Management of molarized premolar with severly calcified and curved canals
06/06/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
This article clarifies how to deal with extra root canal system anatomy of premolars clinically and how you can manage and shape the buccal tinny and curved canals of molarized premolar with simple technique by using an handpiece with manual files in reciprocation motion.
Endodontic treatment success is dependent on thorough debridement and full obturation of the whole root canal system. A solid knowledge of root canal space anatomy is a basic requirement for the effective completion of endodontic therapy, especially when more root canals are anticipated. Extra roots and canals must be identified and negotiated with extreme caution especially when it is curved. One of the most difficult challenges for dentists is providing effective endodontic therapy for a maxillary second premolar because the root and canal systems of these teeth vary greatly between racial and ethnic groups. Although three-rooted maxillary premolars are uncommon, extra roots or canals should be considered to ensure successful endodontic therapy. Vertucci found an incidence of 1% of maxillary second premolars with three canals while Pecora et al reported 0.3%. There are few case reports in the literature which reported the occurrence of three rooted maxillary second premolars.

Fig. 1
Pre-op X-Ray showed upper second premolar with poorly restored amalgam with distal cavitation with fast break phenomenon.
In this type of configuration there is expection of extra anatomy
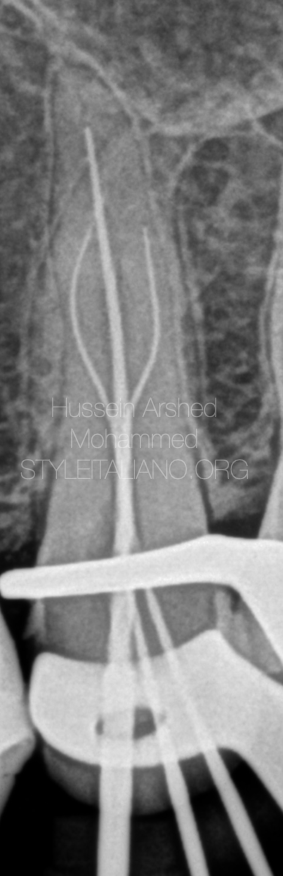
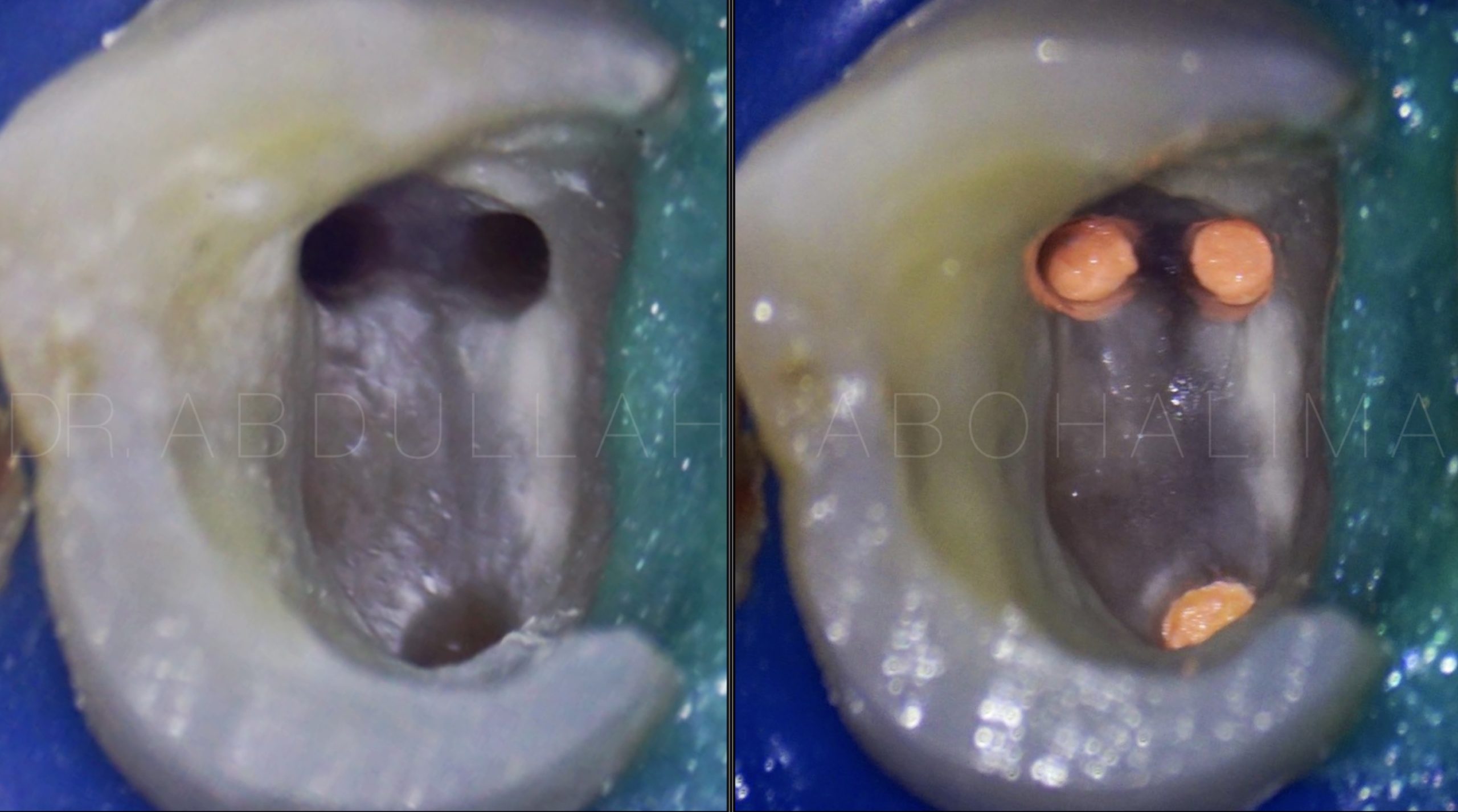
Fig. 2
Negotiation of the canals.
