

Management of Multiplanar Curvature
24/11/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The presence of root canal curvature introduces various factors that heighten the risk of iatrogenic complications during root canal treatment. These factors include the inability to achieve patency in the apical third, ledges, apical transportation, instrument fractures, and perforations resulting from asymmetrical dentine removal along curved pathways. These complications can jeopardize the effective management of intraradicular infections and lead to suboptimal treatment outcomes.
Managing severely curved S-shaped, multiplane-curved root canals presents a significant technical challenge. Throughout the history of endodontics, various instruments and techniques have been developed to manage nearly all anatomical variations of root canals. In this context, a novel root canal instrumentation technique is proposed, which combines principles from both the Schilder Stepdown Technique and the McSpadden zone technique.
In the Stepdown Technique, The root is conceptually divided into three thirds: the coronal, middle, and apical thirds. This partitioning serves to streamline the shaping by breaking it down into a sequence. This Technique has shown remarkable advantages. It enhances access to the apical region by eliminating coronal obstructions, offering improved tactile control during procedures. Furthermore, it promotes more effective cleaning by increasing irrigant volume, resulting in reduced post-operative complications, particularly in necrotic teeth.
The Zone Technique, developed by McSpadden in 2007, differentiates between two areas within the root canal: the coronal zone (located above the canal's curvature) and the apical zone (below the curvature. By using this technique, the pressure exerted on files entering the apical area is reduced, thereby minimizing the probability of procedural errors.
In routine endodontics, the conventional diagnostic and treatment planning tools consist of single or multiple periapical radiographs. These two-dimensional representations, while valuable, only partially capture the complexity of the three-dimensional root canal system. however, three-dimensional imaging techniques, such as computed tomography (CT), are increasingly popular in endodontics due to their significant advantages. CT provides high-resolution images, thereby improving both qualitativ and quantitative assessments of the root canal system. however, it's important to note that CT is associated with factors like increased time, greater radiation exposure, and elevated costs, making it less suitable for routine endodontic procedures.
Assessing root canal curvature involves the evaluation of various factors, including degree, radius, level, length, and height. Throughout the history of this field, a wide range of techniques have been proposed for this cause.
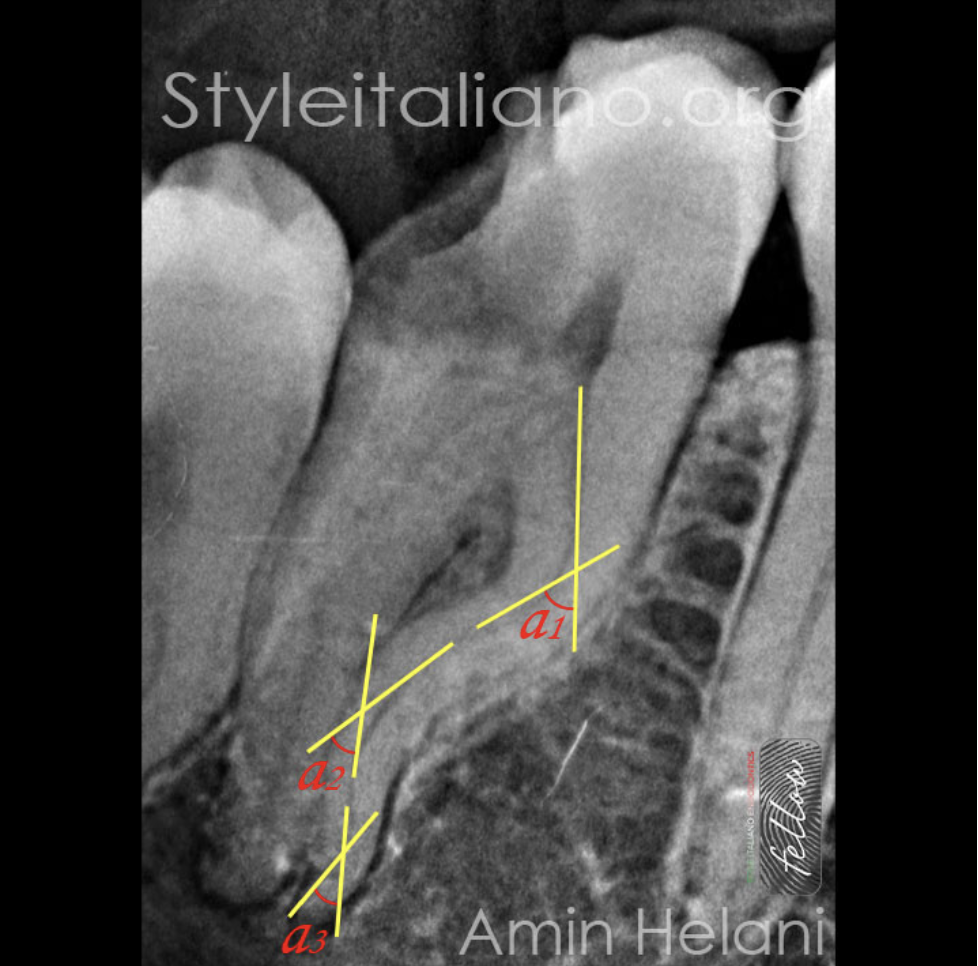
Fig. 1
Schneider proposed a method defining an angle as the space between two lines or surfaces at the point at which they touch each other, When two angles share a common vertex, their other sides together form a straight line (α + β = 180°), making them supplementary. Most studies and research utilize supplementary angles to assess root canal curvature.
