Management of mandibular first premolars with unique anatomies
16/08/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
A thorough knowledge of root canal anatomy is essential for predictable and successful outcomes of endodontic therapy.
Mandibular premolars are rightly called “endodontist’s enigma” by Slowey, as they are known to exhibit a high degree of variability in their root canal morphology, as compared to other teeth in the oral cavity.
These anatomical variations could be in the form of deep splitting canals or a canal ending in multiple portals of exit.
Their unpredictable anatomy, coupled with difficulty in visualizing, accessing and negotiating splitting canals can add to the challenge in dealing with such teeth.
Owing to these reasons, a study by the University of Washington showed mandibular first premolars to have the highest failure rate of 11.4%.
The pre-operative IOPA xray is the most basic diagnostic pre-requisite and can provide an arbitrary blueprint for the root canal anatomy.
The clinician should be aware of the “fast break” appearance which is usually seen as a sudden disappearance of a canal along its course and is a tell- tale sign of canal division.
CBCT can offer a 3 dimensional orientation of the spatial positioning of the canals and the exact level of intra-canal division.
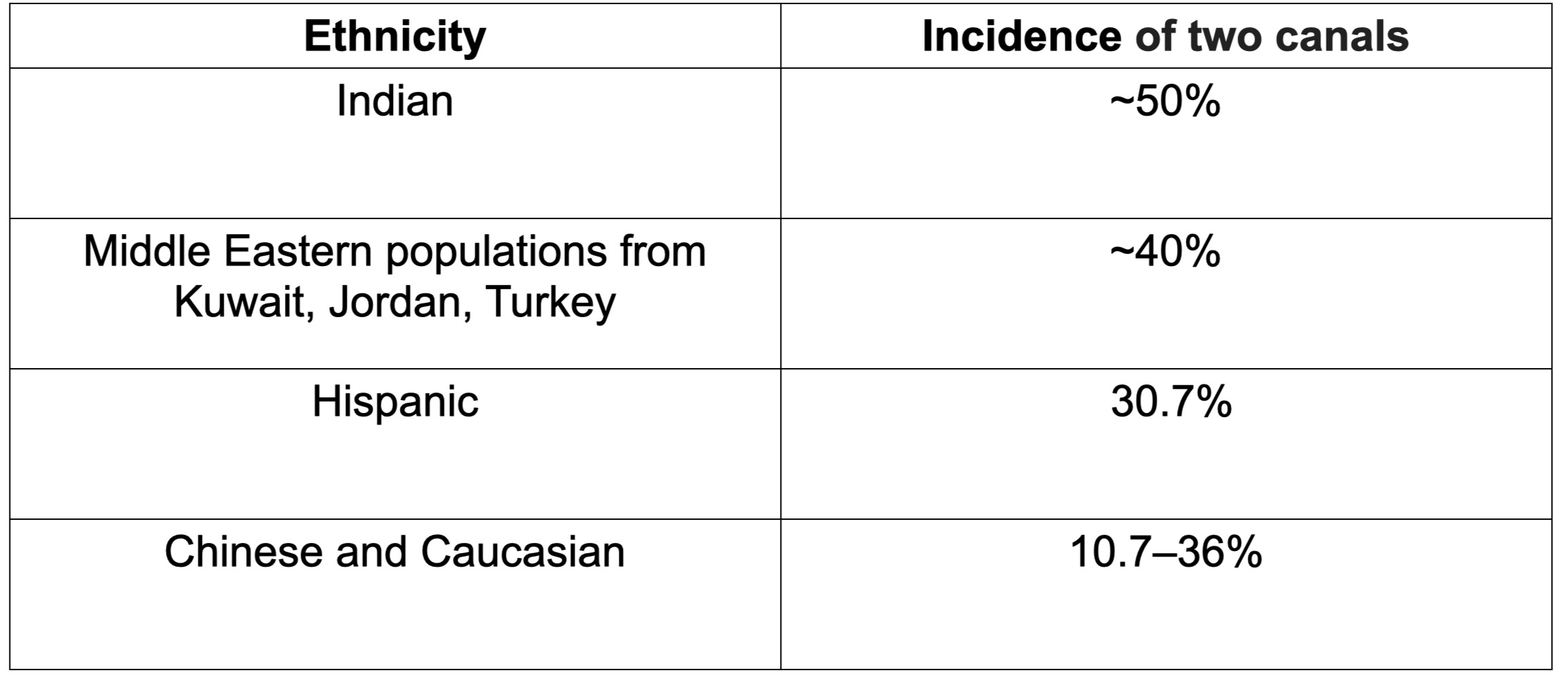
Fig. 1
Systematic Review by Kotoor et al. (2013) stated the following incidences in mandibular first premolars:
- 1 root in 97.21%
- 2 canals in 23.55%
- 3 or more canals in 0–5%.
They also stated the incidence of two canals in mandibular first premolars according to ethnicity (insert table)
This case report describes the diagnosis and non-surgical endodontic treatment of 2 mandibular premolars with two and three canals.

Fig. 2
Case 1:
Pre-operative clinical scenario in mandibular left first premolar (tooth 34) with deep class V defect, dislodged restoration and severe nocturnal and spontaneous pain.
Patient was diagnosed with symptomatic irreversible pulpitis after pulp sensibility testing.

