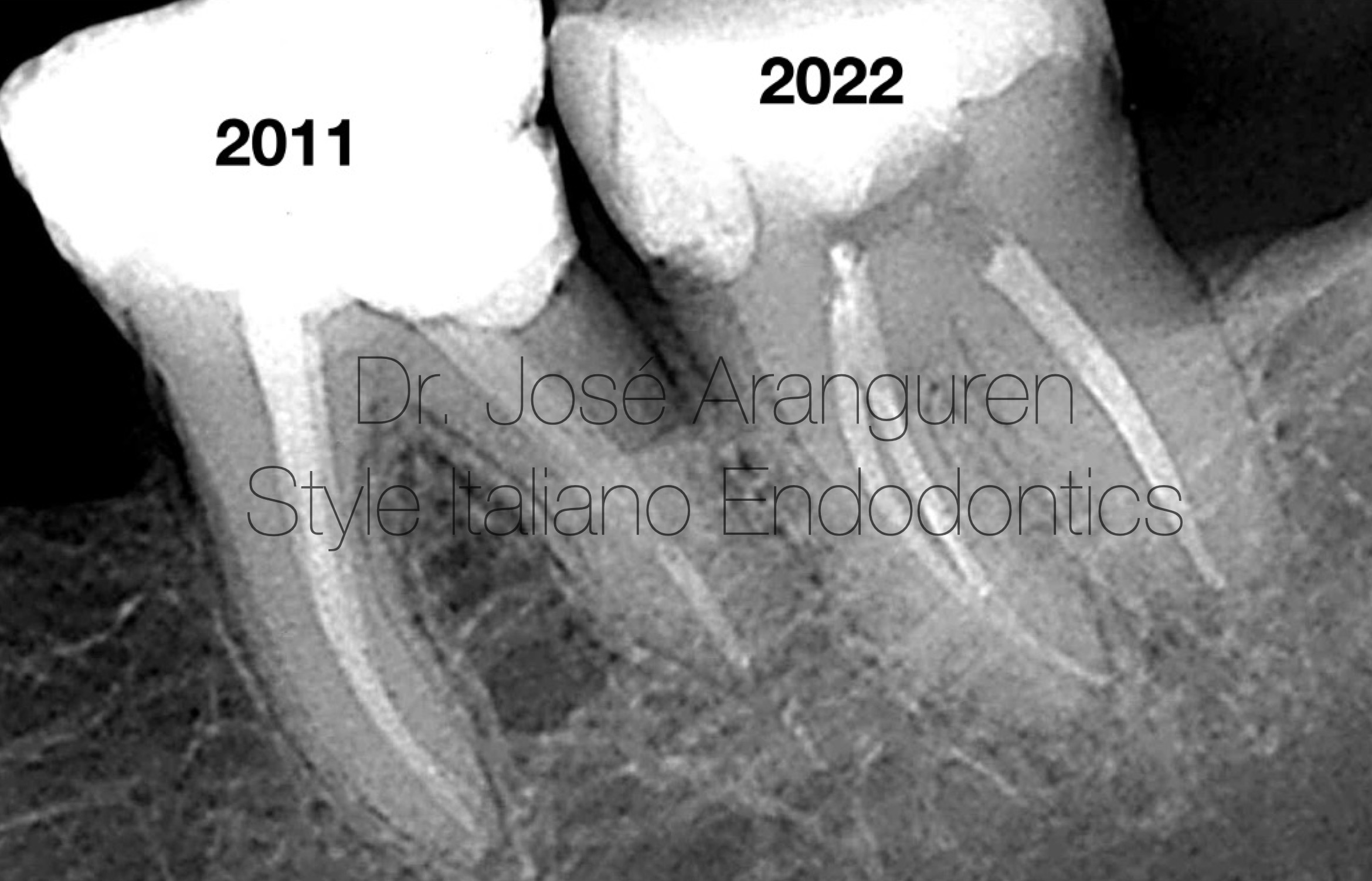
Fig. 2
Treatment performed on the same patient by the same specialist (Dr. Aranguren), 11 years of difference.