There is one palatal and one buccal orifices.
The buccal orifice splits in the middle third into one mesiobuccal canal and one distobuccal canal.
The buccal canals were very tinny and had multiple curves.
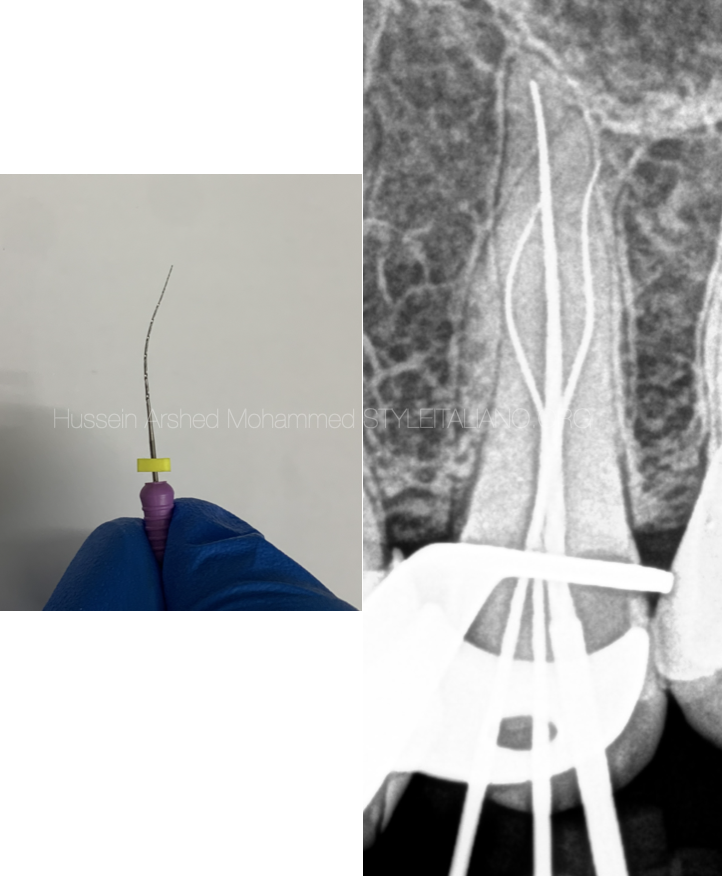
Fig. 3
Trying to reach the full working length with D finder files #10, very difficult to negotiate especially in the mesiobuccal canal.
Using the rotary devices is very helpful to get patency, in this case a manual ISO file was adapted in a handpiece that moves it in reciprocation motion.
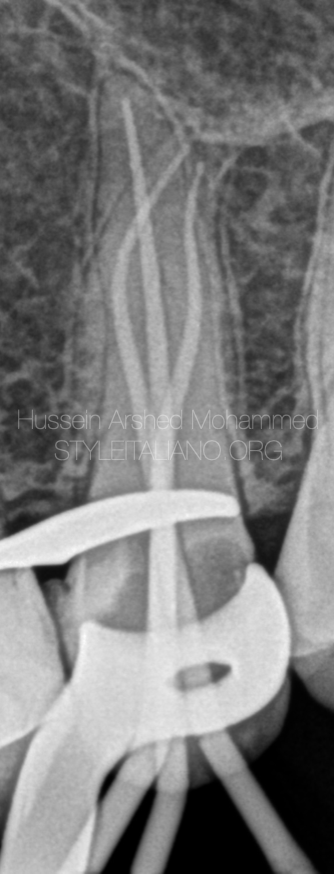
Fig. 4
Shaping till the full working length 30/04 for all the canals and master apical cone confirmed.
The shaping protocol :-
- coronal flaring with orifice opener file
- k- file # 10.
- Rotary file 10/04
- Rotary file 15/03
- Rotary file 17/04
- Rotary file 25//04
- Rotary file 30/04
With copious amount of NaOCl 5.25% between each file.

Fig. 5
Post-op X-Ray with final restoration.
Conclusions
Knowledge of basic root canal anatomy and abnormalities from what is standard is essential for nonsurgical root canal treatment to be successful. Endodontic management of complex root canal anatomy can benefit greatly from careful interpretation of radiographs, access refinement, and evaluation of the pulpal floor under magnification.
Bibliography
1. Rodig T, Hulsmann M. Diagnosis and root canal treatment of a mandibular second premolar with three root canals. Int Endod J. 2003;36:912–9.
2. Sikri VK, Sikri P. Mandibular premolars: aberrations in pulp space morphology. Indian J Dent Res. 1994;5:9–14.
3. Mushtaq M, Farooq R, Rashid A, Robbani I. Spiral computed tomographic evaluation and endodontic management of a mandibular first molar with three distal canals. J Conserv Dent. 2011;14:196–8.
4. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58:589–99.
5. Chauhan R, Singh S. Endodontic management of three-rooted maxillary second premolar in a patient with bilateral occurrence of three roots in maxillary second premolars. Journal of clinical and experimental dentistry. 2012 Dec;4(5):e317