Fig. 3
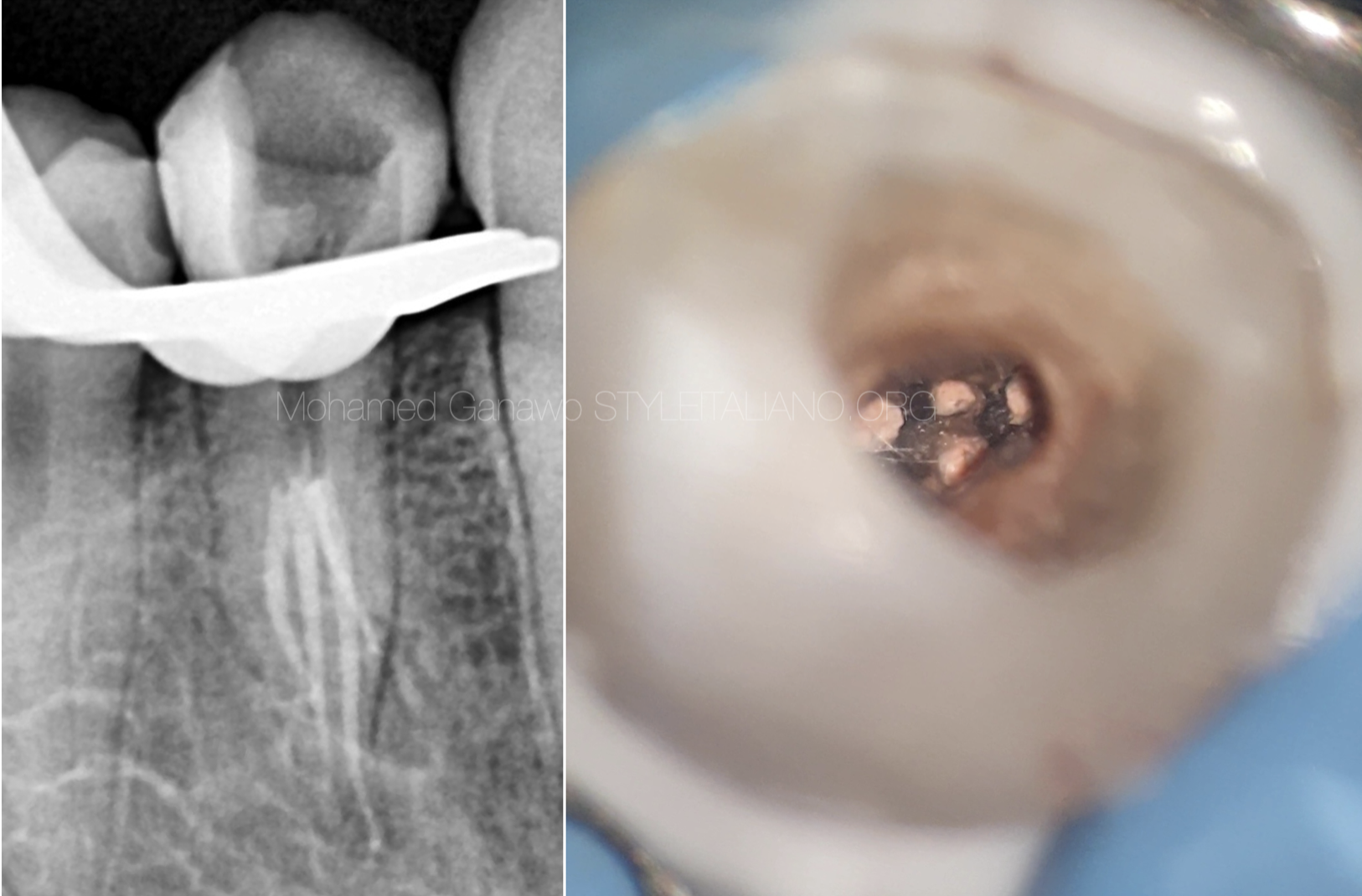
Pre-operative IOPA of tooth 34
“Fast break appearance” seen in the middle third of the root.
Single canal leaving the pulp chamber continuing till middle third, then bifurcating in 2 canals with 2 separate portals of exit.

Fig. 4
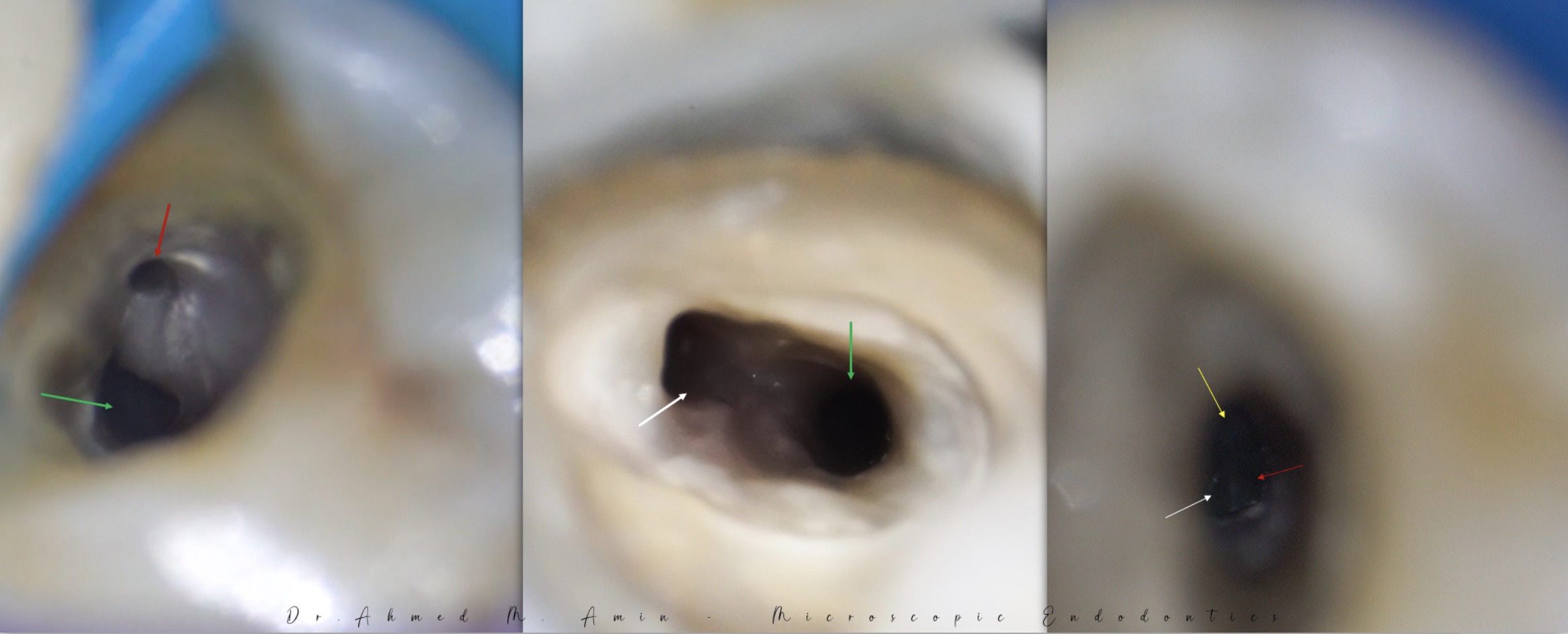
Clinical image showing 2 canals in bucco-lingual orientation at level of split in middle third.
