
Managing of three rooted upper first premolars
31/05/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Three rooted upper first premolars are one of the most challenging anatomy variation.
The aim of this article is to analyze prevalence, characteristics and management of this particular type of first upper premolars.
The aim of endodontic treatment is to disinfect the root canal system eliminating the most of bacteria: the main cause of endodontic failure is the permanence of microorganisms (intraradicular o extraradicular) due mainly to improper shaping, cleaning and filling. (1)
Knowledge of anatomy is crucial to correctly manage endodontic treatment and to achieve and mantain success.
However the huge variability of endodontic system imply a proper approch to each single case.
One of the most challenging anatomy variation is the first upper premolar presenting three different roots.
The purpose of this article is to analize prevalence and managing of this type of anatomical variant.
The prevalence of upper first premolar with three roots is 0- 9,2 % , the number of canals is three in 100% of the cases(2,3,4)
Occlusal anatomy doesn’t present any particularity but the vestibular face can reveal the present of two vestibular roots: the cercical profile isn’t covex but plane, the difference between mesio-distal diameters in the coronal third and cervical third is less evident than in a normal premolar; with a parodontal probe we can detect the vestibular furcation that present a little development furrow on vestibular face. (2)
The presence of the third root is commonly bilateral.(5)
The xr preoperatory identification isn’ t always easy.
Due to the small diameters of the vestibular roots, shaping have to be extremely conservative(6-7).

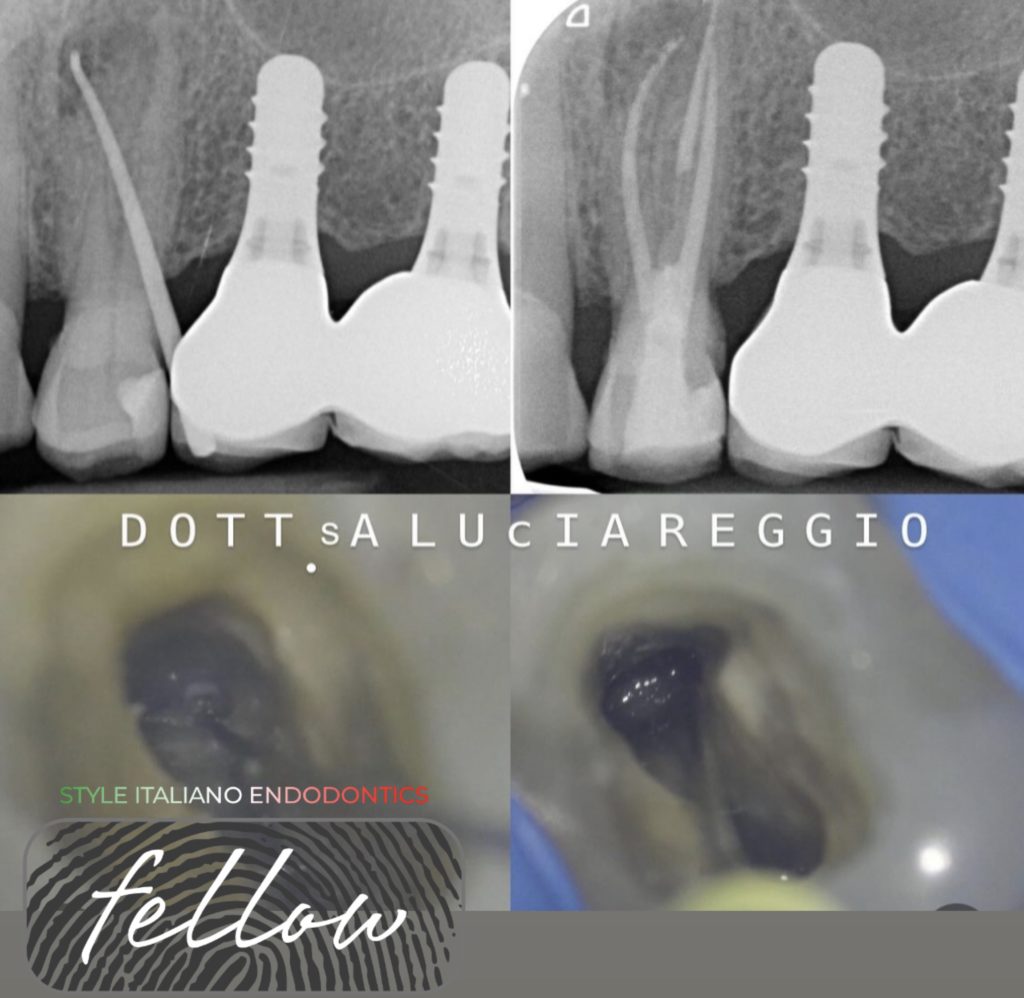
Fig. 1
Case 1: Due to deep level of buccal furcation and to small diameters , in the first phase of shaping, the buccal canals aren’t scoutable : working lenght is reached after US instrumentation to enlarge mesio-distally the access.