The greater this angle, the higher the canal curvature, thus making the management more challenging.
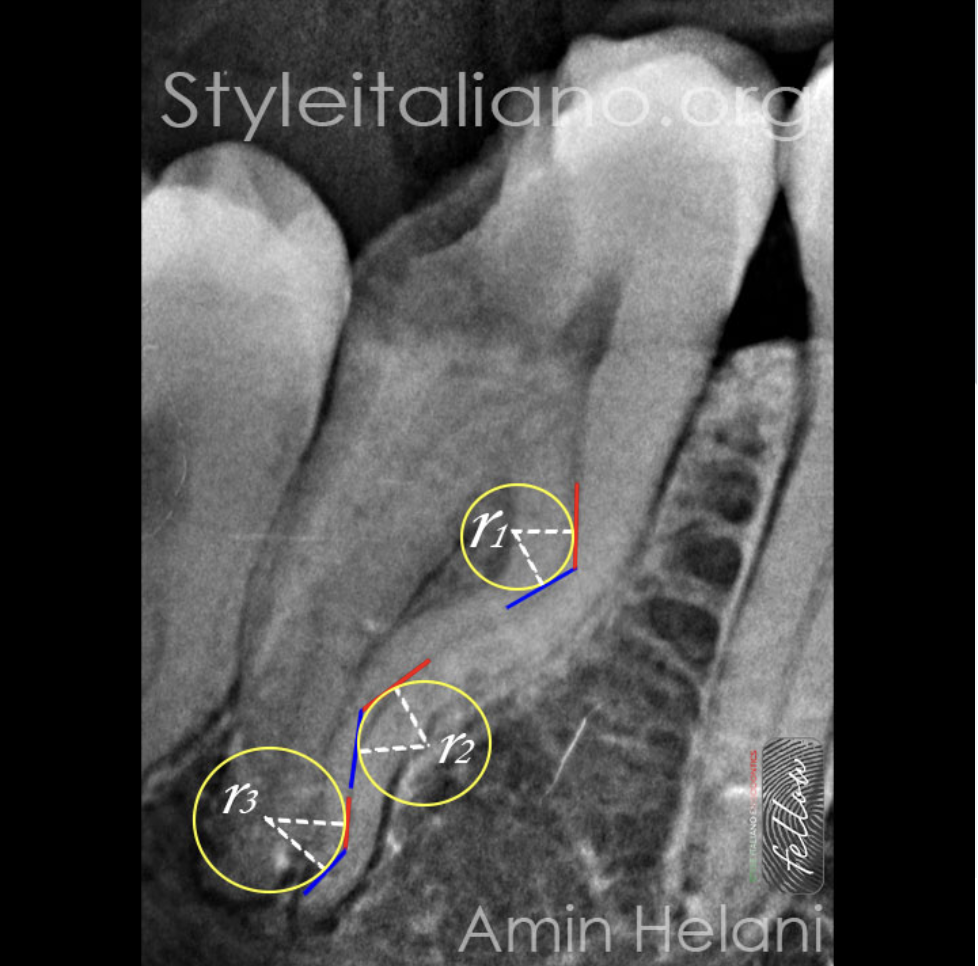
Fig. 2
Many studies highlight the insufficiency of using the angle of curvature alone to describe the curvature. with radius being a second parameter with an effect on the root canal treatment difficulty . Furthermore, other factors like the position, level, shape, and height of the curve should be considered to better understand root canal morphology.