2 canals- buccal (B) and lingual (L).

Fig. 5
Master cone fit radiograph
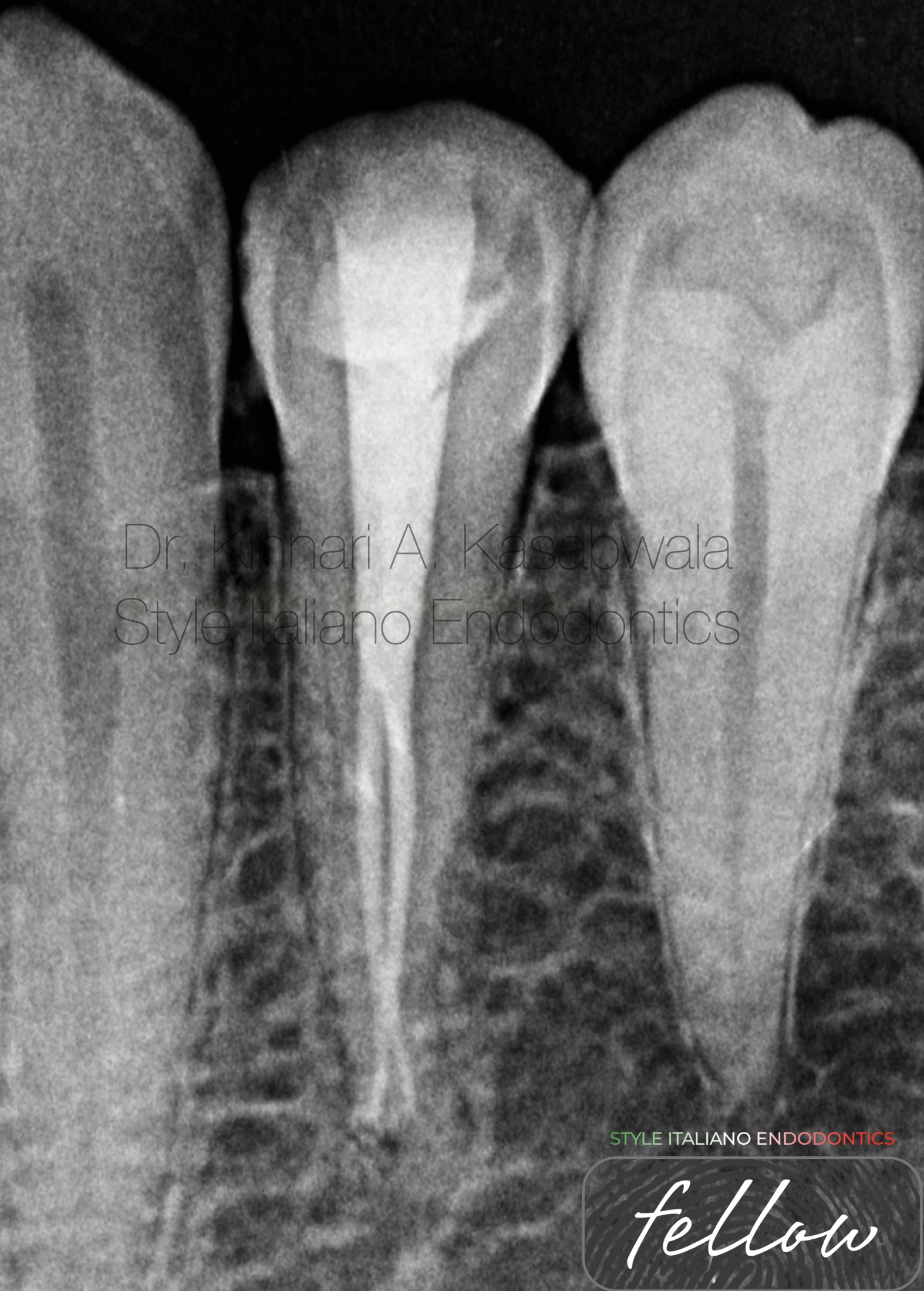
Fig. 6
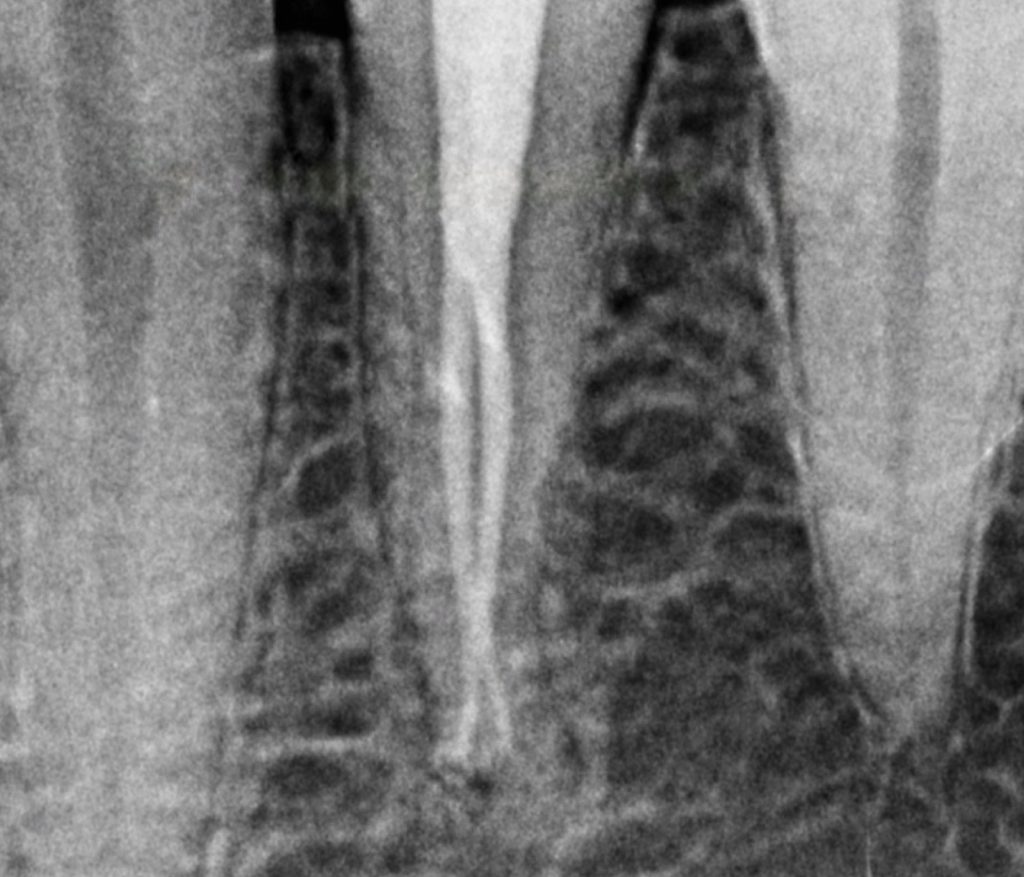
Post- obturation radiograph
Vertucci type VII anatomy (1-2-1-2):
1 canal leaving the pulp chamber continuing till middle third, then bifurcating in 2 canals, anastomosing again in the apical third as an isthmus, finally exiting as 2 canals with 2 separate portals of exit.