Last rx is 8 years follow.
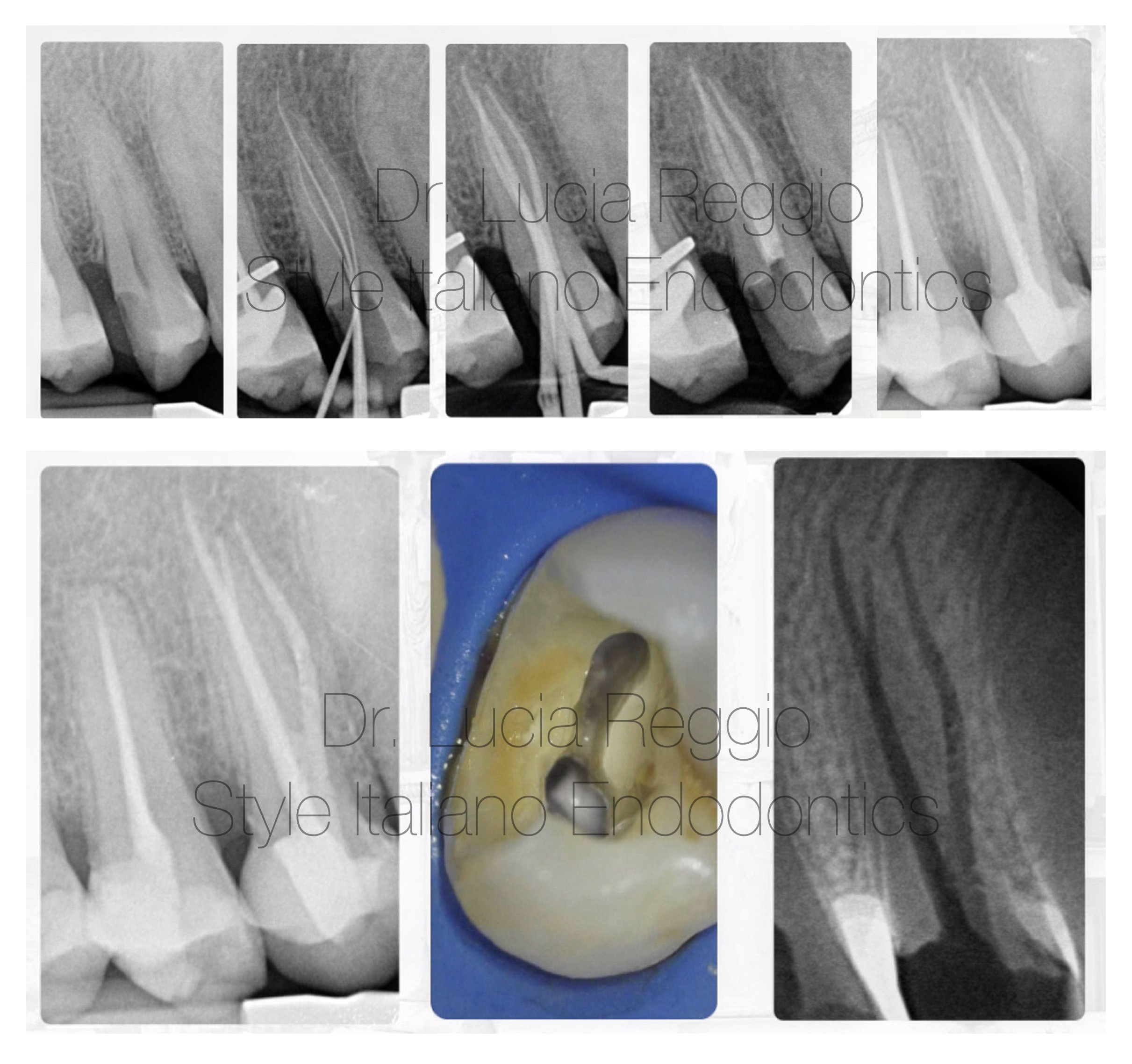
Fig. 2
Case 2: After coronal lengthening procedures and proper rubber dam isolation , chamber opening is managed to allow a conservative shaping, performed by low conicity and hight flessibility reciprocating files.