Brushing vs Pecking motion, more inserts (more time) vs Kiss and bye. For this minimal invasive shaping, bioceramics is a great help. Single cone technique is an easy and reproducible procedure in these narrow canals.
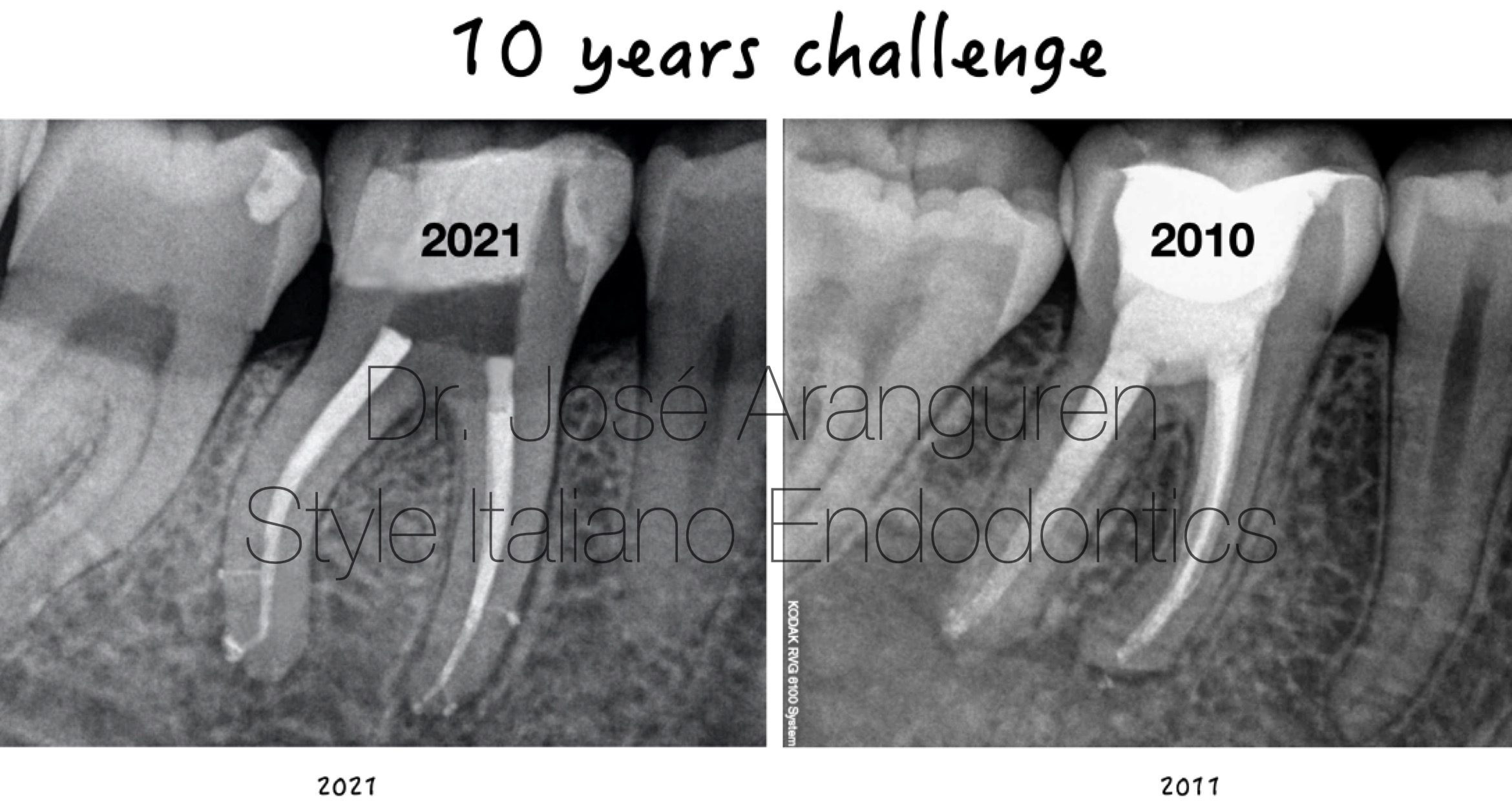
Fig. 3
To resist the compressive stresses of obturation techniques and masticatory forces, root dentin preservation is key.