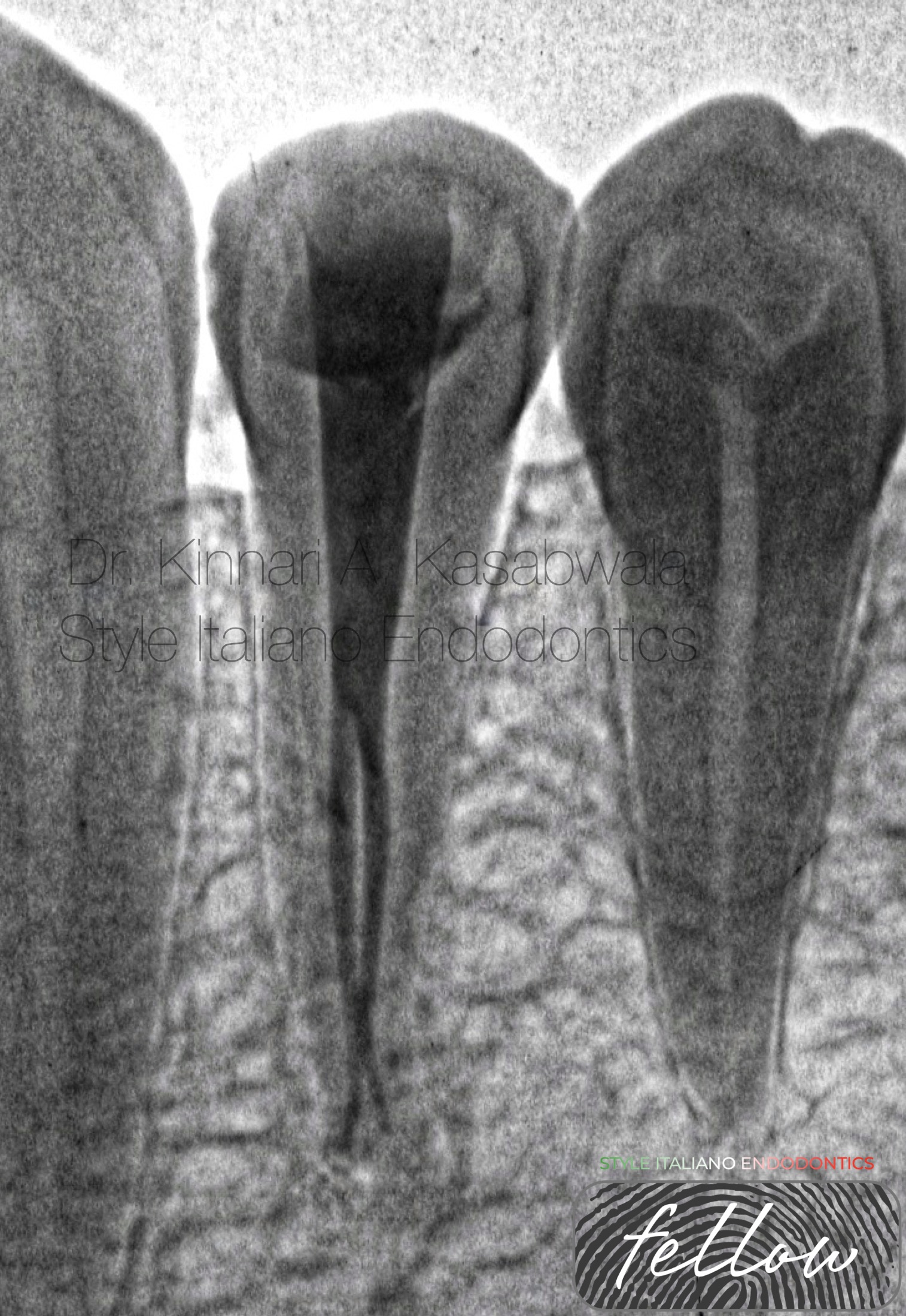
Fig. 7
Post- obturation radiograph (inverted)
Pre-requisites:
- Comprehensive pre-operative evaluation using multi- angled radiographs and/or CBCT
- Magnification- dental operating microscope or loupes
- Isolation-rubber dam
- 6,8,10 size K files
- Flexible NiTi files
- Downpack and backfill obturation system
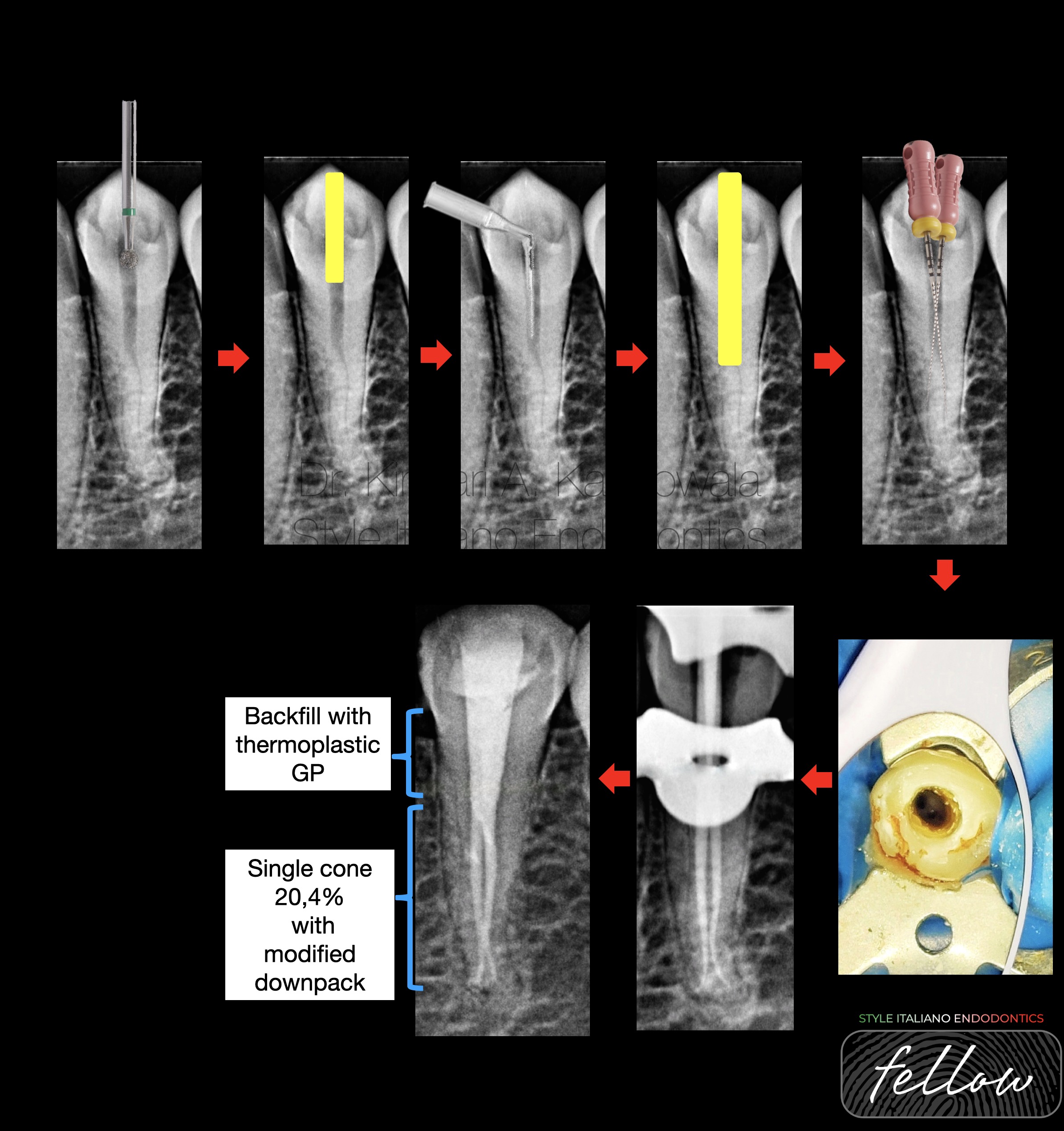
Fig. 8
Sequential steps in negotiating a premolar with bifurcated split
- Use round bur to access the pulp chamber
- Deroof using ultrasonic tip (start X2, Satellac)
- Refinement of the canal till the level of bifurcation using ultrasonic tip (start X3, Satellac)
- Insertion of DG 16 probe tip to “catch” the orifices and further refinement in bucco-lingual direction to de-roof orifices if necessary.