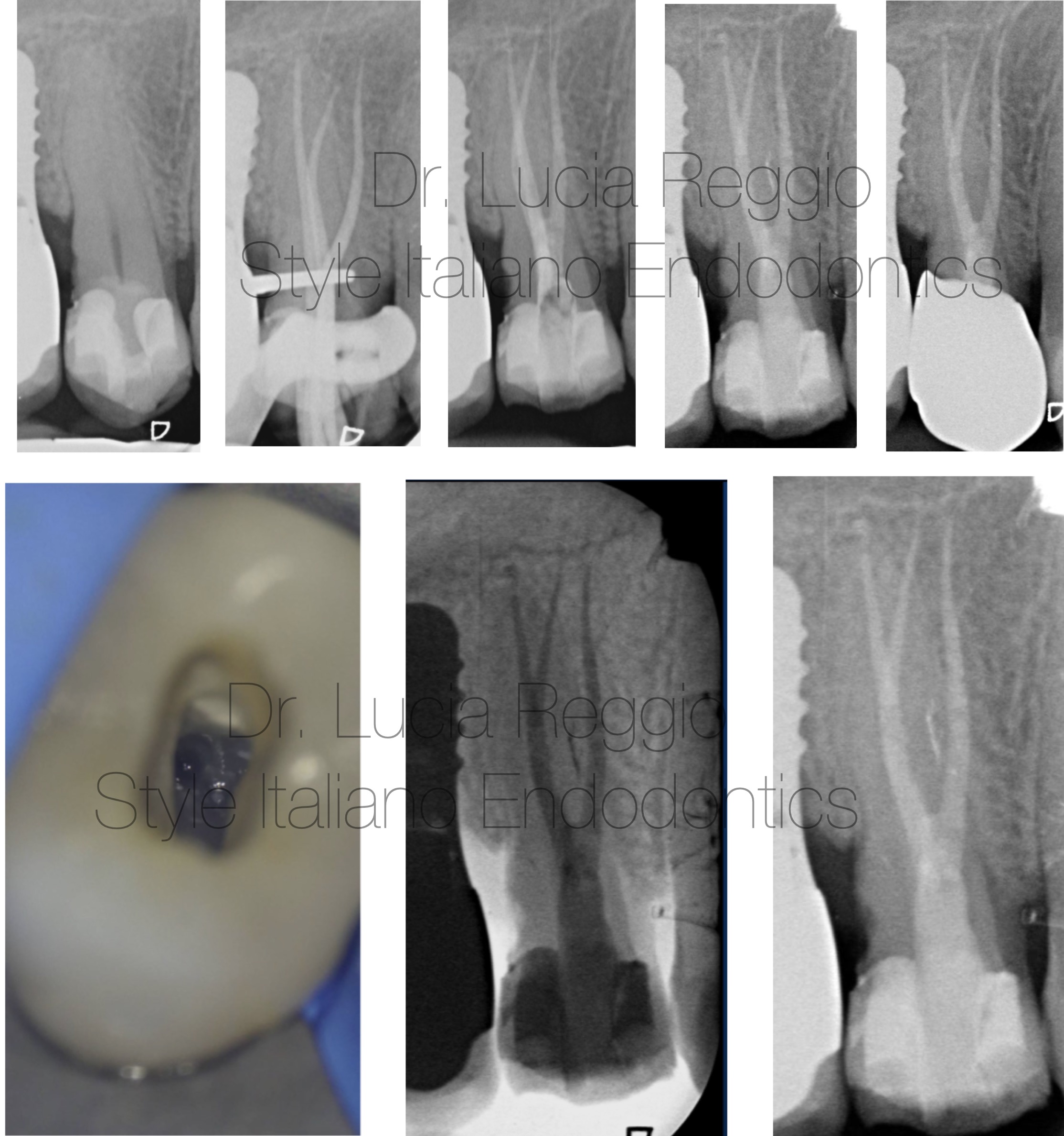
Fig. 3
Case 3: The shape of the chamber is extended in depth and also the palatal canal arise from chamber at a deeper level than usual.