The current philosophy of instrumentation has completely changed. Today we try to prepare the canals less and to make them resemble the original anatomy as much as possible. The instrumentation techniques are also less invasive and the design of the instruments is getting smaller and smaller.
It has been shown that larger apical diameters and small tapers have a disinfection capacity similar to that of conventional techniques, halving the dentin destruction of the canal. (6). These instrumentation techniques preserve much coronal dentin but also complicate irrigation and obturation procedures for the clinician. New materials such as plastic needles (Irriflex, PD, Vevey, SUI) and bioceramic sealers reduce these possible complications. Figure 2: Instrumentation has changed a lot in recent years. Today we prepare less canals while preserving much more pericervical dentin. To get this minimal shaping we need to use smaller instruments (less taper) and not brushing movements. The more time the file is in the canal and the more number of inserts, the more canal transportation and more coronal enlargement.
Instrumentation has changed a lot in recent years. Today we prepare less canals while preserving much more pericervical dentin.

Fig. 4
Numerous investigations demonstrate the superior centering and dentin preservation provided by the new nickel-titanium file technology and its new alloys[4].
Instrumentation technique has also changed considerably. Before, we were used to preparing the canals for a longer time and with more passes of the files through the root canal. It is clear that the more time and more passes of the files through the canal, the more deformation and widening of it.
What we recommend is a reduction in instrumentation time. Today files with high cutting capacity and great flexibility (new heat treatments) make us faster and safer in instrumentation techniques, significantly reducing deformation and transport within the canal. Rotary systems are made up of a series of instruments, the first of which is generally the one that does 80% of the work. This instrument should be used with the pecking motion technique and not "brushing" as previously proposed. With this, we will significantly reduce the wear of the pericervical dentin.
Minimal invasive Shaping of 4 different rotary systems:
Slim Shaper(Zarc) 35.03 (SS), Trunatomy (Dentsply) 35.04 (TA),
Rotate (Dentsply) 30.04 (RO) and Race Evo 30.04 (RE).
In all the cases the coronal persevation is amazing.
The rest of the files must be used with a single insertion, and once the working length is reached, remove the instrument definitively from the canal (“Kiss and bye”). To be able to work so directly with the finishing files, we need to work at high speed (RPM) and high torque (N/cm) so that the file does not stop in its direct introduction to the apical third. To be able to work with this type of technique we need our instruments (files) to be efficient and for this their cutting capacity must not be altered. For this reason, I recommend using new files practically always, especially if we are going to face a case of high difficulty.
Instrumentation has changed a lot in recent years. Today we enlarge less canals while preserving much more pericervical dentin. This is achieved due to two reasons:
- The files are smaller (smaller taper).
- The time reduction of the use of the files, as we have described above.
Second lower molar video.
In the attached video we can see how nowadays it is possible to instrument a molar (in this case a molar with maximum difficulty) up to a diameter of 40 in apical without widening or deforming the coronal third. This is possible today thanks to the new minimally invasive files (smaller taper and great flexibility).

Fig. 5
In the video we can see how nowadays it is possible to instrument a molar (in this case a molar with maximum difficulty) up to a diameter of 40 in apical without widening or deforming the coronal third. This is possible today thanks to the new minimally invasive files (smaller taper and great flexibility).