- Insertion of pre-bent 6K files one at a time into the orifices at the level of split
- Enlargement of canal orifices and removal of coronal interferences at the level of split.
- Negotiation of canals till apex with hand files with gentle watch winding motion followed by rotary files
- Selection of master GP cones
- Hybrid obturation with modified downpack till the level of split followed by backfilling with thermoplastic GP till CEJ.
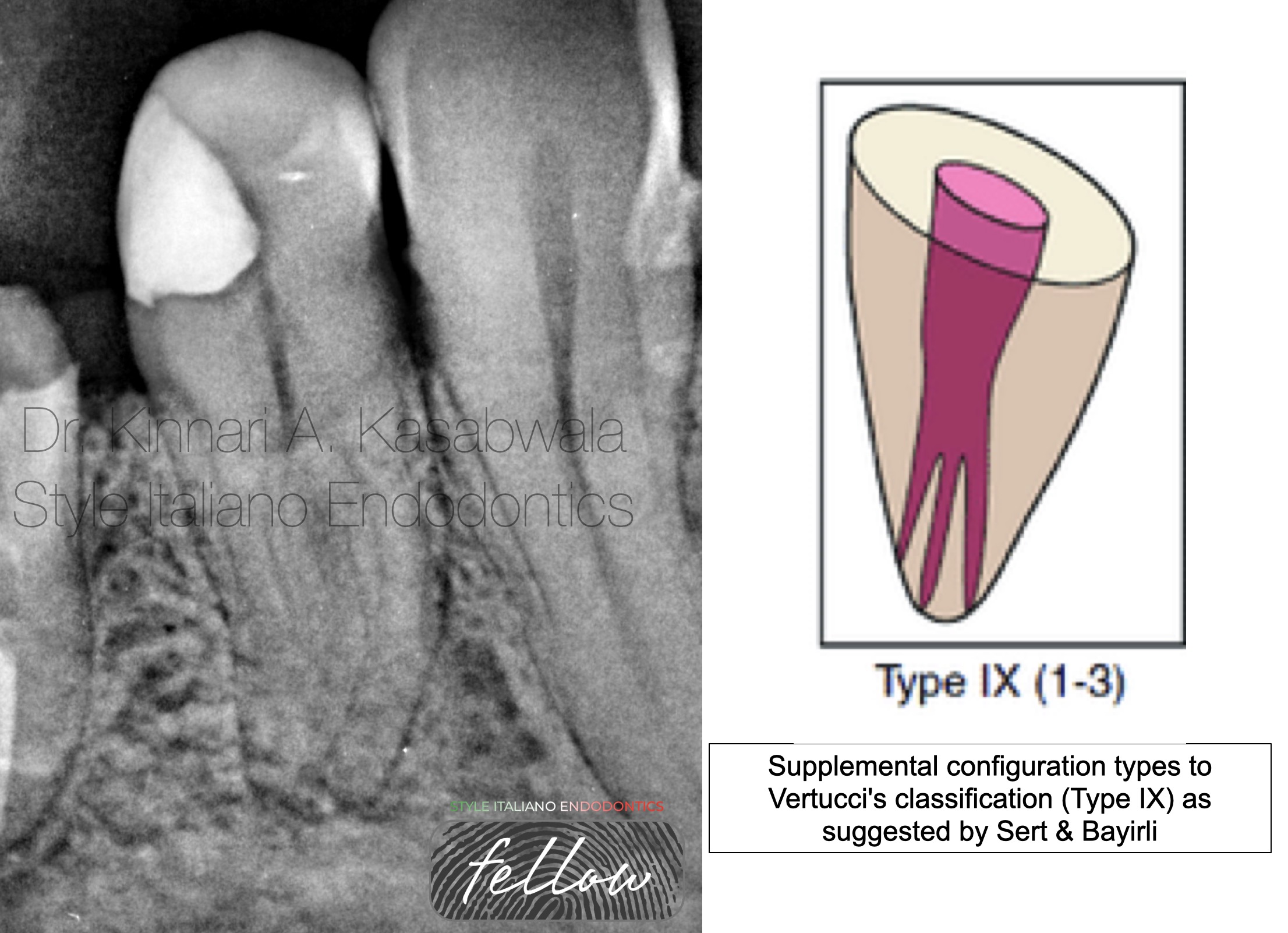
Fig. 9
Case 2:
Patient presented with spontaneous throbbing pain and pain on chewing.
H/O deep restoration 2 months ago.
Diagnosis: symptomatic irreversible pulpitis with symptomatic apical periodontitis.
“Fast break” appearance seen in the end of cervical third in pre-operative IOPA.