Last rx is 3 years follow up.
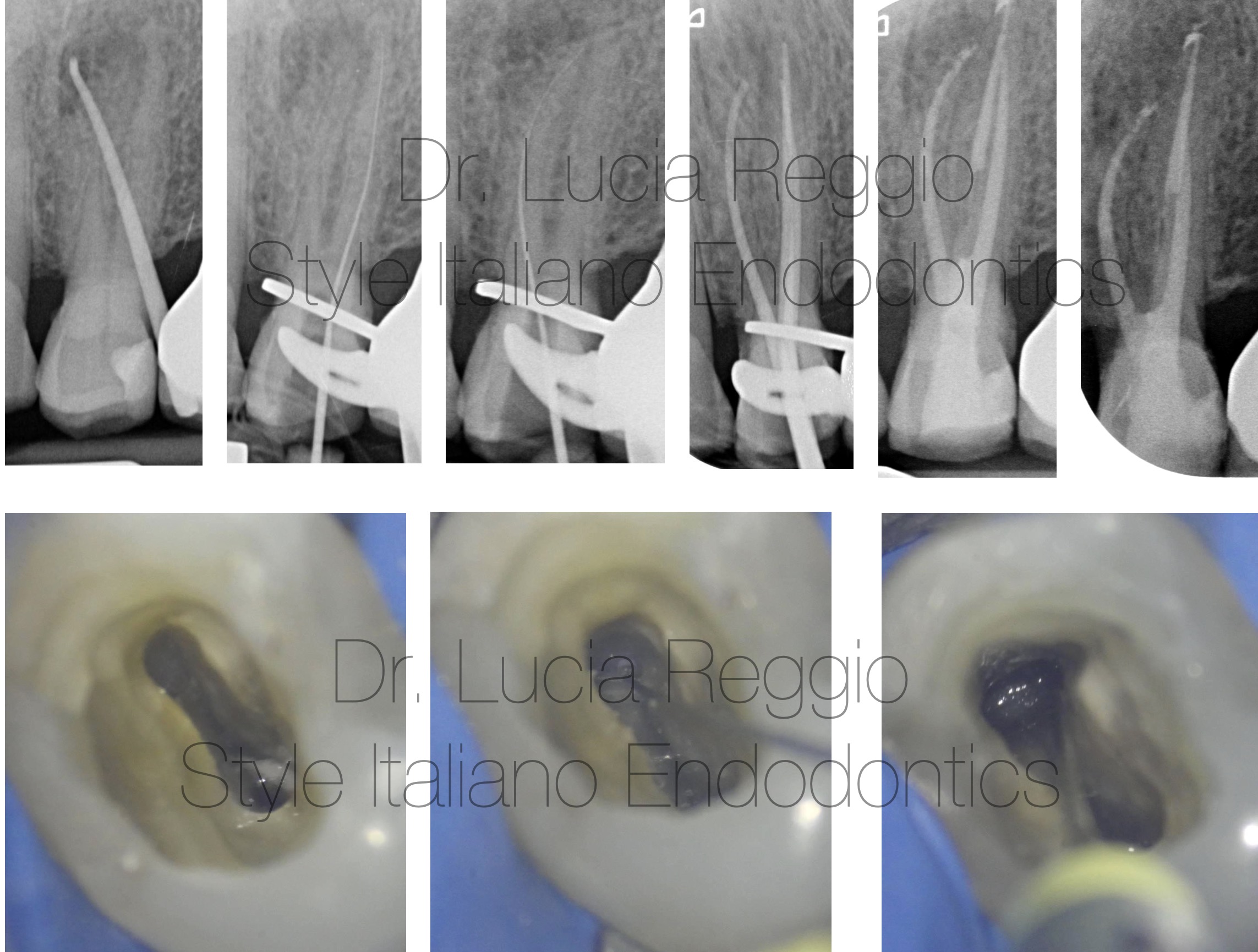
Fig. 4
Case 4: Due to previous cervical composite restauration, the buccal canals are calcified.