The new heat treatments of the files (Blue, Gold, Pink...) give the files a more martensitic behavior with more flexibility, less deformation capacity of the canal and more resistance to cyclical fatigue. For this reason, in minimally invasive endodontics we do not recommend performing compensatory wear since before it was necessary with the old (not very flexible) conventional NiTi files. Today, with the new heat treatments it is no longer necessary, preserving more pericervical dentin.
The instrumentation of the video is done with the Slim Shaper system (Zarc4endo, Gijon, Spain) finishing in a 40 3%.
The new heat treatments provide a better performance of the files and more flexibility. Dual Wire technology (2 alloys in the same file), a new patent from Zarc.
Conclusions
Shaping procedure change so much in the last years, minimal invasive endodontics is a MUST in dentistry today, new materials lead us to work fast, secure and minimal invasive.
- The minimal invasive procedure depends on: smaller files (less taper) , less time the files in the canal (“Kiss and Bye”) and eliminate “brushing” motion.
- The compensatory failing is not needed when we are using martensitic files.
- Plastic needles are needed in this minimal invasive procedures, to penetrate close to working length.
- When it comes to minimally invasive endodontic treatment, the hydraulic qualities of bioceramic sealers help create a solid 3D bond, and the root canal is shaped to match the canal's morphology.
Bibliography
1. Minimally invasive endodontics: saving the precious dentin. Taneja S. J Dent Spec. 2021;9:44–45. [Google Scholar]
2. Selehrabi R, Rotstein I. Epidemiologic evaluation of results of orthograde endodontic retreatment J Endod 2010;36:790-792.
3. Minimally invasive endodontics. Shibu TM, Julie SR. J Dent Oral Hyg. 2014;6:36–38. [Google Scholar]
4. Preserved for endurance: minimal invasive endodontics. Chethan M, Revathi K, Natesan R, Rashmi M, Soubhagya M, Nair VS. IP Indian J Conserv Endod. 2021;6:88–91. [Google Scholar]
5. Minimally invasive endodontics: challenging prevailing paradigms. Gluskin AH, Peters CI, Peters OA. Br Dent J. 2014;216:347–353. [PubMed] [Google Scholar]
6. Effects of Conservative Access and Apical Enlargement on Shaping and Dentin preservation with traditional and moderm Instruments: A Micro-computed Tomographic Study.Aazzouzi K,Ramirez A, Mendez P, Vieira G, Aranguren J, Perez A. J Endod 2023;49(4):430-437.
7. A new perspective on minimally invasive endodontics: a systematic review. Celikten B, Koohnavard M, Oncu A, Sevimay FS, Orhan AI, Orhan K. Biotechnol Biotechnol Equip. 2021;35:1758–1767. [Google Scholar]
8. Traditional and minimally invasive access cavities in endodontics: a literature review. Kapetanaki I, Dimopoulos F, Gogos C. Restor Dent Endod. 2021;46:0. [PMC free article] [PubMed] [Google Scholar]
9. Minimally invasive access cavities: does size really matter? Silva EJ, Versiani MA, Souza EM, De-Deus G. Int Endod J. 2021;54:153–155. [PubMed] [Google Scholar]
10. How biomechanics can affect the endodontic treated teeth and their restorative procedures? Soares CJ, Rodrigues MP, Faria-E-Silva AL, Santos-Filho PC, Veríssimo C, Kim HC, Versluis A. https://www.scielo.br/j/bor/a/TcSFzSrswRrdR7GG9Ckx8Rz/ Braz Oral Res. 2018;32:0. [PubMed] [Google Scholar]
11. In vitro evaluation of the strength of endodontically treated teeth after preservation of soffit and pericervical dentin. Gaikwad A, Pandit V. https://www.ijce.in/journal-article-file/3209 Ind J Conserv Endod. 2016;1:93–96. [Google Scholar]