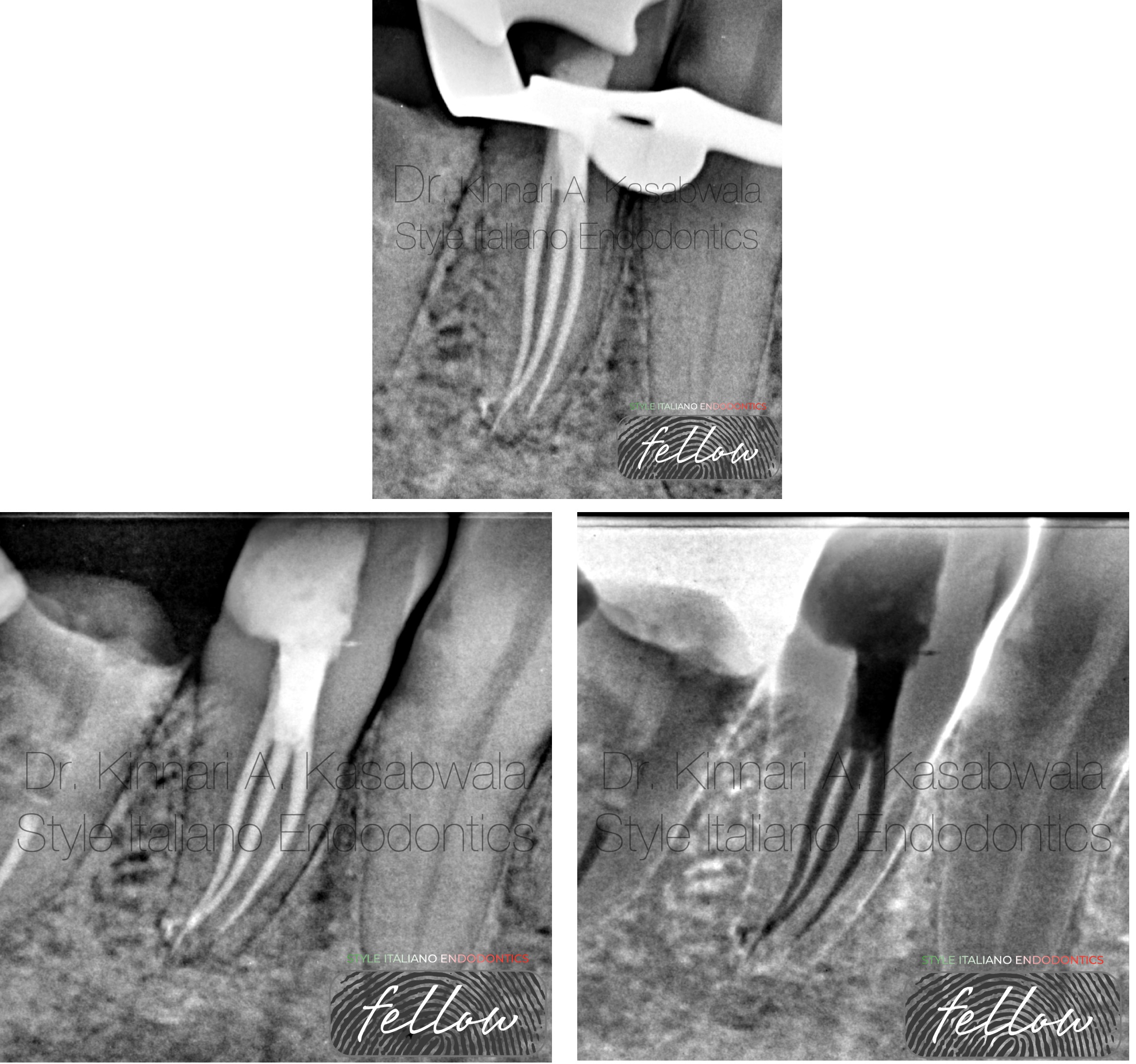
Fig. 10
Supplemental configuration types to Vertucci's classification (Type IX) as suggested by Sert & Bayirli:
1 canal leaving the pulp chamber continuing till beginning of middle third, then trifurcating in 3 canals and exiting as 3 separate portals of exit.
3 separate root outlines seen apically.
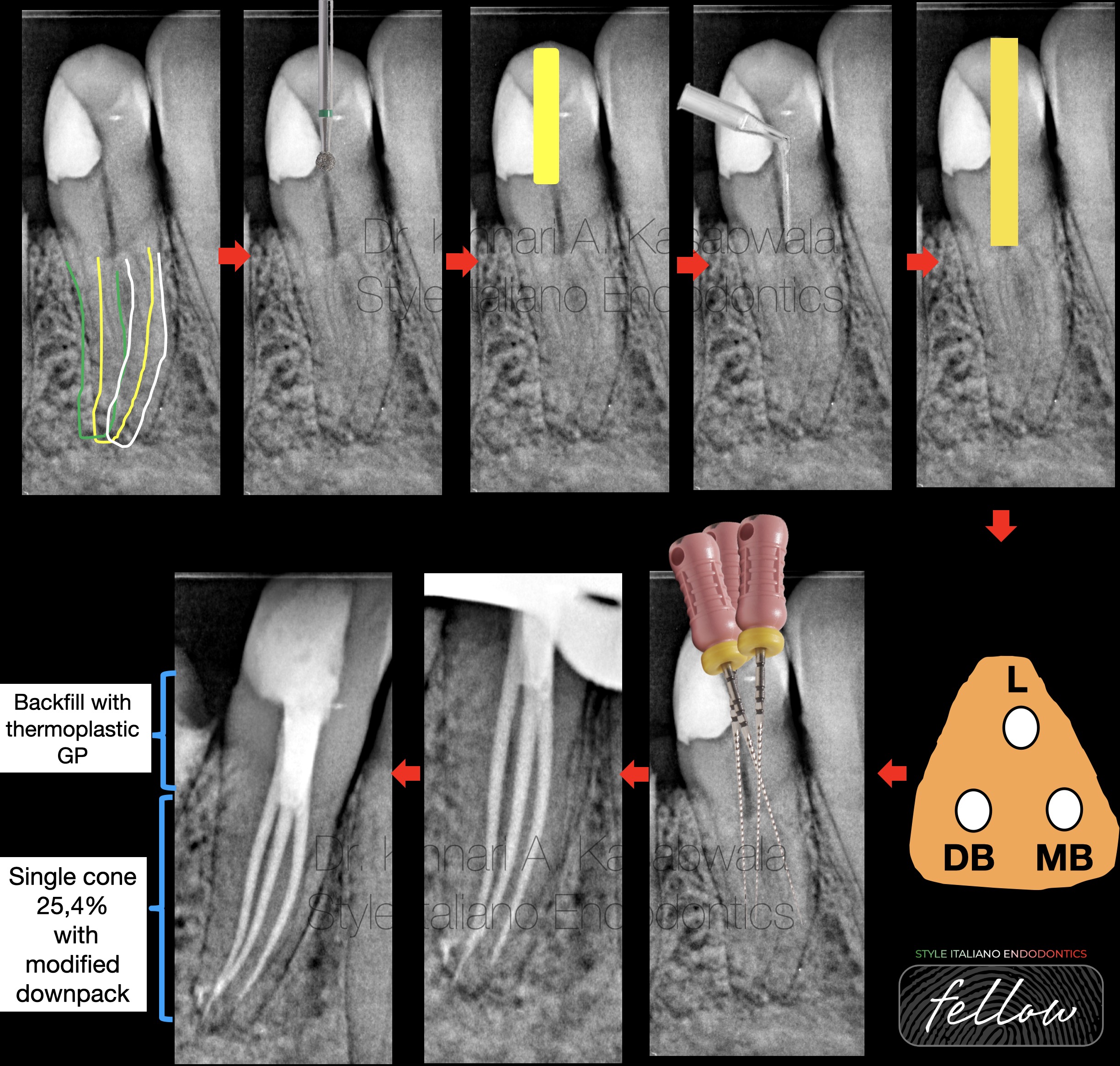
Fig. 11
Sequential steps in negotiating a premolar with trifurcated split
- Trace the root outline to ascertain the number of roots and corresponding root canals.
- Use round bur to access the pulp chamber
- Deroof using ultrasonic tip (start X2, Satellac)
- Refinement of the canal till the level of trifurcation using ultrasonic tip (start X3, Satellac)
- Triangular shaped platform should be aimed for when considering a trifurcation.
- Insertion of DG 16 probe tip to “catch” the orifices and further refinement in bucco-lingual and mesio-distal direction to de-roof orifices if necessary.
- Insertion of pre-bent 6K files one at a time into the orifices at the level of split
- Enlargement of canal orifices and removal of coronal interferences at the level of split.
- Negotiation of canals till apex with hand files with gentle watch winding motion followed by rotary files
- 10.Selection of master GP cones
- 11.Hybrid obturation with modified downpack till the level of trifurcation followed by backfilling with thermoplastic GP till CEJ.

Fig. 12
About Dr. Kinnari Kasabwala
- B.D.S. from Nair hospital dental college, Mumbai (2011-2016)
- M.D.S. specializing in Conservative dentistry and Endodontics from Meenakshi Ammal dental college and hospital, MAHER University, Chennai (2017-2020)
She is awarded with the following:
- "Emerging star 2019" for being the outstanding postgraduate by Conservative dentistry and endodontics association of Tamil Nadu
- Selected as top finalist at the National level in Endodontics for "Young Achiever award 2020" by Indian association of conservative dentistry and endodontics IACDE.
- Gold medal from MAHER university for securing first position in MDS final examination.