US instrumentation with small active points is necessary to reach the buccal orifices.

Fig. 5
This type of anathomy requests a proper management of chamber opening widening the buccal aspect to allow better access to each buccal canal. (8-9).
We can have two differet chamber type: three differt canal orifices that leave chamber separately or buccal root that leave the chamber as a single canal and divide into two separate and distinct canals. (9)
- PREOP DIAGNOSIS: it’s hard to detect this type of anatomy but, there are some elements we can detect before treatment such as the point in which radioopacity becomes quickly less evident that can indicate the point of trifurcation. (fig 5)
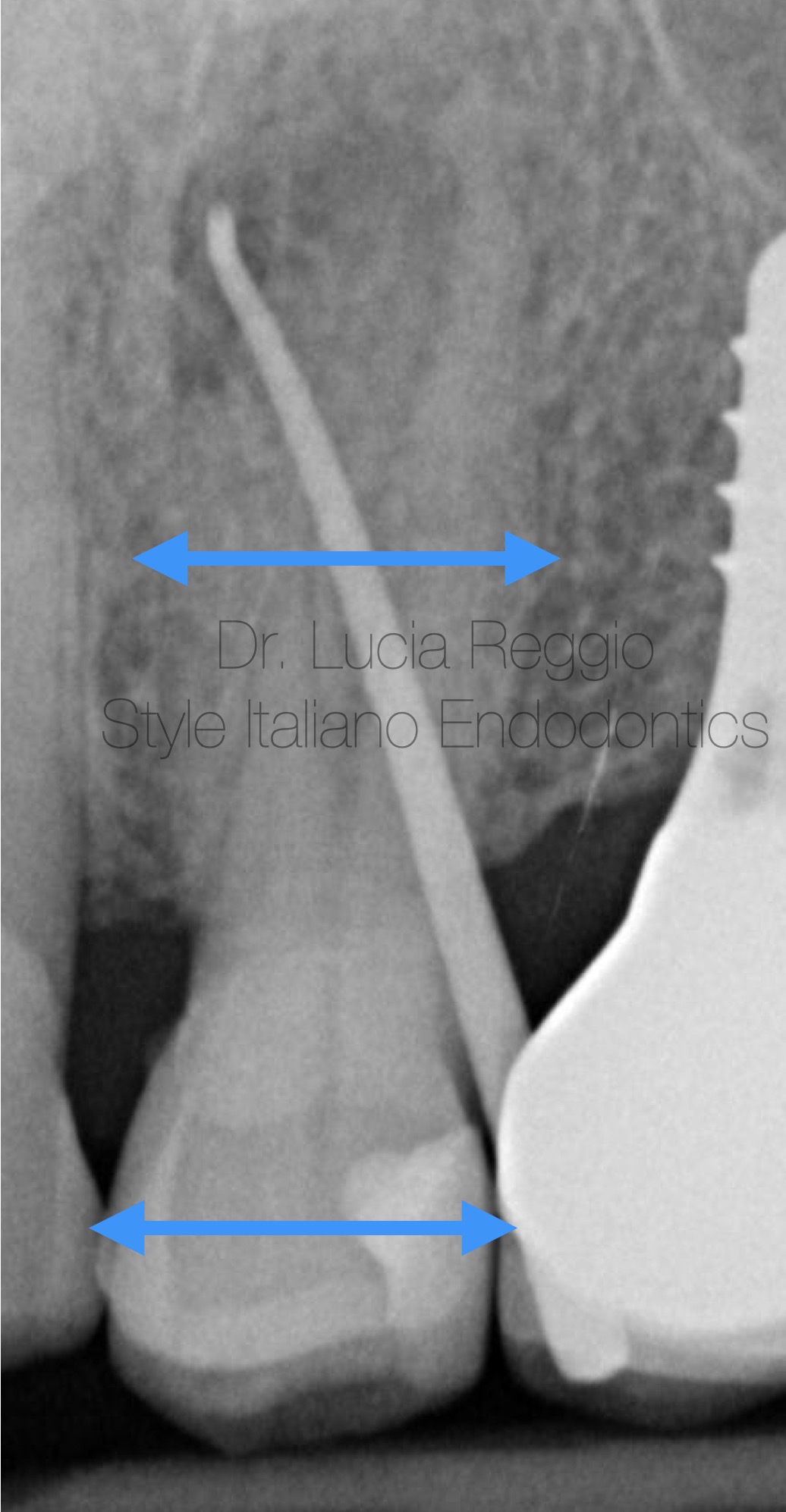