the method to determine the curvature radius involves using two 3 mm semistraight lines over the root canal. The primary line (blue) represents the apical continuity, and the secondary line (red) represents the coronal region. The circumcenter is determined at the midpoint of each semistraight line, and the distance between the circumcenter and the center of each semistraight line defines the radius of the circumference, indicating the degree of root curvature. These values classify root curvature as small (r≤2 mm, severe curvature), intermediary (r>2 and r≤4 mm, moderate curvature), or large (r>4 mm, mild curvature).
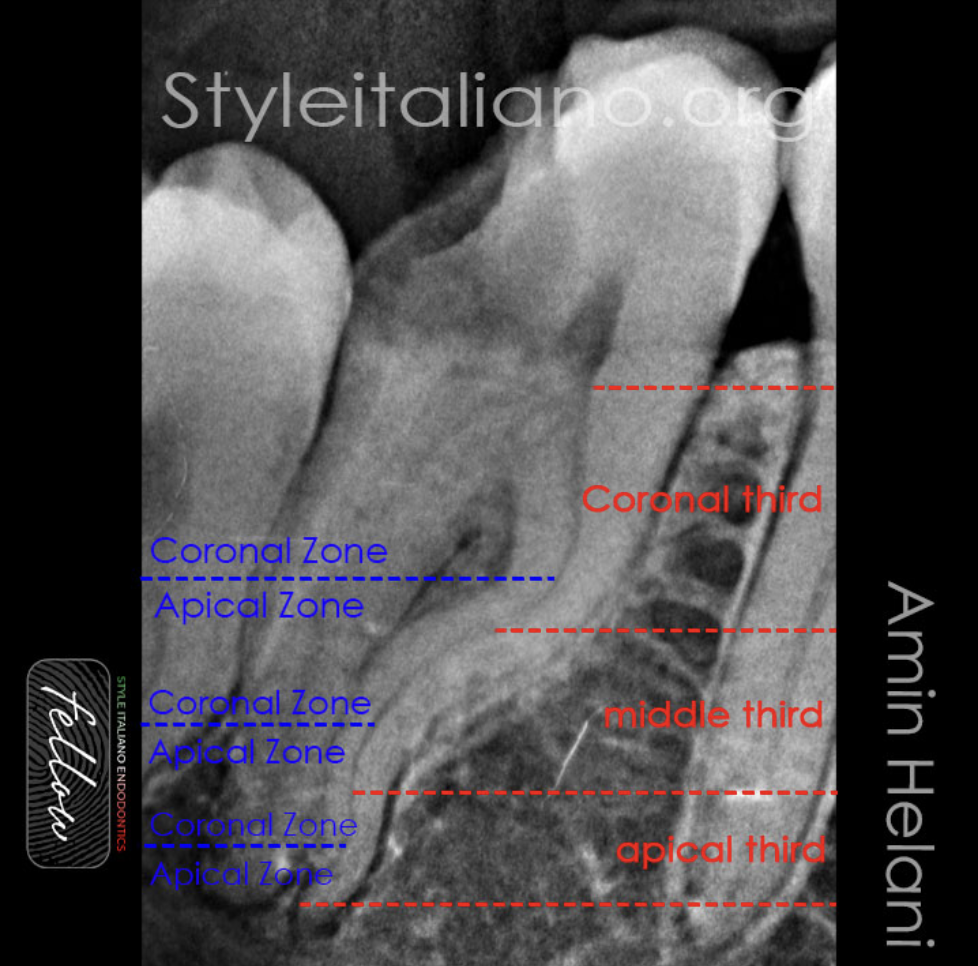
Fig. 3
In red, the canal was divided into three thirds using the Stepdown technique: coronal, middle, and apical. In blue, each curvature was divided into two zones using the Zone technique: coronal (above the curvature) and apical (below the curvature).