- "Best outgoing student" for year 2020 by Conservative dentistry and endodontics department of Meenakshi Ammal dental college and hospital, Chennai
- Awarded "Best student of the year" for years 2017-2018, 2018-2019, 2019-2020 amongst the post graduate students at Endodontics department Meenakshi Ammal dental college and hospital
She is a patent holder of "Indigenous cost-effective biofilm flow cell model and bubble trap" under Intellectual property India, Government of India.
She has authored and co-authored several publications in National and International journals.
She is recently inducted as a national key opinion leader with Bombay dental surgical.
She is recently inducted as a fellow with Style Italiano endodontics forum from May 2023.
Dr. Kinnari Kasabwala is currently practising as a private practioner, specializing in micro-endodontics at Dr Kasabwala dental speciality clinic in Mumbai.
Her interests are Endodontics, Dental aesthetic procedures and multi-disciplinary dentistry.
Conclusions
CONCLUSION:
The endodontic treatment of mandibular premolars with atypical canal configurations can be diagnostically and technically challenging.
They are the most under-estimated teeth with unfortunately, the maximum failure rate in endodontic treatment.
While dealing with premolars with complex anatomies, the clinician’s skill set and patience will be put to the test.
Sound knowledge of normal and aberrant anatomy , correct diagnosis, proper armamentarium and technique can allow the clinician to obtain successful and predictable outcomes.
Bibliography
Bibliography references
Slowey RR. Root canal anatomy. Road map to successful endodontics. Dental Clinics of North America. 1979;23(4):555–573.
Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58:589-99
Ingle J, Bakland L. Endodontics. 5th ed. Hamilton: B C Decker; 2002
Albuquerque D, Kottoor J, Hammo M. Endodontic and clinical considerations in the management of variable anatomy in mandibular premolars: a literature review. Biomed Res Int. 2014;2014:512574
Kottoor J, Albuquerque D, Velmurugan N, Kuruvilla J. Root anatomy and root canal configuration of human permanent mandibular premolars: a systematic review. Anat Res Int. 2013;2013:254250.