Fig. 6
Another preop xr element to look forthat may suggest the presence of threerooted premolars is that if the mesial-distal width of the mid-root image appears equal to or grater than the mesial-distal width of the crown image, then the tooth most likely has three roots.(8) (fig.6)
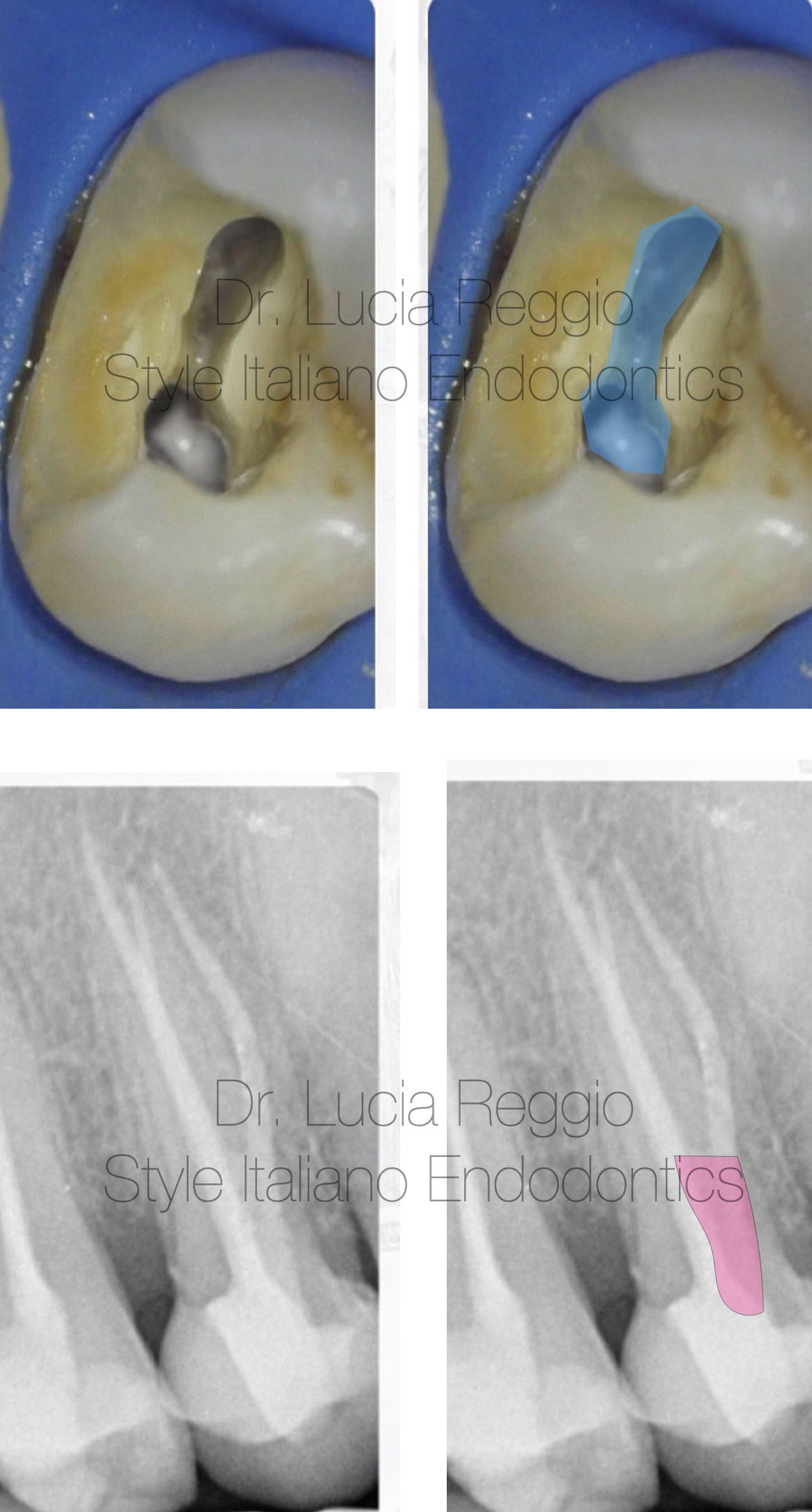
Fig. 7
- CHAMBER OPENING: thre chamber of a threerooted premolar is similar to upper molar chamber reduced in dimension; we requires an access cavity modification into a "T" shape, mesial-distally extending the buccal aspect of the usual outline form. (fig. 7,8)
Another clear sign that identifies this kind of anatomy is a buccal orifice not in line with the cusps like the palatal one.