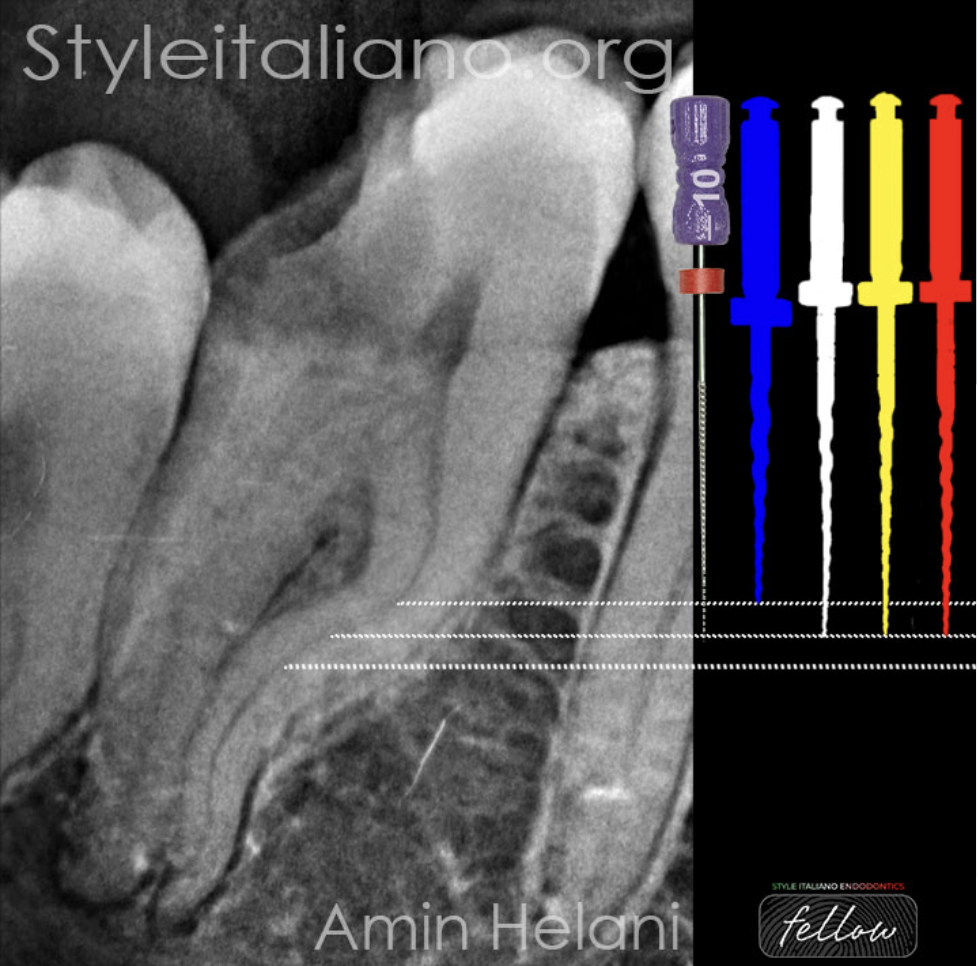
Fig. 4
Both the Step Down and Zone techniques emphasize the gradual use of files, shaping each third or section of the canal as if it were a separate canal.
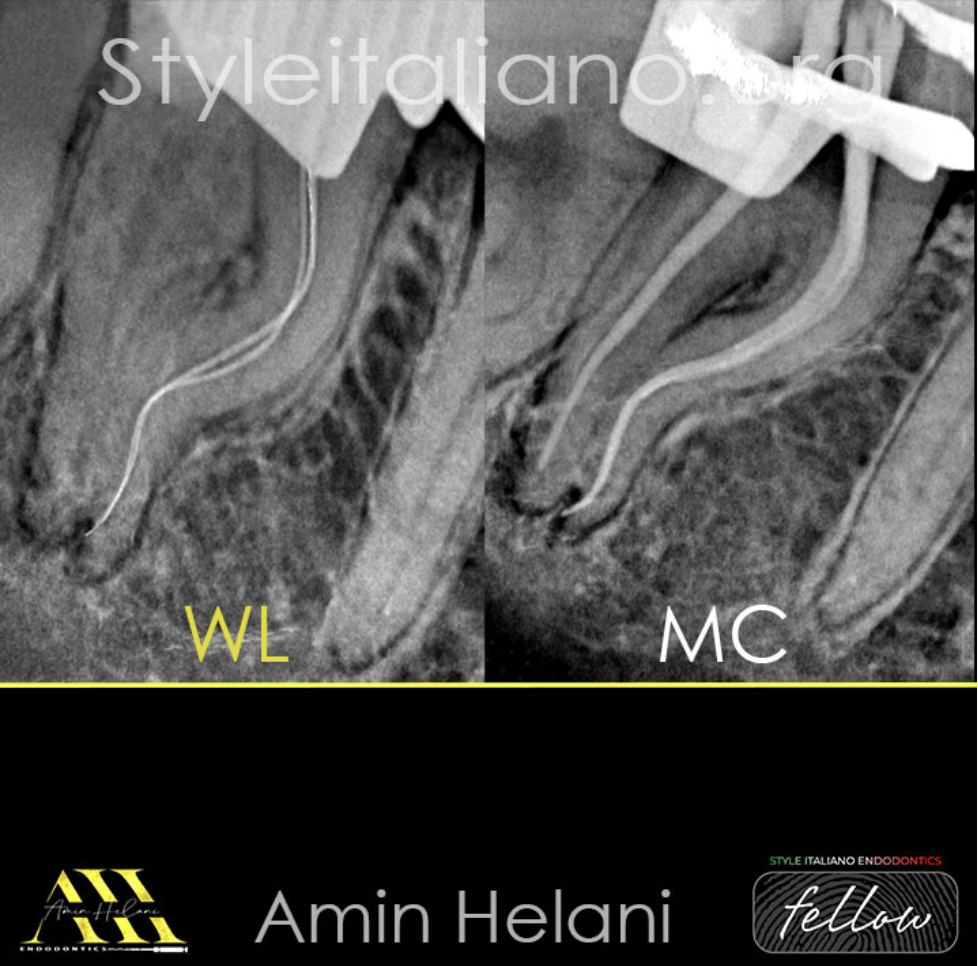
Fig. 5
The working lenght is determined after reaching the apical region, and the Master-Cone radiograph is taken after completing the shaping to ISO 25 taper 4%.
A video demonstrating the process of irrigation using a flexible root canal irrigation needle (Irriflex) and activation using Sonic activation (Endoactivator), as well as intracanal heating with System-B.

Fig. 6
The Post-Op radiograph shows adequate obturation of the root canal systems.

Fig. 7
Case 2:
A 45-year-old man presented with symptomatic irreversible pulpitis. Radiographic examination revealed an S-shaped double-curved root and a sound appearance of periapical tissues.

Fig. 8
After planning, the Shaping is done gradually using heat-treated files to ISO #25 taper 4, and obturation is completed using the single cone technique with bioceramic sealer.

Fig. 9
About the author:
Dr. Amin Helani graduated in 2014 from the University of Aleppo in Syria.
• In 2021, he received a specialist degree in Endodontics from the German Society of Endodontics.
• He works as a Microscopic Endodontist for advanced root canal treatment in Braunschweig, Germany.
• He has been offering lectures, webinars, and hands-on courses to both general dentists and endodontists.
• He is a member of the German Society for Endodontology and Traumatology.