12. Minimally invasive endodontics and endo-endorestorative-prosthodontic continuum: the right balance? Mahalaxmi S. J Oper Dent Endod. 2019;1:42–53. [Google Scholar]
13. Evaluation of remaining dentin thickness and fracture resistance of conventional and conservative access and biomechanical preparation in molars using cone-beam computed tomography: An in vitro study. Makati D, Shah NC, Brave D, Singh Rathore VP, Bhadra D, Dedania MS. J Conserv Dent. 2018;21:324–327. [PMC free article] [PubMed] [Google Scholar]
14. Biomechanical studies on the effect of iatrogenic dentin removal on vertical root fractures. Ossareh A, Rosentritt M, Kishen A. J Conserv Dent. 2018;21:290–296. [PMC free article] [PubMed] [Google Scholar]
15. Minimally invasive endodontics: a new diagnostic system for assessing pulpitis and subsequent treatment needs. Wolters WJ, Duncan HF, Tomson PL, et al. Int Endod J. 2017;50:825–829. [PubMed] [Google Scholar]
16. Influence of the endodontic treatment on mechanical properties of root dentin. Soares CJ, Santana FR, Silva NR, Preira JC, Pereira CA. J Endod. 2007;33:603–606. [PubMed] [Google Scholar]
17. A literature review of minimally invasive endodontic access cavities - past, present and future. Chan MY, Cheung V, Lee AH, Zhang C. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9035856/ Eur Endod J. 2022;7:1–10. [PMC free article][PubMed] [Google Scholar]
18. Minimally invasive endodontics using a new single-file rotary system - Part 2. . Van der Vyver PJ, Vorster M, Peters OA. https://www.moderndentistrymedia.com/moderndentistrymedia/wp-content/uploads/2020/04/van-der-vyver.pdf International Dentistry (African ed.) . 2019;10:4–20. [Google Scholar]
19. Access cavity preparations: classification and literature review of traditional and minimally invasive endodontic access cavity designs. Shabbir J, Zehra T, Najmi N, Hasan A, Naz M, Piasecki L, Azim AA. J Endod. 2021;47:1229–1244.[PubMed] [Google Scholar]
20. Mechanisms and risk factors for fracture predilection in endodontically treated teeth. Kishen A. Endod Topics. 2006;13:57–83. [Google Scholar]
21. Ten years of minimally invasive access cavities in Endodontics: a bibliometric analysis of the 25 most-cited studies. Silva EJ, Pinto KP, Ajuz NC, Sassone LM. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8411007/pdf/rde-46-e42.pdf Restor Dent Endod. 2021;46:0. [PMC free article] [PubMed] [Google Scholar]
22. Regenerative endodontics and minimally invasive dentistry: intertwining paths crossing over into clinical translation. Elnawam H, Abdelmougod M, Mobarak A, Hussein M, Aboualmakarem H, Girgis M, El Backly R. Front Bioeng Biotechnol. 2022;10:837639. [PMC free article] [PubMed] [Google Scholar]
23. A new approach for minimally invasive access to severely calcified anterior teeth using the guided endodontics technique. Lara-Mendes ST, Barbosa CF, Machado VC, Santa-Rosa CC. https://doi.org/10.1016/j.joen.2018.07.006. J Endod. 2018;44:1578–1582. [PubMed] [Google Scholar]
24. Minimally invasive endodontics a promising future concept: a review article. Mukherjee P, Patel A, Chandak M, Kashikar R. http://www.ijss-sn.com/uploads/2/0/1/5/20153321/ijss_apr_ra02_-_2017.pdf Int J Sci Stud. 2017;5:245–251. [Google Scholar]
25. Minimally invasive endodontics: the expectations and reality. Mostafa NM. https://www.researchgate.net/profile/Nawras-Mostafa/publication/348501323_Minimally_Invasive_Endodontics_The_Expectations_and_Reality/links/6001786c92851c13fe10e2a3/Minimally-Invasive-Endodontics-The-Expectations-and-Reality.pdf J Dent Oral Disord Ther. 2020;8:1–2. [Google Scholar]