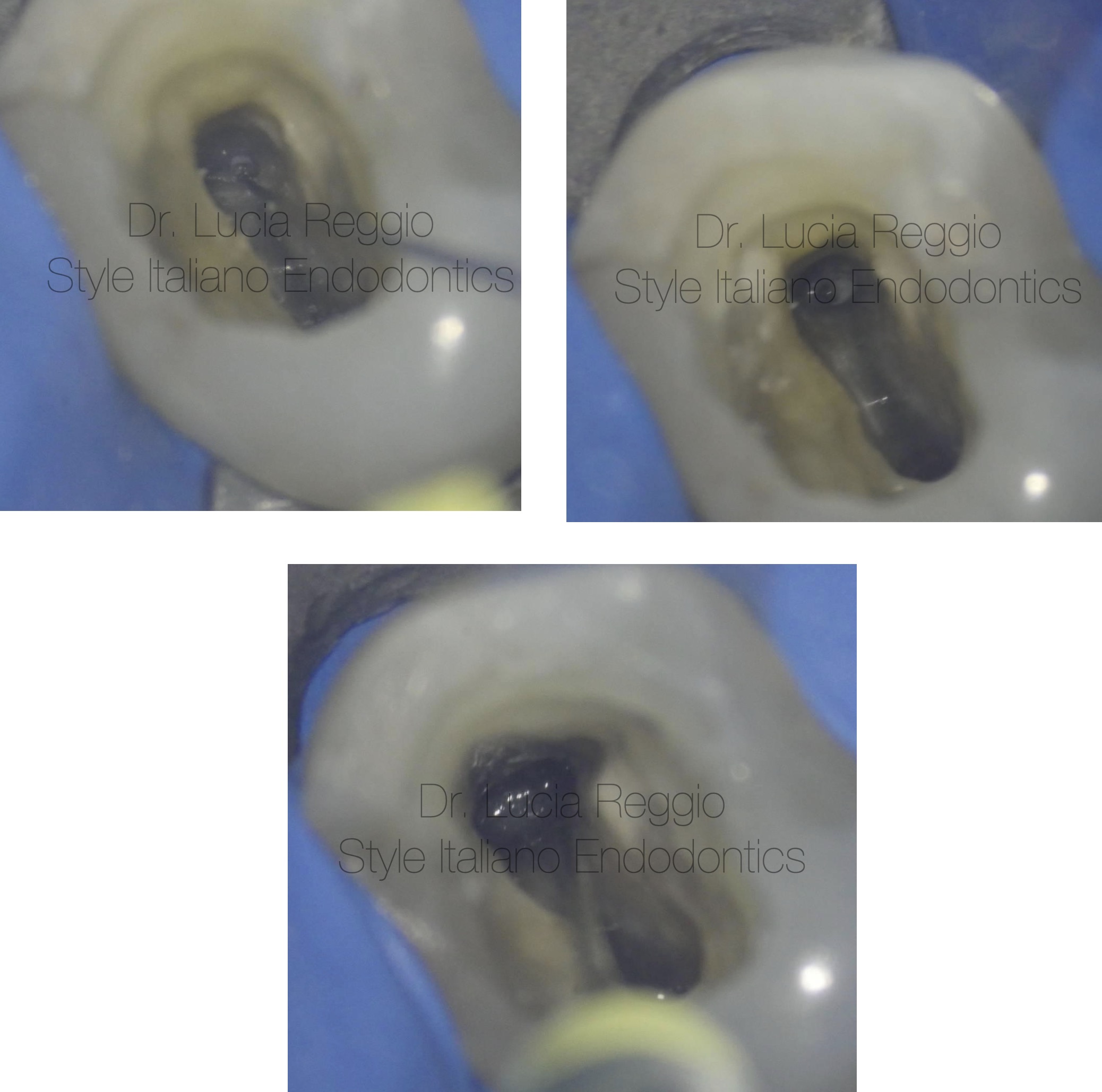
Fig. 8
- INSTRUMENTATION scouting is crucial to identify the curvatures and to allow shaping to be as much conservative as possible.