• He is a fellow member of Style Italiano Endodontics.
Conclusions
In conclusion, the management of root canal curvature presents multifaceted challenges, including complications such as apical blockages, ledges, transportation, and file separations. Our novel technique not only enhances access and control but also contributes to better overall management and leading to better treatment outcomes.
The selection of appropriate tools and techniques is of paramount importance in successfully managing complex cases and achieving predictable results.
Bibliography
-Chaniotis A , Ordinola-Zapata R. Present status and future directions: Management of curved and calcified root canals. International endodontic journal. Int Endod J. 2022 3:656-684
-Elayouti A, Dima E, Judenhofer, M.S., Löst C & Pichler BJ . Increased apical enlargement contributes to excessive dentin removal in curved root canals: a stepwise microcomputed to-mography study. J Endod. 2011;37(11):1580-4
- R. C. Hartmann M, Fensterseifer O, A. Peters J. A. P. de Figueiredo, M. S. ,Gomes G. Rossi-Fedele. Methods for measurement of root canal curvature: a systematic and critical review. Int Endod J. 2019;52(2):169-180
- Estrela c, Bueno M, Damião SOUSA-NETO M, Djalma PÉCORA. Method for Determination of Root Curvature Radius Using Cone-Beam Computed Tomography Images. Braz Dent J. 2008;19(2):114-8
- Schilder H. Cleaning and shaping the root canal. Dent Clin North Am. 1974;18(2):269-96
-Ruddle C. Cleaning and shaping the root canal system. In: Cohen S, Burns R, editors. Pathways of the Pulp. 8th ed. St. Louis, MO: Mosby; 2002