26. Minimally invasive endodontics. Bürklein S, Schäfer E. Quintessence Int. 2015;46:119–124. [PubMed] [Google Scholar]
27. Minimally invasive endodontics: a review. Dimri A, Srivastava N, Rana V, Kaushik N. Int J Appl Dent Sci. 2021;7:33–35.[Google Scholar]
28. Minimally invasive and alternative approaches for long-term LVAD placement: the Vanderbilt strategy. Maltais S, Davis ME, Haglund N. Ann Cardiothorac Surg. 2014;3:563–569. [PMC free article] [PubMed] [Google Scholar]
29. Three-dimensional analysis of coronal root canal morphology of 136 permanent mandibular first molars by micro-computed tomography. Fu Y, Gao Y, Gao Y, Tan X, Zhang L, Huang D. J Dent Sci. 2022;17:482–489. [PMC free article][PubMed] [Google Scholar]
30. Modern molar endodontic access and directed dentin conservation. Clark D, Khademi J. Dent Clin North Am. 2010;54:249–273. [PubMed] [Google Scholar]
31. Impact of access cavity design on fracture resistance of endodontically treated molars: a systematic review. Saeed M, Al-Obadi M, Salim A, Alsawaf AY, Hadi K. Clin Cosmet Investig Dent. 2021;13:1–10. [PMC free article] [PubMed] [Google Scholar]
32. Case studies in modern molar endodontic access and directed dentin conservation. Clark D, Khademi JA. Dent Clin North Am. 2010;54:275–289. [PubMed] [Google Scholar]
33. Influence of minimally invasive endodontic access cavities and bonding status of resin composites on the mechanical property of endodontically-treated teeth: A finite element study. Lin F, Ordinola-Zapata R, Fok AS, Lee R. https://doi.org/10.1016/j.dental.2021.12.007. Dent Mater. 2022;38:242–250. [PubMed] [Google Scholar]
34. Comparative evaluation of the impact of minimally invasive preparation vs. conventional straight-line preparation on tooth biomechanics: a finite element analysis. Yuan K, Niu C, Xie Q, Jiang W, Gao L, Huang Z, Ma R. Eur J Oral Sci. 2016;124:591–596. [PubMed] [Google Scholar]
35. Influence of different apical preparations on root canal cleanliness in human molars: a SEM study. Plotino G, Grande NM, Tocci L, Testarelli L, Gambarini G. J Oral Maxillofac Res. 2014;5:0. [PMC free article] [PubMed] [Google Scholar]
36. Minimally invasive endodontics-a review. Arbiya AS, Hegde S, Mathew S. https://www.indianjournals.com/ijor.aspx?target=ijor:jdor&volume=15&issue=2&article=012 Journal of Dental and Orofacial Research. 2019;15:77–88. [Google Scholar]
37. Influence of cervical preflaring and root canal preparation on the fracture resistance of endodontically treated teeth. da Silva PB, Duarte SF, Alcalde MP, et al. BMC Oral Health. 2020;20:111. [PMC free article] [PubMed] [Google Scholar]
38. Influence of minimally invasive endodontic access cavities on root canal shaping and filling ability, pulp chamber cleaning and fracture resistance of extracted human mandibular incisors. Rover G, de Lima CO, Belladonna FG, Garcia LF, Bortoluzzi EA, Silva EJ, Teixeira CS. https://doi.org/10.1111/iej.13378. Int Endod J. 2020;53:1530–1539. [PubMed] [Google Scholar]
39. The restoration of root filled teeth: a review of the clinical literature. Bhuva B, Giovarruscio M, Rahim N, Bitter K, Mannocci F. https://doi.org/10.1111/iej.13438. Int Endod J. 2021;54:509–535. [PubMed] . [Google Scholar]
40. Digital design of minimally invasive endodontic access cavity. Gambarini G, Galli M, Morese A, et al. Appl Sci. 2020;10:3513. [Google Scholar]