Management of severe trajectories: a clinical perspective
22/07/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The curved and dilacerated roots in the posterior teeth often present the major challenge to the clinicians during the endodontic treatments.
Failure to secure a safe glide path in order to achieve an optimum biomechanical preparation may lead to complications which will jeopardize the final outcome of the treatment due to :
- Ledges.
- Zip formation.
- Apical transportation.
- Perforations.
- File separation.
Planning should start by proper analysis of the pre operative radiography and access cavity preparation before any intracanal intervention.

Fig. 1
A referred case of tooth no. 36 with a previous inadequate treatment due to inability of the referring doctor to deal with due to multiple curvatures
Patient complained of persistent symptoms of apical periodontitis
After analysis of the preoperative radiography , I started to remove the temporary filling then removing the intracanal filling.

Fig. 2
After removing most of the intracanal filling and checking working length
We should avoid :
- Forcing instruments in a curved canals
- Using stiff and large instruments
- Leaving the rotating file for full length more than just a seconds i.e. just kissing the apical constriction to avoid torsional separation of the file.

Fig. 3
Shaping done safely and here is the final outcome

Fig. 4
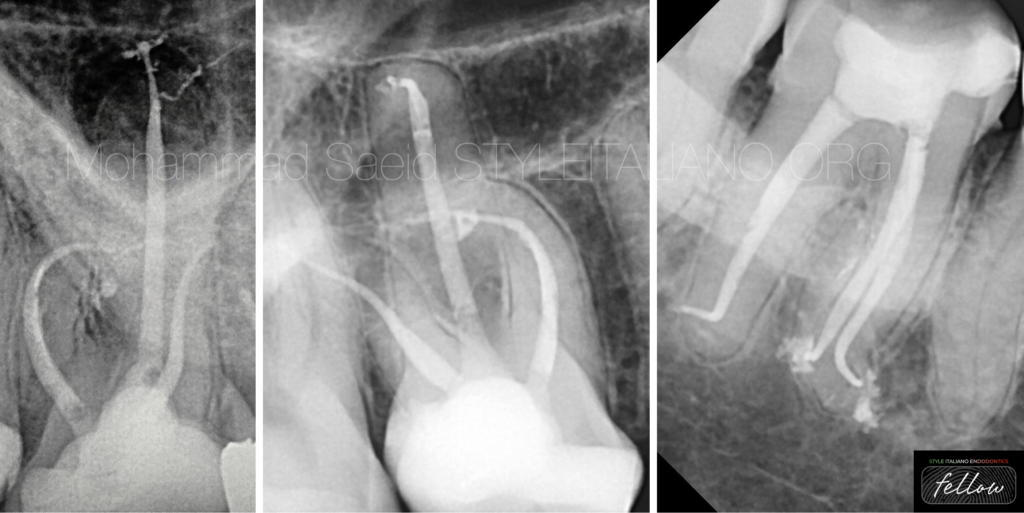
Here is a case of tooth no. 48 that the patient insisted to keep with coronal and severe apical curvature and very small radius

Fig. 5
Scouting done to determine shaping protocol, radius was very small so I decided here to end up at 20.04 and more focus on irrigation
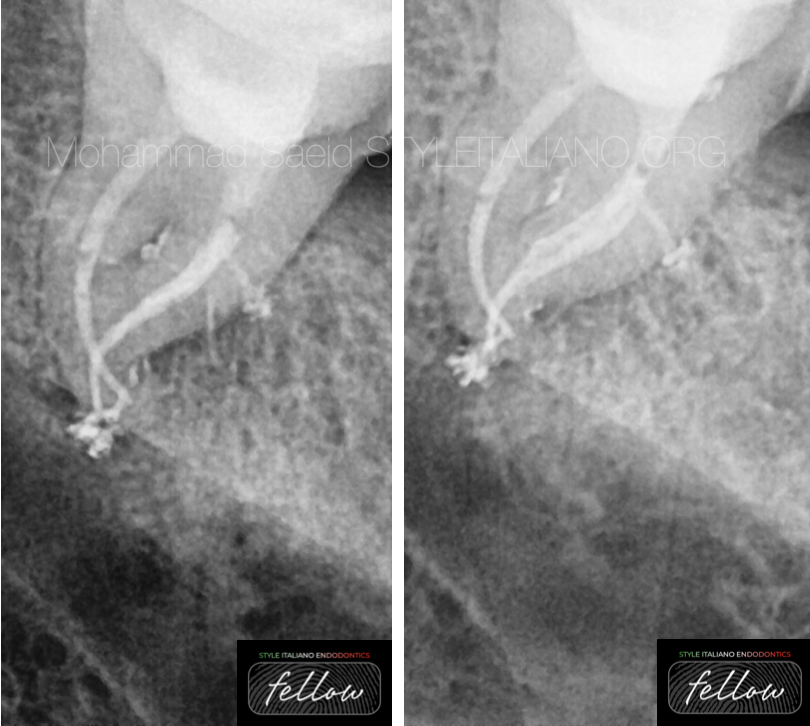
Fig. 6
Final radiography with lateral canals filled