In case of calcification of the coronal third ultrasonic intrumentation is needed.
In some cases the two buccal canals arise from a common narrow channel which originates from the pulp chamber.
This configuration restricts the access to each buccal canal and produces a “s” shaped curvatures; this situation can be rectified by extending a trough apically in depth, over and between the two canals eliminating the coronal curvatures.(8)(fig.11)
Intracanal preparation have to be the more conservative as possible due to the small diameters of the roots, avoiding lateral strip perforations or dentinal cracks.
- CLEANING: cleaning phase need hypoclorite activation to reach all the endodontic space including apical third, because of Irrigant replacement was limited to 1-1.5 mm apical to the needle tip, expecially in small diameters.(10)
- OBTURATION: obturation technique must be choosen related to anathomy. Vertical warm condensation could be used provided that small heat pluggers passively reach 4-5 mm to the WL. Carrier techniques and single cone technique are effective alternatives
- .POST-ENDO RESTORATION: If a core post build-up is needed is much more preferable to place the post in palatal root avoiding further dentin removal.

Fig. 9
Lucia Reggio graduated with honours in 2008 at Turin University.
She won Industrial Union Optime premium as best graduate of the year.
She was co-owner of University course in orthograde and retrograde endodontics at San Luigi Gonzaga, Orbassano . She is active member of the Italian Society of Endodontics. From 2020 to 2022 she was part of the comunication committee of the Italian Society of Endodontics and from 2023 to 2024 she was the cultural coordinator of north-west macro area of the Italian Society of Endodontics.
She is speaker in several courses and lectures.
She is fellow of Style Italiano Endodontic.
She is certified international opinion leader in endodontic and restorative.
She is responsible and coordinator of the conservative and endodontics clinical area of Studio Favatà Savio in Turin and she mainly applies in endodontics and adhesive restorative.
Conclusions
Anatomy is hugely variable and there cannot be a single approach to every endodontic treatment.
Three rooted upper premolars are one of the most challenging anatomical variation because of the small diameters and the difficult of proper access.
A scrupulous preoperative diagnosis is necessary to a proper management of endodontic treatment of three rooted upper premolars.
Specific modifications in access, shaping, cleaning and obturation phases can lead to a succefull approach.
Bibliography
- Influence of microbiology on endodontic failure.Literature review. I.Prada et al Med Oral Patol Oral Cir Bucal 2019 May; 24(3):e364-e372
- Testo atlante di anatomia endodontica Gagliani M., Fornara R. et al. Ed: Tecniche Nuove, 2011: 77-91
- Woelfel JB. Dental anatomy : its rilevance to dentistry. IV ed Philadelphia: Lea and Febiger, 1990:81-103.
- Lipski M et al. Root and canal morphology of the first human maxillary premolar. Durham Anthropology J 2005:12:2-3
- Sabala CL et al. Bilateral root and canals aberrations in a dental school patient population. J endod 1994; 20:38-42
- Bellucci g. et al A study on the thickness dentine and cementum in anterior and premolar teeth. Int Endod J 2002;35: 594-606
- Gimlin DR et al A comparison of stresses produced during lateral and vertical condensation using engineering models. J Endod 1986:12;235-241
- Sieraski SM et al. Identification and endodontic menagement of three-canalled marillary premolars. J endod 1985;15:29-32
- Balleri P et al. Primer premolar superior con tres raices. Endodontic practice1997;3:13-5
- 10.Boutsioukis C et al Irrigant flow within a prepareted root canal using various flow rates:a computational fluid dynamic study.Int Endod J 2009;42:144-55