Fig. 7
Tooth no. 16 that is almost SOLID with an old amalgam filling and proximal caries with symptoms of acute irreversible pulpitis
After removal of the restoration and caries excavation, a dedicated ultrasonic tip was used to remove calcification in the pulp chamber and exploring canal orifices
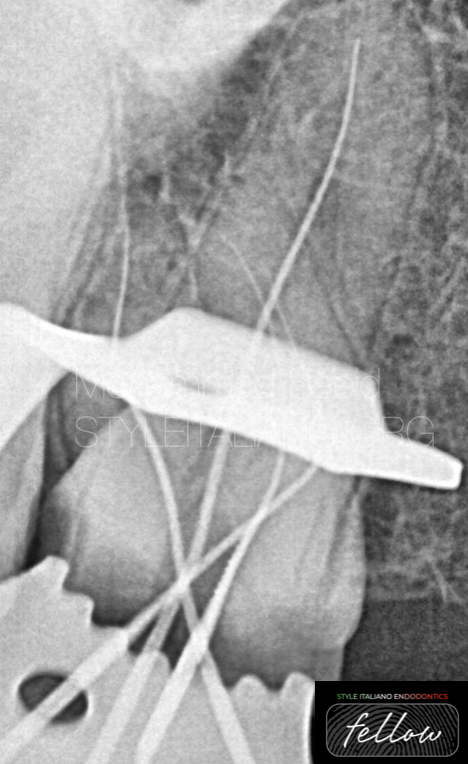
Fig. 8
First attempt resulted in failure to reach the length due to severe coronal curvature of MB2
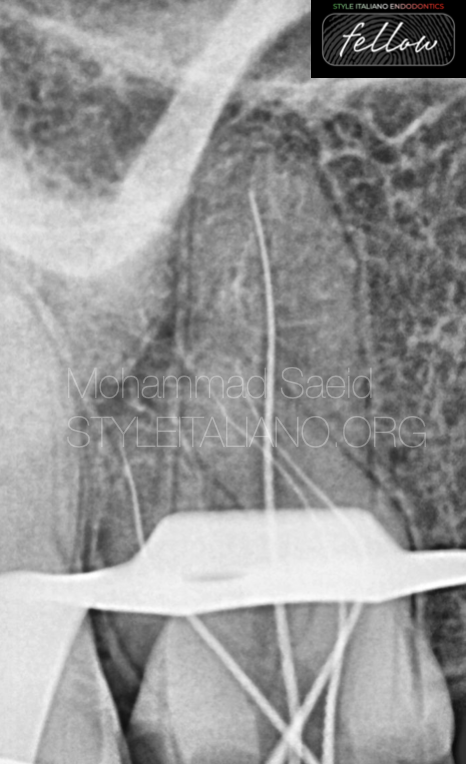
Fig. 9
Access cavity modification and orifice relocation done with the help of ultrasonic and orifice opener to reach the full length.

Fig. 10
The final radiography with different angles showing the multiplanar curvature of MB2

Fig. 11
About the author:
BDS - Cairo university 2001
Endodontic specialist.
Lecturer in the field of minimally invasive endodontics.
Part time consultant endodontics in private dental centers in Cairo.
StyleItalianoEndodontics Fellow.
Conclusions
The preoperative analysis and planning a head when dealing with curved canals along with types of files and decisions regarding type of access cavity, orifice relocation and choosing the final shaping file size should all be in mind to guarantee a successful treatment.
Bibliography
Jafarzadeh H, Abbott PV. Dilaceration: review of an endodontic challenge. J Endod. 2007;33:1025–30.
Estrela C, Bueno MR, Sousa-Neto MD, Pécora JD. Method for determination of root curvature radius using cone-beam computed tomography images. Braz Dent J. 2008;19:114–8.
Ruddle C. Cleaning and shaping the root canal system. In: Cohen S, Burns R, editors. Pathways of the Pulp. 8th ed. St. Louis, MO: Mosby; 2002. pp. 231–92.
Mounce R. Negotiating challenging mid root curvatures: Rounding the bend. Dent Today. 2007;26:108. 110, 112.
Ankrum MT, Hartwell GR, Truitt JE. K3 Endo, ProTaper, and ProFile systems: Breakage and distortion in severely curved roots of molars. J Endod. 2004;30:234–7.